

NAI Basics & Skeletal Scan - Bones Don't Lie
- Non-Accidental Injury (NAI): Harm to a child due to non-accidental means by a caregiver.
- Red Flags: Inconsistent/vague history, delayed medical attention, multiple injuries of different ages, specific fracture patterns (e.g., metaphyseal, posterior ribs, sternal, scapular).
- Imaging Indications:
- All suspected NAI cases in children < 2 years.
- Older children with suspicious injuries if history is inconsistent.
- Skeletal Survey Components:
- AP/Lat: Skull, chest, spine.
- AP: Pelvis, hands, feet.
- AP/Lat: Long bones (humeri, femora, tibiae/fibulae).
- Oblique views of ribs.
- Follow-up Survey: Crucial in 10-14 days to detect initially occult fractures (e.g., healing periosteal reactions).

⭐ Skeletal survey is the primary imaging modality for suspected NAI in children <2 years old due to its ability to detect a wide range of fractures, including those not clinically apparent.
NAI Fracture Patterns - Twists & Telltales
Error generating content for this concept group: Failed to process successful response
NAI: Head & Viscera - Beyond Broken Bones
- Abusive Head Trauma (AHT): Critical intracranial injuries.
- Subdural Hematoma (SDH): Interhemispheric, convexity, posterior fossa; often thin.
- Retinal Hemorrhages: Highly specific; often bilateral, multilayered, extending to ora serrata.
- Hypoxic-Ischemic Injury (HII): From shaking/impact; diffuse cerebral edema, watershed infarcts.
- AHT Imaging:
Loading diagram…
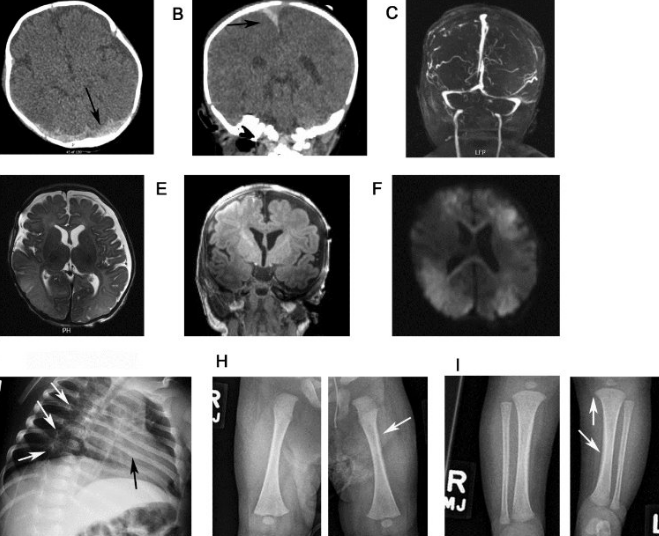
- CT for acute bleeds; MRI for subacute/chronic changes, HII, and small SDHs.
- Visceral Injuries (Often Occult):
- Liver laceration: Most common (posterior right lobe).
- Pancreatic injury, bowel (hematoma/perforation), adrenal hemorrhage.
- High mortality; suspect with unexplained shock/anemia. CT abdomen with contrast.
- Cutaneous Clues: Patterned bruises (e.g., handprints), specific burn types (e.g., cigarette, immersion).
⭐ The triad of subdural hematoma, retinal hemorrhages, and encephalopathy is highly suggestive of Abusive Head Trauma.
NAI Imaging Mimics - Innocent Impostors
- Osteogenesis Imperfecta (OI): Blue sclera, wormian bones, gracile bones, recurrent fractures (minor trauma).
⭐ Osteogenesis Imperfecta is a key differential for multiple fractures, but Classic Metaphyseal Lesions (CMLs) and posterior rib fractures are rare in OI.
- Rickets: Cupping/fraying/splaying of metaphyses, Looser zones, rachitic rosary.
- Scurvy: Subperiosteal hemorrhage, Wimberger's sign (ring epiphysis), Pelkan spur, Frankel's line.
- Caffey Disease: Infantile cortical hyperostosis (mandible, clavicle, ulna); irritability, fever.
- Normal Variants: Physiologic periostitis (newborn), distal clavicular erosions (resolves by 2 yrs).
- Birth Trauma: Clavicle, humerus, femur fractures.
- Metabolic bone disease workup if suspected.
oka
High‑Yield Points - ⚡ Biggest Takeaways
- Skeletal survey is crucial for suspected abuse in children < 2 years.
- Classic metaphyseal lesions (CMLs) are highly specific for non-accidental injury.
- Posterior rib fractures, especially multiple and healing, strongly indicate abuse.
- Subdural hematomas (SDH), particularly interhemispheric, are common in abusive head trauma.
- Retinal hemorrhages are strongly associated with abusive head trauma.
- Multiple fractures at various stages of healing are a key indicator.
- CT head for acute injury; MRI for detailed brain assessment and timing of injury.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more