

Syndrome Overview - Defining the Duo
| Feature | NephrOtic Syndrome | NephrItic Syndrome |
|---|---|---|
| Primary Defect | Podocyte damage, ↑ permeability | Glomerular Inflammation |
| Proteinuria | Massive: $ > \textbf{3.5g/24h}## Syndrome Overview - Defining the Duo |
| Mild-moderate: $ < \textbf{3.5g/24h}## Syndrome Overview - Defining the Duo
|
| Hematuria | Often absent/microscopic | Gross/microscopic; RBC casts | | Edema | Severe, generalized (hypOalbuminemia) | Mild, periorbital (Na⁺/water retention) | | Hypertension | Less common, may be late | Common, often abrupt (Increased BP) | | Renal Function | Often preserved initially | Often Impaired (↑ creatinine, oliguria) | | Key Features | HypOalbuminemia, hyperlipidemia, lipiduria | Immune complex deposition | | Mnemonic | 📌 PrOteinuria, HypOalbuminemia, Oedema, Hyperlipidemia | 📌 Inflammation, Immune complexes, Increased BP, Impaired renal fn. |> ⭐ Oval fat bodies (Maltese cross appearance under polarized light) are characteristic of nephrotic syndrome.
Nephrotic Syndrome - Leaky Filters Galore
Pathophysiology: Podocyte injury, loss of GBM negative charge → ↑ protein permeability.
Cardinal Features:
- Proteinuria: $ > \textbf{3.5 g/24h}$ (or $ > \textbf{50 mg/kg/day}$ children).
- Hypoalbuminemia: Serum albumin $ < \textbf{3 g/dL}$.
- Generalized Edema: Anasarca, often periorbital.
- Hyperlipidemia & Lipiduria: Oval fat bodies, fatty casts.
📌 NAPHROTIC Mnemonic: Na+ retention, Albuminuria, Proteinuria ($ > \textbf{3.5g/day}$), Hyperlipidemia, Renal vein thrombosis, Orbital edema, Thromboembolism, Infection, Coagulability.
Common Causes:
- Primary Glomerular Diseases:
Disease Key Biopsy Finding MCD Podocyte effacement (EM) FSGS Segmental sclerosis (LM) Membranous Neph. Thick GBM, subepithelial spikes (EM/IF) - Secondary Causes:
- Diabetes Mellitus (most common in adults)
- Amyloidosis
- SLE (Class V)
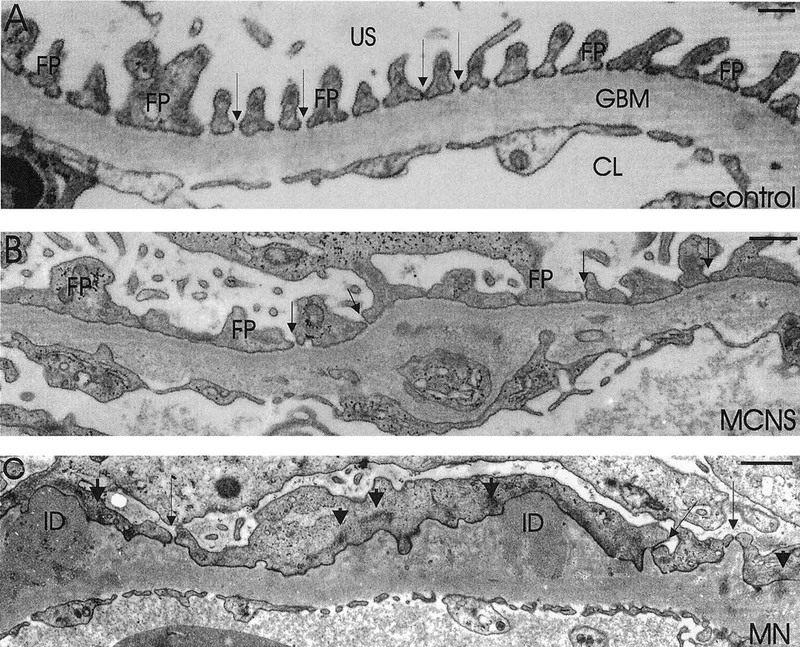
⭐ Minimal Change Disease is the most common cause of nephrotic syndrome in children and shows diffuse effacement of podocyte foot processes on electron microscopy.
Nephritic Syndrome - Inflamed & Angry Gloms
Pathophysiology: Glomerular inflammation & immune complex deposition → glomerular injury, ↓GFR.
