

HIV Basics & Transmission - Viral Villainy Unveiled
- Structure: Enveloped RNA retrovirus.
- Key Antigens: gp120 (surface, CD4 binding), gp41 (transmembrane, fusion), p24 (capsid, early marker).

- Key Antigens: gp120 (surface, CD4 binding), gp41 (transmembrane, fusion), p24 (capsid, early marker).
- Transmission Routes:
- Sexual (most common): Risk: receptive anal > vaginal > insertive > oral.
- Parenteral: IV drug use (shared needles), contaminated blood products (highest efficiency).
- Perinatal (Vertical): Mother-to-child (in utero, delivery, breastfeeding). Risk ~25-30% without ART.
- Brief Lifecycle:
- Attachment (gp120 to CD4+coreceptor) & Fusion (gp41).
- Reverse Transcription (RNA→DNA).
- Integration (viral DNA into host DNA).
- Replication, Assembly, Budding, Maturation.
⭐ p24 antigen is the earliest detectable viral marker, typically 2-3 weeks post-exposure, before antibodies develop.
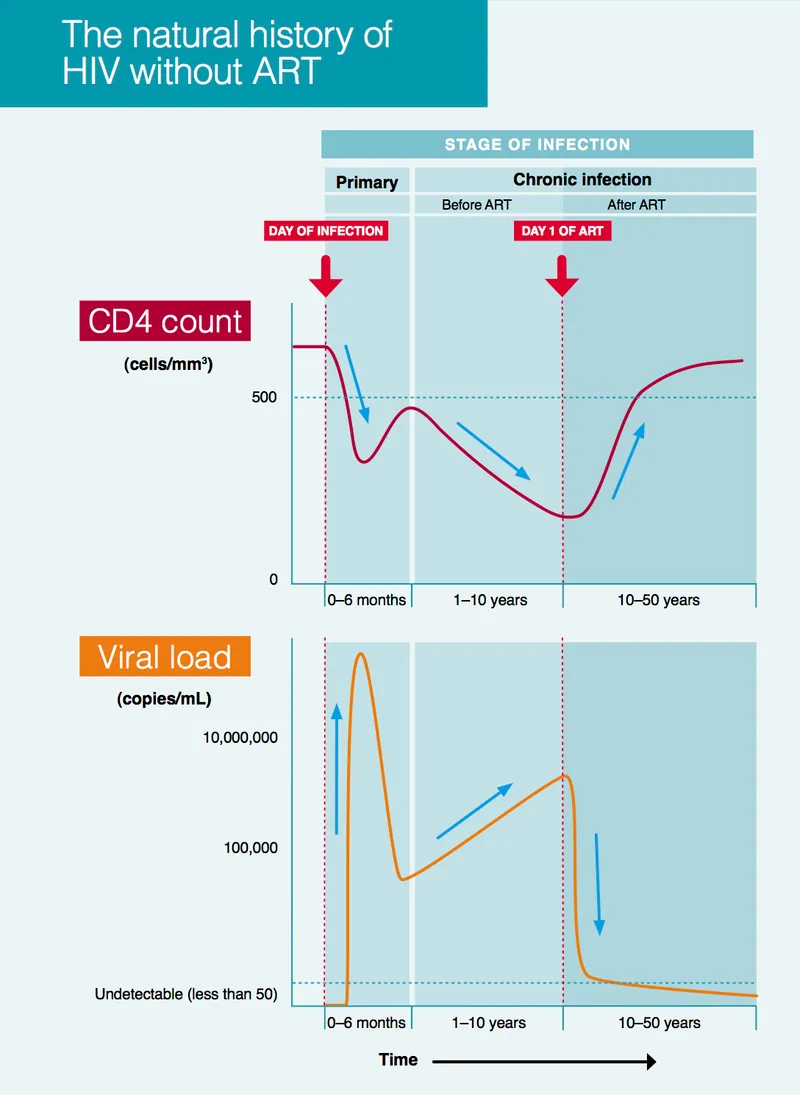
Pathogenesis & Clinical Course - Immune System Under Siege
- CD4+ T-cell Depletion: HIV targets CD4+ cells, causing immune destruction. Entry via co-receptors CCR5 (early) or CXCR4 (late, faster progression).
- Infection Phases:
- Acute Retroviral Syndrome (ARS): 2-4 weeks post-exposure. Flu/mono-like symptoms (fever, rash). High viral load.
⭐ The typical 'seroconversion illness' mimics infectious mononucleosis.
- Clinical Latency: Asymptomatic (median ~10 yrs untreated). Gradual CD4↓.
- Symptomatic Disease: Constitutional symptoms, opportunistic infections (OIs).
- AIDS: CD4 < 200/µL OR AIDS-defining illness.
- Acute Retroviral Syndrome (ARS): 2-4 weeks post-exposure. Flu/mono-like symptoms (fever, rash). High viral load.
- WHO Staging (Simplified):
- Stage 1: Asymptomatic.
- Stage 2: Mild (e.g., weight loss <10%).
- Stage 3: Advanced (e.g., TB, severe infections).
- Stage 4: Severe/AIDS-defining (e.g., PCP, Kaposi).
HIV Diagnosis & ART - Finding & Fighting HIV
- Diagnosis:
- Screening: 4th gen ELISA/Rapid (p24 Ag+Ab). Window: 2-4 wks.
- Confirmatory: Western Blot/NAAT/HIV-RNA.
- Infant (<18m): HIV DNA/RNA PCR (6wks, 3-6m, 12-18m).
- Monitoring: CD4 (Q3-6M), VL (at 6m, then annually if suppressed).
- ART - Treat All:
- Goals: Suppress VL, ↑CD4, ↓transmission.
- ⭐ > NACO 1st line: Tenofovir (TDF) + Lamivudine (3TC) + Dolutegravir (DTG).
- 2nd line: Per resistance testing.
- ARV Classes (📌 INSTI-gravir):
- NRTI: TDF (nephrotoxic), Zidovudine (AZT - anemia).
- NNRTI: Efavirenz (EFV - neuropsych), Nevirapine (NVP - rash).
- PI: Atazanavir (ATV - jaundice), Lopinavir/r (LPV/r - dyslipidemia).
- INSTI: Dolutegravir (DTG - insomnia).
- EI (Entry Inhibitors): Enfuvirtide.

