

ILD Overview - The Lung Labyrinth
- Definition: Diverse group of diffuse parenchymal lung diseases affecting the interstitium, causing inflammation and/or fibrosis.
- Key Symptoms: Progressive exertional dyspnea, persistent dry cough.
- Key Sign: Bibasilar fine inspiratory crackles ('Velcro rales'). Clubbing possible.
- Basic Pathophysiology: Alveolitis → Chronic Inflammation → Fibrosis → Impaired gas exchange, stiff lungs.
- PFTs: Restrictive pattern: ↓TLC, ↓DLCO; normal or ↑ $FEV_1/FVC$ ratio.
- Broad Classification:
- Known causes: Drugs (amiodarone, bleomycin), CTD (RA, SSc), environmental (asbestosis, silicosis).
- Idiopathic Interstitial Pneumonias (IIPs): e.g., IPF, NSIP.
- Granulomatous: Sarcoidosis, Hypersensitivity Pneumonitis (HP).
- Rare ILDs.

⭐ Bibasilar 'Velcro' crackles are a characteristic auscultatory finding in many ILDs, especially IPF.
IPF - Scarred Scenery
- Most common, severe Idiopathic Interstitial Pneumonia (IIP).
- Affects older adults (>60 yrs), M>F predominance.
- Pathology: Usual Interstitial Pneumonia (UIP) pattern (hallmark: spatial & temporal heterogeneity).
- HRCT Chest (essential for diagnosis):
- Bilateral, basal, subpleural reticulation.
- Honeycomb cysts.
- Traction bronchiectasis.
- Absence of: extensive Ground Glass Opacities (GGO), nodules, consolidation.
- Diagnosis of exclusion: Rule out Connective Tissue Disease (CTD), drug toxicity, chronic Hypersensitivity Pneumonitis (HP).
- Prognosis: Poor; median survival 3-5 years.
- Management:
- Antifibrotics: Pirfenidone, Nintedanib (slow Forced Vital Capacity (FVC) decline).
- Supportive: O2, pulmonary rehabilitation.
- Lung transplant.
- ⭐ > The UIP pattern on HRCT, characterized by subpleural, basal predominant honeycombing, is crucial for IPF diagnosis.
Sarcoidosis - Granuloma Galaxy
- Unknown etiology multisystem disorder; hallmark: non-caseating granulomas.
- Pulmonary involvement: >90% of cases.
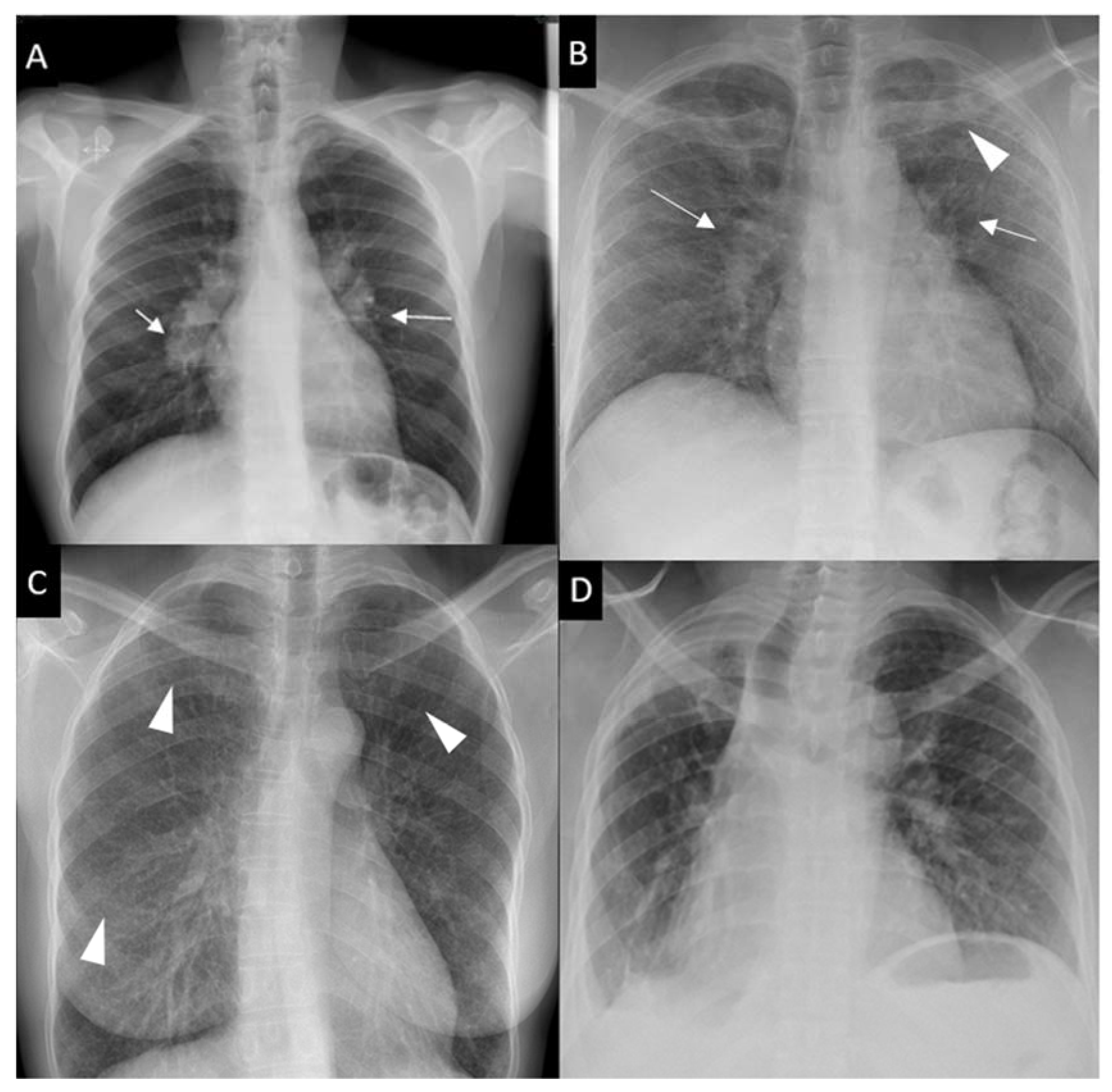
- CXR Staging (Scadding):
Loading diagram…
- Extrapulmonary sites: Skin (erythema nodosum, lupus pernio, maculopapular rash), eyes (uveitis, conjunctivitis), lymph nodes, liver, spleen, heart, nervous system.
