

Foundations & Assessment - Backbone Blueprint
- Core Principles
- Biopsychosocial model.
- Goal-oriented: Functional restoration.
- Interdisciplinary team.
- Patient education for self-management.
- Assessment Protocol
- History
- Pain profile.
- ⚠️ Red flags (neuro deficits, cauda equina, systemic symptoms).
- Yellow flags (psychosocial).
- Physical Examination
- Observation: Posture, gait.
- Palpation: Tenderness, spasm.
- ROM: Spinal segments.
- Neurological: Motor (MRC 0-5), Sensory (dermatomes), Reflexes (DTRs 0-4+, Babinski).
- Special tests: SLR, Spurling’s.
- Functional Scales
- VAS (pain).
- ODI (lumbar disability).
- NDI (cervical disability).
- Imaging
- X-ray: Initial, trauma, instability.
- MRI: Soft tissues, neural elements (disc, cord).
- CT: Bony detail, complex fractures.
- History

⭐ Early identification of red flags (e.g., progressive neurological deficit, saddle anesthesia, unexplained fever) is critical to rule out serious spinal pathology requiring urgent intervention.
Common Conditions Rehab - Ache Avengers
-
Low Back Pain (LBP)
- Classification: Acute (<6 weeks), Subacute (6-12 weeks), Chronic (>12 weeks).
- ⚠️ Red Flags: Cauda equina (bowel/bladder, saddle anesthesia), unexplained weight loss, fever, trauma, progressive neuro deficit, cancer Hx.
- Rehab:
- McKenzie Method (extension bias, centralization).
- Williams' Flexion Exercises (stenosis, flexion bias).
- Core stabilization (Transversus abdominis, multifidus, e.g., McGill's Big 3).
- Aerobic conditioning.
-
Cervical Pain (Neck Pain)
- Key: Postural correction, ergonomic adjustments (workstation).
- Exercises: ROM, stretching, cervical isometrics, deep neck flexor (DNF) strengthening (chin tucks).
-
Lumbar Disc Herniation
- Common: Posterolateral, radicular pain.
- Rehab:
- Directional preference exercises (e.g., McKenzie extension).
- Nerve gliding techniques.
- Core stability for prevention.
- Avoid: Sustained flexion, poor lifting mechanics.
-
Spondylolisthesis
- Focus: Segmental stabilization, core (transversus abdominis) & glute strength.
- Avoid: Lumbar hyperextension, high-impact activities. Bracing if symptomatic.
-
General Rehab Principles
- Pain Management: Cryo/thermotherapy, TENS, NSAIDs (short-term).
- Patient Education: Body mechanics (lifting, sitting), activity pacing.
- Functional Restoration: Graded activity, return to work/sport.
⭐ Most acute LBP resolves in 6 weeks with conservative care; imaging often not needed initially without red flags.
Loading diagram…
SCI Rehabilitation - Cord Crusaders
Goal: Maximize functional independence & quality of life (QoL), prevent complications. Multidisciplinary team approach.
-
Phases of SCI Rehab:
- Acute: Medical stabilization, prevent secondary injury.
- Subacute (Rehabilitation Unit): Intensive therapy, functional goals.
- Chronic/Community Reintegration: Maintain function, QoL, vocational rehab.
-
Key Management Areas:
- Mobility: Bed mobility, transfers, wheelchair (W/C) skills, gait training (orthotics, FES).
- ADLs: Self-care, adaptive devices.
- Bladder: Intermittent catheterization (IC) preferred. Prevent UTIs.
- Bowel: Timed program, diet, digital stimulation.
- Skin: Pressure relief (turn q2h bed, shift weight q15-30min W/C).
- Respiratory: Crucial for high cervical lesions (e.g., C1-C4 often ventilator-dependent).
- Spasticity: Stretching, meds (e.g., Baclofen).
- Pain: Neuropathic, musculoskeletal.
-
Autonomic Dysreflexia (AD):
- Occurs with lesions T6 or above.
- Symptoms: Sudden ↑BP, pounding headache, bradycardia, sweating above lesion.
- Management: Sit patient up, loosen constrictive clothing, check bladder/bowel, antihypertensives if needed.
Loading diagram…
⭐ Autonomic dysreflexia (AD) is a potentially life-threatening hypertensive crisis in individuals with SCI at or above T6, typically triggered by noxious stimuli below the level of injury.
