

Heavy Metals - Lead, Mercury & Arsenic Alerts
- Lead (Plumbism)
- Features: Burton's line (gums), basophilic stippling (RBCs), foot/wrist drop (motor neuropathy), abdominal colic, encephalopathy.
- Enzymes: $\delta$-ALA dehydratase, ferrochelatase (inhibits heme synthesis).
- Chelators: CaNa$_2$EDTA, DMSA (Succimer), BAL (Dimercaprol), D-Penicillamine.
- 📌 Mnemonic "LEAD": Lead lines (gums, bones), Encephalopathy, Anemia, Drop (wrist/foot).
- Mercury
- Forms: Elemental, inorganic, organic (methylmercury - Minamata disease).
- Features: Acrodynia ("pink disease" - children), erethism (tremors, irritability), nephrotic syndrome, gingivostomatitis.
- Chelators: DMSA (Succimer), BAL (Dimercaprol for inorganic Hg; not for methylmercury).
- Arsenic
- Features: Aldrich-Mees lines (nails), garlic odor (breath/stool), "rain-drop" skin pigmentation, peripheral neuropathy, gangrene, pancytopenia.
- Carcinogen: Known human carcinogen (skin, lung, bladder).
- Chelators: BAL (Dimercaprol for acute poisoning), DMSA (Succimer).
⭐ Basophilic stippling of RBCs is a classic, though not pathognomonic, finding in lead poisoning, indicating disrupted erythropoiesis.

Gaseous Foes & Solvent Woes - CO, H2S & More
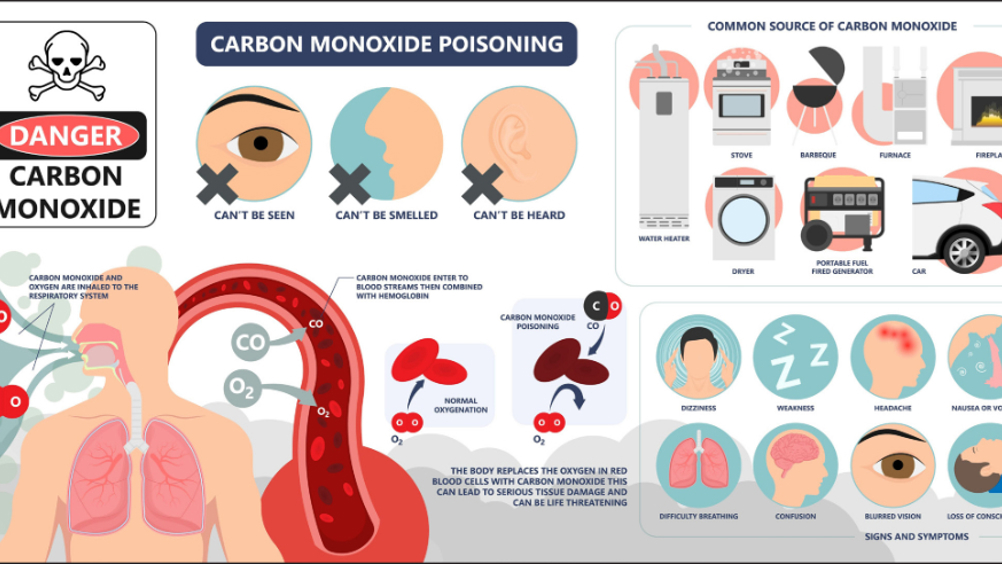
- Carbon Monoxide (CO)
- Sources: Incomplete combustion (fires, exhaust).
- Patho: Binds Hb (COHb, >200x affinity vs O₂), ↓O₂ delivery.
- Sx: Headache (common), nausea. Cherry-red skin (late).
- Dx: ↑COHb levels.
- Rx: 100% O₂; Hyperbaric O₂ (severe: COHb >25%, LOC, neuro/cardiac).
⭐ The most common symptom of acute carbon monoxide poisoning is headache; cherry-red skin is a late and unreliable sign.
Loading diagram…
-
Hydrogen Sulfide ($H_2S$)
- Sources: Decaying organics. Smell: Rotten eggs (low); olfactory paralysis (high).
- Effects: "Knockdown" (>500 ppm). Cellular asphyxiant (cytochrome oxidase inhibitor).
- Rx: Nitrites (sodium/amyl), sodium thiosulfate. Supportive care.
-
Solvent Woes
- Benzene: Aplastic anemia, ↑ AML risk (chronic).
- Organochlorine Solvents:
- $CCl_4$: Hepatotoxic (centrilobular necrosis), nephrotoxic.
- TCE: CNS depression, trigeminal neuropathy, arrhythmias.
Pesticide Perils - OP, OC & Paraquat Pointers
Occupational hazard. Early diagnosis, specific antidotes vital.
- Organophosphates (OP) & Carbamates:
- Mechanism: AChE inhibition (OPs: irreversible, Carbamates: reversible).
- Symptoms: Cholinergic crisis. 📌 DUMBELS: Diarrhea/Diaphoresis, Urination, Miosis, Bronchorrhea/Bronchospasm, Emesis, Lacrimation, Salivation. Muscle weakness.
- Management:
- Atropine: 2-5 mg IV q 5-15 min for muscarinic effects.
- Pralidoxime (PAM): 1-2 g IV for OP. Not for carbamates.
- Organochlorines (OC) (e.g., DDT):
- Mechanism: CNS stimulation (ion channels).
- Symptoms: Seizures, tremors.
- Management: Symptomatic (seizures), decontamination.
- Paraquat:
- Mechanism: Free radical generation, oxidative stress.
- Symptoms: GI upset, renal/hepatic failure. "Paraquat Lung" (pulmonary fibrosis).
- Management: Fuller's earth, charcoal, hemoperfusion. Avoid high O₂.
Loading diagram…
⭐ Pralidoxime (PAM) reactivates AChE, best for nicotinic symptoms in early OP poisoning; not for carbamates.
Dusty Lungs - Silicosis, Asbestosis & CWP Facts
- Silicosis: Exposure to silica dust (sandblasting, mining, quarrying). CXR shows "egg-shell" calcification of hilar lymph nodes. Upper lobe predominance. Increased risk of tuberculosis.
⭐ Egg-shell calcification of hilar lymph nodes on chest X-ray is highly suggestive of silicosis.
- Asbestosis: Exposure to asbestos fibers (shipbuilding, insulation, construction). Features pleural plaques (hallmark), ferruginous bodies. Lower lobe predominance. Increased risk of mesothelioma and lung cancer.
- CWP (Coal Worker's Pneumoconiosis): Coal dust exposure. Simple CWP (anthracosis) or complicated CWP (Progressive Massive Fibrosis - PMF). Associated with Caplan syndrome (CWP + rheumatoid arthritis). Upper lobe predominance.
- Byssinosis: Exposure to cotton, flax, or hemp dust. Characterized by "Monday fever": chest tightness, dyspnea, and cough on the first day back to work, improving through the week.
High‑Yield Points - ⚡ Biggest Takeaways
- Silicosis (sandblasting, mining) shows eggshell calcification of hilar nodes and increases TB risk.
- Asbestosis (shipbuilding, insulation) is linked to pleural plaques, asbestosis bodies, and mesothelioma.
- Lead poisoning (batteries, old paint) causes Burton's line, wrist/foot drop, and basophilic stippling.
- Organophosphate poisoning (pesticides) induces a cholinergic crisis (DUMBELS); antidote: atropine and pralidoxime.
- Carbon monoxide poisoning (incomplete combustion) presents with cherry-red skin/mucosa; treat with 100% O2 or hyperbaric oxygen.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more