

Anatomy & Biomechanics - Anatomy's Tightrope Act
- Glenohumeral Joint (GHJ): Inherently unstable; relies on static & dynamic stabilizers.
- Static Stabilizers:
- Glenoid: Shallow; retroversion 2-7°.
- Labrum: Fibrocartilage, deepens glenoid.
⭐ Labrum increases glenoid depth by ~50%.
- Ligaments:
- SGHL: Resists inferior translation (adducted).
- MGHL: Limits ER at 0-45° abd. (📌 MGHL May Go Hiding - often variable).
- IGHLC: Main anterior stabilizer in ABER position (90° abd. + ER).
- Negative intra-articular pressure.
- Dynamic Stabilizers:
- Rotator Cuff (SITS): Compresses humeral head.
- Long Head of Biceps (LHB): Depresses head.
- Scapulothoracic rhythm.

Classification & Lesions - Decoding the Wobble
- Etiology: Traumatic, Atraumatic, Microtraumatic (repetitive).
- Direction: Anterior, Posterior, Inferior (Luxatio erecta), Multidirectional (MDI).
- Severity: Dislocation (complete) vs. Subluxation (partial).
⭐ Anterior instability is the most common type (approx. 95%).
| Feature | TUBS | AMBRI |
|---|---|---|
| Etiology | Traumatic | Atraumatic |
| Direction | Unidirectional (usually Anterior) | Multidirectional |
| Pathology | Bankart lesion | Often bilateral, capsular laxity |
| Treatment | Surgery (often required) | Rehabilitation (primary), Inferior capsular shift (if surgery) |
| 📌 Mnemonic | Torn Loose, Bankart, Surgery | Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift |
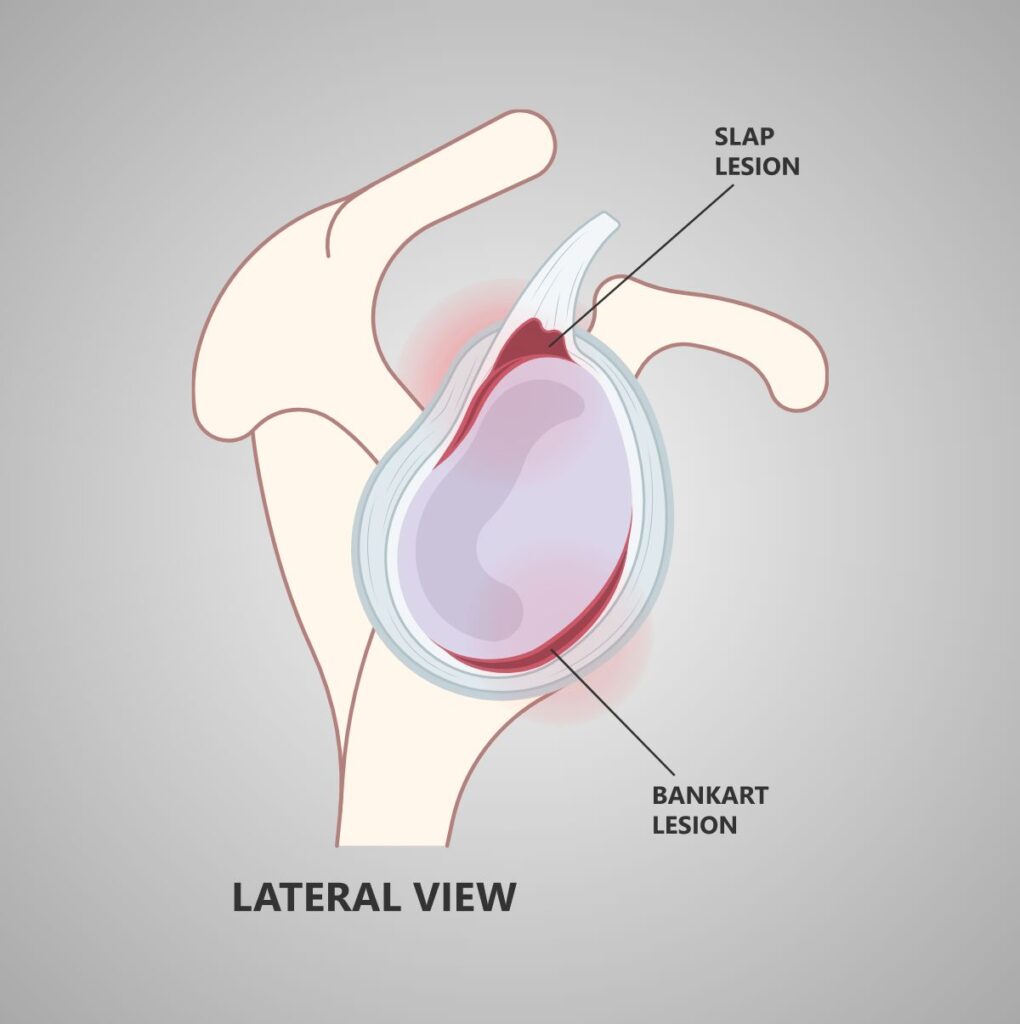
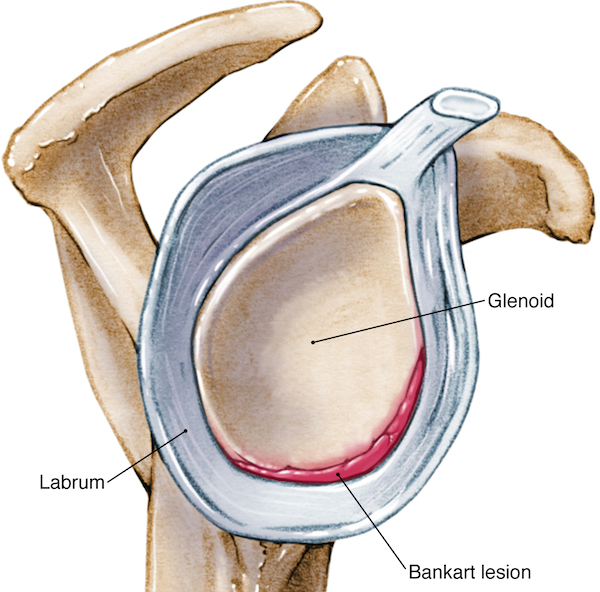
- **Bankart Lesion**: Anteroinferior labrum & IGHL detachment.
+ Bony Bankart: Involves glenoid rim fracture.
- **Hill-Sachs Lesion**: Posterolateral humeral head impaction fracture.
- ALPSA: Anterior Labrum Periosteal Sleeve Avulsion.
- HAGL: Humeral Avulsion of Glenohumeral Ligament.
- SLAP: Superior Labrum Anterior-Posterior tear.
Diagnosis & Evaluation - Clinical Detective Work
- History: Mechanism (FOOSH, direct blow, overuse), prior dislocations, pain, clicking, "dead arm" sensation. Differentiate TUBS vs. AMBRI.
- Examination: Observe (asymmetry, atrophy), palpate key structures, assess active/passive ROM. Neurovascular status crucial.
Loading diagram…
- Special Tests:
Test Category Key Tests Anterior Instability Apprehension, Relocation, Surprise Posterior Instability Posterior Drawer, Jerk Test Inferior Instability Sulcus Sign (Grades +1/+2/+3) Labral/SLAP O'Brien's, Crank Test - Imaging:
