

Definition & Triggers - Bleed Big, Act Fast
- Massive Hemorrhage:
- Loss >1 blood volume/24h.
- Loss >50% blood volume/3h.
- Bleeding >150 mL/min.
- Massive Transfusion (MTP):
- ≥10 units PRBCs/24h.
- ≥4 units PRBCs/1h + ongoing need. 📌 MTP "Ten-Four" Rule.
- Triggers for MHP Activation:
- Clinical judgment (paramount).
- Persistent shock: SBP <90 mmHg, HR >120 bpm.
- Scoring: ABC score ≥2.
Loading diagram…
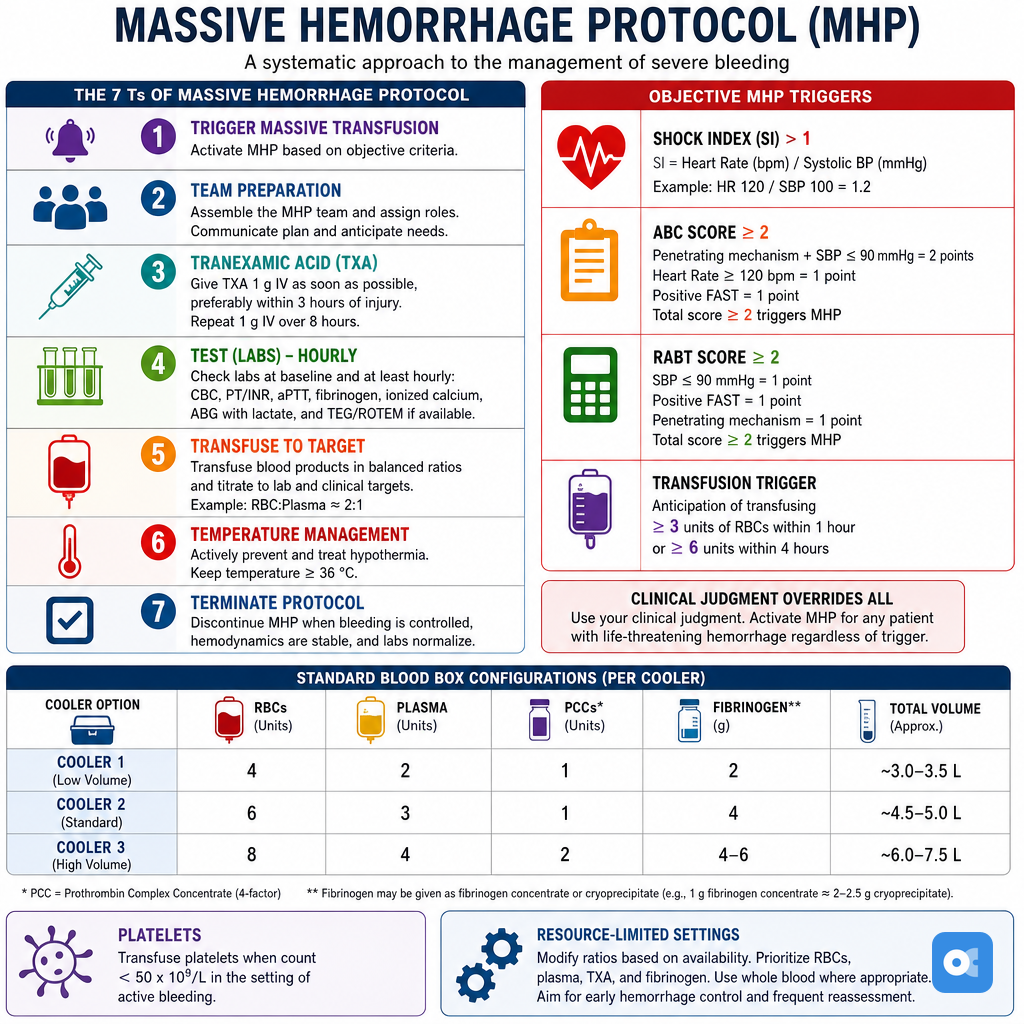
> ⭐ ABC Score (Assessment of Blood Consumption): Penetrating injury, SBP ≤**90 mmHg**, HR ≥**120 bpm**, Positive FAST. Score ≥**2** strongly predicts MHP need.
