

Microbiology & Pathogenesis - The Clap's ID
- Organism: Neisseria gonorrhoeae, a Gram-negative diplococcus.
- Key Features:
- Often intracellular (within neutrophils).
- Aerobic, oxidase-positive.
- Major Virulence Factors (📌 POPLI):
- Pili: Attachment to mucosa; high antigenic variation.
- Opa proteins: Adhesion, invasion into host cells; antigenic variation.
- Por proteins (Porins): Outer membrane channels; prevent phagolysosome fusion.
- LOS (Lipooligosaccharide): Endotoxin; triggers inflammation, tissue damage.
- IgA protease: Cleaves IgA1, aids mucosal colonization.
⭐ Antigenic variation in pili and Opa proteins contributes to immune evasion and repeat infections.

Clinical Manifestations - Gonorrhea's Gallery
Incubation period: 2-7 days.
- Urogenital (Male):
- Acute urethritis: dysuria, purulent discharge.
- Complications: epididymitis, prostatitis.
- Urogenital (Female):
- Cervicitis: often asymptomatic; mucopurulent discharge.
- Urethritis.
- Risk of Pelvic Inflammatory Disease (PID).
- Anorectal:
- Proctitis: often asymptomatic; features include pain, discharge, tenesmus.
- Pharyngeal:
- Pharyngitis: often asymptomatic; sore throat.
- Ophthalmia Neonatorum:
- Conjunctivitis in newborns: purulent discharge.
- Can lead to blindness; prophylaxis (e.g., erythromycin ointment) vital.
- Disseminated Gonococcal Infection (DGI): Bacteremia.
- Two main forms:
Syndrome Features Arthritis-Dermatitis Syndrome Fever, tenosynovitis, polyarthralgia, skin lesions (pustular/hemorrhagic) Septic Arthritis Purulent monoarthritis or oligoarthritis - 📌 Mnemonic (Arthritis-Dermatitis): JST - Joints, Skin, Tendons.
- Two main forms:
⭐ Asymptomatic infection is common, especially in women (cervicitis) and pharyngeal/rectal sites, making screening crucial in high-risk populations.
Diagnostic Approach - Spotting the Culprit
- Specimens: Urethral, endocervical/vaginal, urine (1st void), pharyngeal/rectal swabs, synovial fluid, blood (DGI).
- Microscopy (Gram Stain): Gram-negative intracellular diplococci (GNID). >95% Sens. in symptomatic male urethritis.
- Culture: Thayer-Martin (MTM) selective media (📌 VCNT: Vancomycin, Colistin, Nystatin, Trimethoprim). For antimicrobial susceptibility (AST).
- NAATs (Nucleic Acid Amplification Tests): Highest Sens/Spec. Preferred. No AST.
⭐ NAATs are the diagnostic test of choice for gonorrhea due to their high sensitivity and ability to use non-invasive samples like urine, but culture is essential for antimicrobial susceptibility testing.
Diagnostic Tests Comparison:
| Test | Sample(s) | Features | Use |
|---|---|---|---|
| Gram Stain | Urethral (♂), Endocervical | GNID. >95% Sens (symp. ♂ urethritis) | Rapid presumptive (symp. ♂) |
| Culture | Swabs, Urine | Thayer-Martin (VCNT). Allows AST. | Definitive Dx, AST |
| NAATs | Urine, Swabs | Highest Sens/Spec. No AST. | Preferred Dx/screening |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |||
| flowchart TD |
Start["<b>🩺 Suspected GC</b><br><span style='display:block; text-align:left; color:#555'>• N. gonorrhoeae</span><span style='display:block; text-align:left; color:#555'>• Clinical suspicion</span>"]
Assess["<b>📋 Assess Patient</b><br><span style='display:block; text-align:left; color:#555'>• Symptomatic male?</span><span style='display:block; text-align:left; color:#555'>• Urethritis signs?</span>"]
Gram["<b>🔬 Gram Stain</b><br><span style='display:block; text-align:left; color:#555'>• Look for GNID</span><span style='display:block; text-align:left; color:#555'>• >95% sensitivity</span>"]
Treat["<b>💊 Treatment</b><br><span style='display:block; text-align:left; color:#555'>• Direct therapy</span><span style='display:block; text-align:left; color:#555'>• Culture if needed</span>"]
NaatCult["<b>🔬 Diagnosis</b><br><span style='display:block; text-align:left; color:#555'>• NAAT or Culture</span><span style='display:block; text-align:left; color:#555'>• Extragenital/Asx</span>"]
NaatPref["<b>✅ NAAT Result</b><br><span style='display:block; text-align:left; color:#555'>• Preferred method</span><span style='display:block; text-align:left; color:#555'>• High Sens/Spec</span>"]
AstCult["<b>🔬 AST Culture</b><br><span style='display:block; text-align:left; color:#555'>• Susceptibility</span><span style='display:block; text-align:left; color:#555'>• Resistance check</span>"]
Start --> Assess
Assess -->|Yes| Gram
Assess -->|No/Asx| NaatCult
Gram -->|Positive| Treat
Gram -->|Neg/Equiv| NaatCult
NaatCult --> NaatPref
NaatCult -->|If AST needed| AstCult
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8
style Assess fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E
style Gram fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C
style Treat fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534
style NaatCult fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C
style NaatPref fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
style AstCult fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C
## Treatment & Complications - Gonorrhea's Gauntlet
* **Antimicrobial Resistance:** A major concern; monitor local patterns.