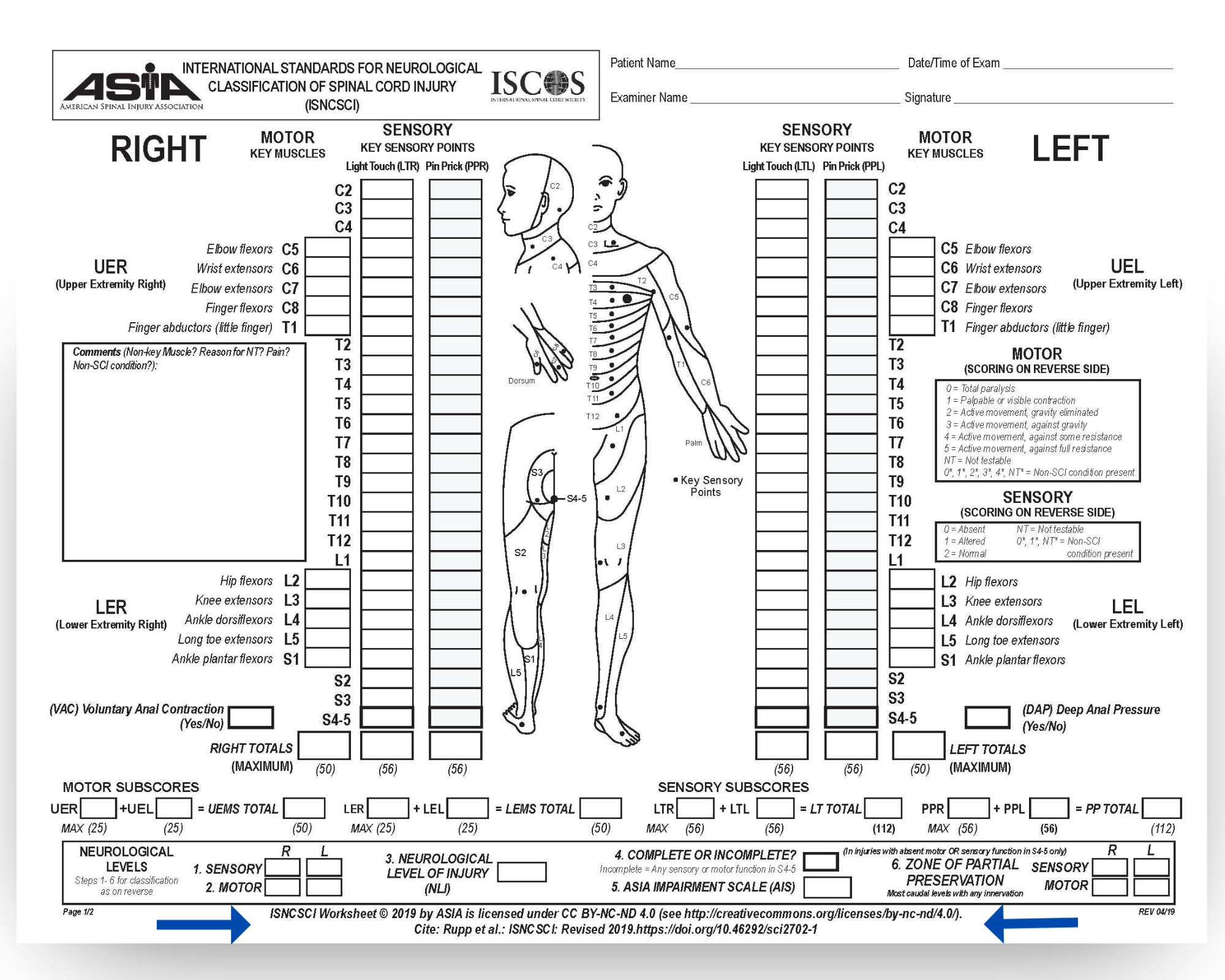
📌 ASIA Scale: American Spinal Injury Association Impairment Scale for classifying severity (A=Complete to E=Normal).
High‑Yield Points - ⚡ Biggest Takeaways
- SCI levels dictate functional outcomes: C5 (elbow flexion), C6 (tenodesis grasp), C7 (independent transfers).
- Autonomic Dysreflexia (SCI above T6): medical emergency with hypertension, bradycardia, triggered by noxious stimuli.
- Prevent pressure ulcers with regular 2-hourly turning, meticulous skin inspection, and appropriate support surfaces.
- Neurogenic bladder (intermittent catheterization) and bowel (timed programs) require diligent management.
- Manage spasticity post-SCI with physiotherapy, oral baclofen/tizanidine, or botulinum toxin injections.
- The ASIA Impairment Scale is crucial for classifying SCI severity and predicting neurological prognosis after injury.
- Early and comprehensive rehabilitation significantly improves functional independence and quality of life post-SCI.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more