- X-rays: AP, Grashey, Axillary lateral. Consider West Point (bony Bankart), Stryker Notch (Hill-Sachs).
⭐ The West Point axillary view is best for imaging a bony Bankart lesion.
- MRI/MR Arthrogram: Gold standard for labral tears, capsular injury, RTC.
Management Principles - Fixing the Flux
- Goal: Restore stability & function; prevent recurrence & arthropathy.
- Conservative Management (Often first-line):
- Immobilization (sling for comfort, brief duration).
- Physiotherapy: Key for AMBRI. Focus on rotator cuff, deltoid, and scapular stabilizer strengthening.
- Activity modification.
- Surgical Management (Indications vary by instability type):
- TUBS: Often requires surgery after first dislocation in high-demand individuals or for recurrence.
- Arthroscopic Bankart Repair: For labral tears without significant bone loss.
- Latarjet Procedure: For significant glenoid bone loss >20-25% or failed soft-tissue repair.
- AMBRI: Surgery (e.g., capsular shift/plication) if extensive physiotherapy fails.
- 📌 Mnemonic (Instability Types & Treatment Bias):
- TUBS: Traumatic, Unidirectional, Bankart lesion, Surgery often needed.
- AMBRI: Atraumatic, Multidirectional, Bilateral, Rehabilitation (primary), Inferior capsular shift (if surgery).
- TUBS: Often requires surgery after first dislocation in high-demand individuals or for recurrence.
Loading diagram…
⭐ Latarjet procedure is indicated for recurrent anterior instability with significant glenoid bone loss (typically >20-25%) or failed previous soft tissue repairs.
High‑Yield Points - ⚡ Biggest Takeaways
- Anterior instability (95%) is most common, from abduction & external rotation.
- Bankart lesion (anteroinferior labral tear) is pathognomonic for traumatic anterior instability.
- Hill-Sachs lesion (humeral head impaction) often co-exists with Bankart.
- Key acronyms: TUBS (Traumatic, Unidirectional, Bankart, Surgery) & AMBRI (Atraumatic, Multidirectional, Bilateral, Rehabilitation).
- Tests: Apprehension, Relocation (anterior); Sulcus sign (inferior/MDI).
- High recurrence of traumatic dislocations in young, active patients.
- Posterior instability often follows seizures/electric shock.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more