- Prophylaxis:
- PEP: Start <72h (TDF+3TC+DTG for 28d).
- PrEP: Daily TDF+FTC/3TC for high-risk individuals.
Opportunistic Infections & Cancers - AIDS' Deadly Allies
Key OIs and malignancies that define AIDS, driven by severe immunosuppression. Early ART is crucial.
-
Common Opportunistic Infections (Typical CD4, Dx, Tx):
- Pneumocystis jirovecii Pneumonia (PJP): <200/µL. Dx: CXR (diffuse infiltrates), BAL. Tx: Co-trimoxazole.
- Tuberculosis (TB): Any CD4. Dx: Sputum AFB/GeneXpert. Tx: Standard RIPE + ART.
- Mycobacterium Avium Complex (MAC): <50/µL. Dx: Blood culture. Tx: Clarithromycin + Ethambutol.
- Cryptococcal Meningitis: <100/µL. Dx: CSF India ink, Cryptococcal Ag. Tx: Amphotericin B + Flucytosine, then Fluconazole.
- Cerebral Toxoplasmosis: <100/µL (if Toxo IgG positive). Dx: CT/MRI (ring-enhancing lesions). Tx: Pyrimethamine + Sulfadiazine + Leucovorin.
- Progressive Multifocal Leukoencephalopathy (PML): <200/µL (JC virus). Dx: CSF JC virus PCR, MRI. Tx: ART.
- CMV Retinitis: <50/µL. Dx: Fundoscopy. Tx: Ganciclovir/Valganciclovir.
-
OI Prophylaxis (Primary):
- PJP: Co-trimoxazole if CD4 <200/µL.
- Toxoplasmosis: Co-trimoxazole if CD4 <100/µL & Toxo IgG positive.
- MAC: Azithromycin if CD4 <50/µL.
-
Common HIV-Associated Malignancies:
- Kaposi's Sarcoma (KS) - HHV-8 associated.
- Non-Hodgkin's Lymphoma (NHL) - esp. Primary CNS Lymphoma (EBV).
- Cervical Cancer (invasive) - HPV associated.
-
IRIS (Immune Reconstitution Inflammatory Syndrome): Paradoxical worsening of pre-existing (often subclinical) OIs after ART initiation due to recovering immunity.

⭐ Drug of choice for PCP treatment is Co-trimoxazole; also used for prophylaxis against PCP and Toxoplasmosis.
High‑Yield Points - ⚡ Biggest Takeaways
- CD4 count guides HIV staging and OI prophylaxis.
- ART is key for viral suppression and improved prognosis.
- Key OIs: PJP (CD4 < 200), Toxoplasmosis (CD4 < 100), MAC (CD4 < 50).
- IRIS (Immune Reconstitution Inflammatory Syndrome) can occur post-ART initiation.
- PEP for HIV: start ideally <2h, up to 72h post-exposure.
- HIV diagnosis: Screening tests (ELISA/Rapid) confirmed by Western Blot/NAAT.
- Prevent vertical transmission with maternal ART and neonatal prophylaxis.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more