* **Uncomplicated Gonorrhea** (Urogenital, Rectal, Pharyngeal):
- **Ceftriaxone 500 mg IM** (or **1g IM** if body weight ≥150 kg) single dose.
- PLUS (if chlamydia not excluded): **Doxycycline 100 mg** orally BID for **7 days**.
- Pharyngeal: Test-of-cure (NAAT/culture) **7-14 days** post-treatment.
* **Disseminated Gonococcal Infection (DGI):**
- Hospitalization.
- **Ceftriaxone 1g IV/IM q24h** for **7 days** (initial parenteral, then oral).
* **Ophthalmia Neonatorum:**
- Treatment: **Ceftriaxone 25-50 mg/kg IV/IM** (max **125 mg**) single dose.
- Prophylaxis: Erythromycin 0.5% ophthalmic ointment.
* **Partner Management:**
- Treat partners from last **60 days**.
- Abstain from sex for 7 days post-treatment (all partners).
* **Complications:**
- Male: Epididymo-orchitis, infertility.
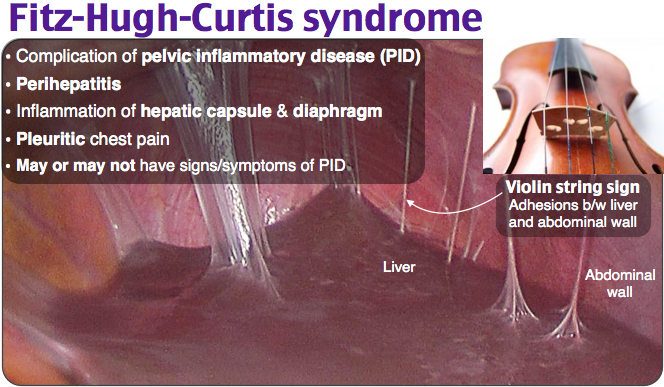
- Female: PID, infertility, ectopic pregnancy, Fitz-Hugh-Curtis syndrome.
* **Prevention:** Condoms, screening, education.
> ⭐ Due to widespread antimicrobial resistance, dual therapy with ceftriaxone and doxycycline (if chlamydia not excluded) is standard for uncomplicated gonorrhea; test-of-cure is recommended for pharyngeal infections.
```mermaid
%%{init: {'flowchart': {'htmlLabels': true}}}%%
flowchart TD
Start["<b>🩺 Gonorrhea Dx</b><br><span style='display:block; text-align:left; color:#555'>• Confirm infection</span><span style='display:block; text-align:left; color:#555'>• Identify sites</span>"]
Case["<b>📋 Select Case</b><br><span style='display:block; text-align:left; color:#555'>• Assess severity</span><span style='display:block; text-align:left; color:#555'>• Clinical type</span>"]
Uncomp["<b>💊 Uncomplicated</b><br><span style='display:block; text-align:left; color:#555'>• Ceftriaxone 500mg</span><span style='display:block; text-align:left; color:#555'>• Add Doxycycline</span>"]
DGI["<b>⚠️ Disseminated</b><br><span style='display:block; text-align:left; color:#555'>• Hospitalize pt</span><span style='display:block; text-align:left; color:#555'>• IV/IM Ceftriaxone</span>"]
Ophthalmia["<b>🔬 Ophthalmia Neon.</b><br><span style='display:block; text-align:left; color:#555'>• Ceftriaxone IM</span><span style='display:block; text-align:left; color:#555'>• Erythro ointment</span>"]
TOC["<b>👁️ Test-of-Cure</b><br><span style='display:block; text-align:left; color:#555'>• Pharyngeal check</span><span style='display:block; text-align:left; color:#555'>• Re-test 7-14d</span>"]
Partners["<b>✅ Shared Steps</b><br><span style='display:block; text-align:left; color:#555'>• Treat partners</span><span style='display:block; text-align:left; color:#555'>• 7d abstinence</span>"]
Start --> Case
Case -->|Uncomplicated| Uncomp
Case -->|Disseminated| DGI
Case -->|Neonatal| Ophthalmia
Uncomp -->|Pharyngeal| TOC
Uncomp --> Partners
DGI --> Partners
Ophthalmia -->|Mother/Partn.| Partners
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8
style Case fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E
style Uncomp fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534
style DGI fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C
style Ophthalmia fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C
style TOC fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1
style Partners fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
High‑Yield Points - ⚡ Biggest Takeaways
- Neisseria gonorrhoeae (Gram-negative diplococcus) is the causative agent.
- Commonest presentations: purulent urethritis in males, cervicitis (often asymptomatic) in females.
- Key complications: Pelvic Inflammatory Disease (PID), epididymo-orchitis, Disseminated Gonococcal Infection (DGI) featuring arthritis-dermatitis syndrome.
- Ophthalmia neonatorum is a serious neonatal infection.
- NAAT is the diagnostic gold standard; Gram stain reveals intracellular diplococci.
- Preferred treatment: Ceftriaxone IM (plus Azithromycin/Doxycycline for Chlamydia co-infection).
- Significant concern: Increasing quinolone and cephalosporin resistance.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more