

Hallmarks & Cell Cycle - Cancer's Playbook
- Key Hallmarks of Cancer:
- Sustained proliferative signaling (e.g., oncogene activation)
- Evading growth suppressors (e.g., loss of p53, Rb function)
- Resisting cell death (e.g., anti-apoptotic protein upregulation)
- Enabling replicative immortality (telomerase re-activation)
- Inducing angiogenesis (VEGF signaling)
- Activating invasion & metastasis (EMT process)
- Cell Cycle & Its Dysregulation:
- Phases: G1 (growth) → S (DNA synthesis) → G2 (prep for mitosis) → M (mitosis).
- Regulators: Cyclins (regulatory subunits) pair with Cyclin-Dependent Kinases (CDKs; catalytic subunits) to control progression.
- Checkpoints: G1/S (restriction point; p53, Rb crucial) & G2/M ensure fidelity.
⭐ Li-Fraumeni syndrome: germline TP53 mutations cause high predisposition to diverse early-onset cancers.
Oncogenes & Suppressors - Genes Gone Wild
Cancer arises from genetic changes. Oncogenes act as accelerators, while Tumor Suppressor Genes (TSGs) are brakes.
| Feature | Oncogenes | Tumor Suppressor Genes (TSGs) |
|---|---|---|
| Normal Function | Promote cell growth/division | Inhibit cell growth/division; repair DNA |
| Effect of Mutation | Gain-of-function (activated) | Loss-of-function (inactivated) |
| Alleles for Cancer | One (dominant) | Two (recessive; Knudson's 'two-hit' hypothesis) |
| Activation/Inactivation | Point mutation, amplification, translocation | Deletion, point mutation, methylation |
| Examples | RAS, MYC, EGFR, HER2 | TP53, RB1, APC, BRCA1/2 |
⭐ The Philadelphia chromosome t(9;22) creates the BCR-ABL fusion oncogene in CML.
Carcinogenesis - Making of a Monster
- Steps: Initiation (irreversible DNA mutation), Promotion (reversible clonal expansion of initiated cells), Progression (malignant transformation, genetic instability, invasion).
- Carcinogens:
- Chemical: Direct-acting; Procarcinogens (need activation, e.g., Aflatoxin B1 - liver; asbestos - lung; benzene - leukemia; PAHs - lung/skin).
- Radiation: UV (pyrimidine dimers, e.g., $T-T$); Ionizing (DNA breaks).
- Viral: HPV (E6 degrades p53, E7 inhibits RB); EBV (Burkitt's, Nasopharyngeal Ca); HBV/HCV (HCC); HTLV-1 (ATLL).

Loading diagram…
⭐ Aflatoxin B1, from Aspergillus on improperly stored grains/nuts, is a potent hepatocarcinogen, especially with chronic Hepatitis B/C.
Metastasis & Immunity - Spread & Evade
- Metastatic Cascade: Sequential steps for cancer spread.
Loading diagram…
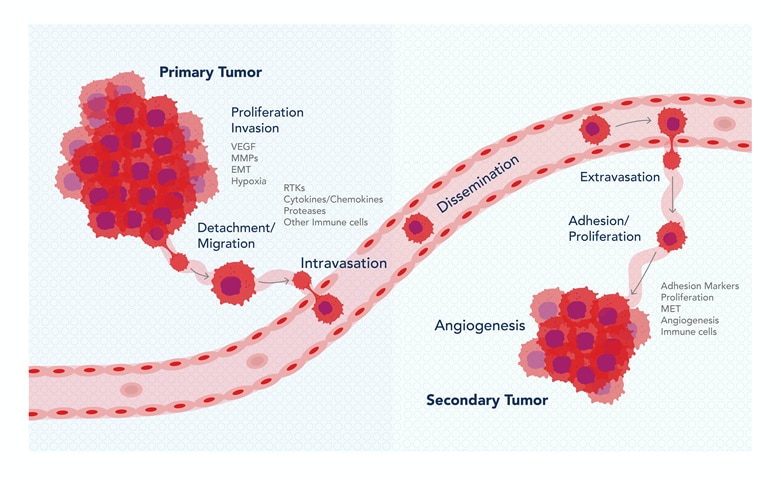
- Angiogenesis: New blood vessel formation, vital for tumor growth/spread. Key mediator: VEGF.
- Tumor Antigens:
- TSA (Tumor-Specific Antigens): Unique to tumor cells (e.g., mutated oncogenes).
- TAA (Tumor-Associated Antigens): Overexpressed/aberrantly expressed (e.g., HER2).
- Immune Surveillance & Immunoediting: (3 Es - Elimination, Equilibrium, Escape)
- Tumor cells evolve to evade immune destruction.
- Mechanisms of Immune Evasion:
- ↓MHC Class I expression (hides from CD8+ T cells).
- ↑PD-L1 expression (inhibits T-cell attack via PD-1).
- Secretion of immunosuppressive cytokines (e.g., TGF-β, IL-10).
- Induction of Tregs.
⭐ Loss of E-cadherin function is crucial for epithelial-mesenchymal transition (EMT) and invasion.
High‑Yield Points - ⚡ Biggest Takeaways
- Hallmarks of Cancer include sustained proliferation, evading growth suppressors, angiogenesis, and invasion/metastasis.
- Tumor suppressor genes like p53 & Rb require two-hit inactivation (Knudson's hypothesis).
- Oncogenes such as RAS & MYC need one-hit activation for transformation.
- Carcinogenesis is a multi-step process: initiation, promotion, and progression.
- Key factors: chemical carcinogens (aflatoxin, asbestos) & viral carcinogens (HPV, EBV).
- Metastasis (invasion to colonization) is the primary cause of cancer mortality.
- Warburg effect: Cancer cells preferentially use aerobic glycolysis.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more