-
Cardinal Features (📌 PHARAOH):
- Proteinuria (mild-moderate, <3.5 g/day)
- Hematuria (cola-colored urine, RBC casts present)
- Azotemia (↑BUN, ↑Creatinine)
- RBC casts (confirms glomerular hematuria)
- Anti-Strep titres (↑ in PSGN, e.g., ASO >200 IU/mL)
- Oliguria (<400 mL/day)
- Hypertension (HTN)
-
Common Causes:
- Primary Glomerulonephritis (GN):
Cause Key Biopsy Finding IgA Nephropathy Mesangial IgA deposits PSGN Diffuse hypercellularity, subepithelial "humps" RPGN Crescents in Bowman's space - Secondary: SLE, Henoch-Schönlein Purpura (HSP), Vasculitis (e.g., GPA, MPA).
- Primary Glomerulonephritis (GN):
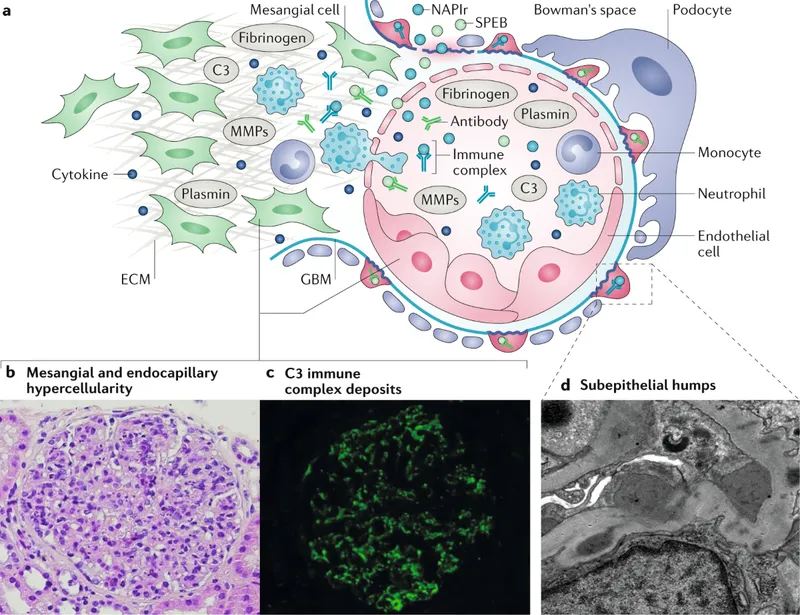
⭐ PSGN: 1-3 wks (pharyngitis) or 2-6 wks (impetigo) post-infection; features subepithelial 'humps' (EM), low C3.
Key Glomerulopathies - Rogues' Gallery
⭐ IgA Nephropathy is the most common glomerulonephritis worldwide and often presents with episodic macroscopic hematuria concurrent with mucosal infections.
| Disease | Syndrome | LM | IF | EM | Key Notes |
|---|---|---|---|---|---|
| MCD | Nephrotic | Normal | Negative | Foot process effacement | Children; steroid-responsive |
| FSGS | Nephrotic | Segmental sclerosis | Often negative | Foot process effacement | HIV, heroin; variable response |
| Membranous Neph. | Nephrotic | Thick GBM, spikes | Granular IgG, C3 | Subepithelial deposits | Idiopathic, HBV, SLE; "spike & dome" |
| Diabetic Neph. | Nephrotic | K-W nodules | Negative | Thick GBM | DM; ESRD risk |
| IgA Nephropathy | Nephritic | Mesangial prolif. | Mesangial IgA | Mesangial deposits | Berger's; URI-hematuria |
| PSGN | Nephritic | Diffuse prolif., humps | Granular IgG, C3 | Subepithelial "humps" | Post-strep; good prognosis (kids) |
| RPGN (Crescentic) | Nephritic | Crescents | Variable: Linear IgG (Goodpasture's), Pauci-immune (ANCA), Granular (Immune complex) | GBM breaks (Goodpasture's) | Rapid renal failure; urgent Rx |
High‑Yield Points - ⚡ Biggest Takeaways
- Nephrotic Syndrome is defined by massive proteinuria (>3.5 g/day), hypoalbuminemia, edema, and hyperlipidemia.
- Minimal Change Disease: commonest nephrotic in children; effacement of podocyte foot processes on EM.
- Nephritic Syndrome presents with hematuria (RBC casts), oliguria, hypertension, and azotemia.
- Post-Streptococcal Glomerulonephritis (PSGN): classic nephritic, ↑ASO titers, low C3, subepithelial "humps".
- IgA Nephropathy (Berger's Disease): most common primary glomerulonephritis; recurrent hematuria often after URI.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more