Initial Management - Stop the Gush!
- Primary Survey (ABCDE): Secure airway, ensure adequate oxygenation & ventilation.
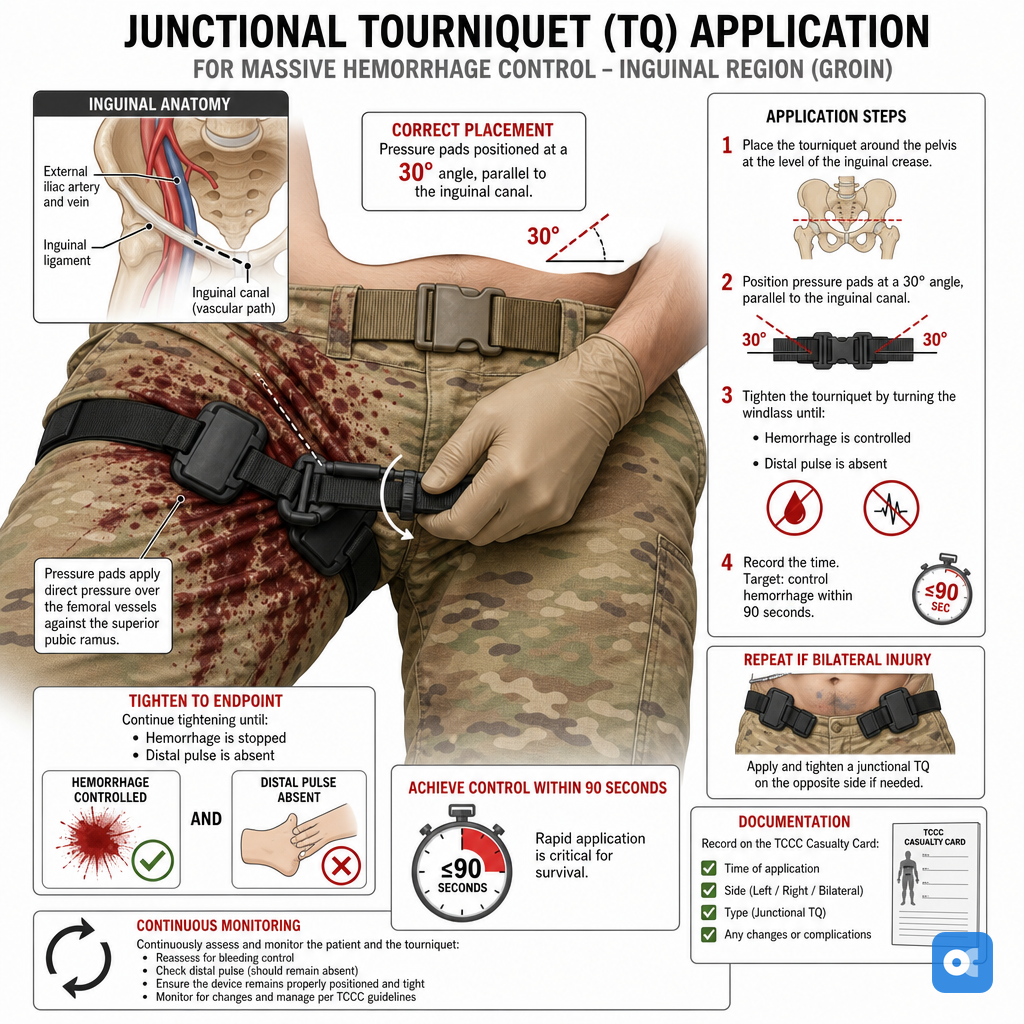
- Control Exsanguination: The absolute priority!