⭐ Löfgren's syndrome (acute arthritis, erythema nodosum, and bilateral hilar lymphadenopathy) is an acute form of sarcoidosis with a good prognosis.
- Diagnosis: Compatible clinical/radiological findings + histological evidence of non-caseating granulomas + exclusion of other granulomatous diseases.
- Lab findings: ↑ Serum Angiotensin-Converting Enzyme (ACE) (non-specific, reflects granuloma load). Hypercalcemia/hypercalciuria (due to macrophage $1\alpha$-hydroxylase activity).
Other Key ILDs - Diverse Diffusopathies
- Hypersensitivity Pneumonitis (HP): Immune reaction to inhaled organic antigens (Farmer's lung, Bird fancier's lung).
- Acute, subacute, chronic (can → fibrosis).
- HRCT: Acute/Subacute - centrilobular ground-glass nodules, mosaic attenuation. Chronic - fibrosis.
- Rx: Antigen avoidance, corticosteroids.
- Connective Tissue Disease-Associated ILD (CTD-ILD): Common in Scleroderma (SSc), Rheumatoid Arthritis (RA), Polymyositis/Dermatomyositis (PM/DM).
- Patterns: NSIP (SSc), UIP (RA-ILD, poorer prognosis), OP.
- Pneumoconioses:
- Silicosis: Silica dust. Upper lobe nodules, Progressive Massive Fibrosis (PMF). ↑ TB risk.
⭐ 'Egg-shell' calcification of hilar lymph nodes on chest X-ray is highly suggestive of silicosis.
- Asbestosis: Asbestos fibers. Lower lobe fibrosis, pleural plaques. ↑ risk of lung cancer & mesothelioma.
- Silicosis: Silica dust. Upper lobe nodules, Progressive Massive Fibrosis (PMF). ↑ TB risk.
High‑Yield Points - ⚡ Biggest Takeaways
- IPF: UIP pattern (honeycombing, traction bronchiectasis) on HRCT; treat with Pirfenidone/Nintedanib.
- Sarcoidosis: Non-caseating granulomas, bilateral hilar lymphadenopathy, ↑ACE, hypercalcemia; Lofgren's syndrome.
- Hypersensitivity Pneumonitis: Antigen exposure (farmer's/bird fancier's lung); antigen avoidance is crucial.
- CTD-ILD: Common with scleroderma, RA; NSIP pattern is frequent.
- Pneumoconioses: Occupational dusts (silicosis: ↑TB risk; asbestosis: mesothelioma).
- ILDs show restrictive PFTs (↓TLC, ↓FVC, ↓DLCO); key drug causes: Amiodarone, Bleomycin, Methotrexate.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more