- External: Apply direct pressure, tourniquets (for limbs, note time), deep wound packing.
- Internal: Urgent surgical exploration or interventional radiology for source control.
- Initiate Damage Control Resuscitation (DCR) principles immediately.
- Permissive Hypotension: Target SBP 80-100 mmHg or MAP ~65 mmHg until definitive bleeding control (⚠️ Avoid if Traumatic Brain Injury suspected).
Loading diagram…
> ⭐ Early surgical or interventional radiology consultation for definitive bleeding control is critical and life-saving.
Transfusion Strategy - Red Rescue Ratio
- Goal: Mimic whole blood; restore volume & hemostasis.
- Ratio: 1:1:1 (PRBC:FFP:Platelets) standard.
- PRBCs: ↑ $O_2$-carrying capacity.
- FFP: Replaces clotting factors; dose 10-15 mL/kg.
- Platelets: Target >50k/μL (general), >100k/μL (CNS/active bleed).
- Cryoprecipitate: For fibrinogen <1.5-2 g/L. Dose 1-2 bags/10kg.
- Tranexamic Acid (TXA): 1g IV (10 min), then 1g (8 hrs). Give <3 hrs post-injury.
- Monitor & replete Calcium.
⭐ The PROPPR trial supported 1:1:1 ratio for improved hemostasis & ↓ 24-hr mortality in massive hemorrhage_._
Adjunctive Therapies - Clotting Crew Aid
- Tranexamic Acid (TXA):
- Antifibrinolytic; inhibits plasminogen activation.
- Dose: 1g IV (10 min), then 1g IV (8 hrs).
- Give within 3 hours of injury.
- Calcium (Chloride/Gluconate):
- Essential for coagulation.
- Monitor ionized Ca (iCa); target > 1.1 mmol/L (total Ca > 2.2 mmol/L).
- Give after every 4 units PRBC.
- Fibrinogen Support:
- Cryoprecipitate: 10-15 units OR Fibrinogen concentrate: 2-4g.
- If fibrinogen < 1.5-2.0 g/L or TEG/ROTEM guided.
- Prothrombin Complex Concentrate (PCC):
- For urgent warfarin reversal; consider if bleeding persists.
- Dose: 25-50 IU/kg.
⭐ TXA within 3 hours of trauma significantly reduces bleeding mortality.
Monitoring & Complications - Storm Watch Duty
- Continuous Watch:
- Vitals: ECG, IBP, SpO₂, EtCO₂.
- Labs: ABG (lactate, BE, K⁺, iCa²⁺), Coags (TEG/ROTEM).
- Core Temp.
- Urine Output: > 0.5 mL/kg/hr.
- Resuscitation Targets:
- Hb > 7 g/dL, Platelets > 50,000/μL, Fibrinogen > 1.5-2 g/L, INR < 1.5.
- Lethal Triad:
- Hypothermia (< 35°C): Warm.
- Acidosis (pH < 7.35): Perfuse.
- Coagulopathy: Use TEG/ROTEM.
- Other Risks:
- Hypocalcemia (citrate): Monitor iCa²⁺.
- Hyperkalemia (stored RBCs).
- TRALI/TACO.
⭐ Hypothermia (< 35°C) significantly worsens coagulopathy and is a key component of the "lethal triad" in trauma.
High-Yield Points - ⚡ Biggest Takeaways
- Massive transfusion: >1 blood volume/24h or >10 units PRBCs/24h.
- Activate MHP with clinical shock signs or high ABC/Shock Index score.
- Crucial: 1:1:1 ratio of PRBC:FFP:Platelets for balanced resuscitation.
- DCR: Permissive hypotension (SBP 80-90 mmHg, avoid TBI); correct lethal triad (acidosis, hypothermia, coagulopathy).
- Early Tranexamic Acid (TXA): 1g IV bolus, then 1g infusion.
- Prevent/treat hypocalcemia, hypothermia, and acidosis aggressively.
- Key complications: TRALI, TACO, dilutional coagulopathy_
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more