

Ca/P Homeostasis Overview - Balancing Act Buddies
Calcium (Ca) and Phosphate (PO₄) are crucial minerals, their balance meticulously managed.
- Normal Serum Levels:
- Calcium (Total): 8.5-10.5 mg/dL
- Calcium (Ionized, $Ca^{2+}$): 4.5-5.6 mg/dL
- Phosphate: 2.5-4.5 mg/dL
- Body Distribution:
- Ca: ~99% in bone; ~1% in ECF/ICF.
- PO₄: ~85% in bone; ~14% ICF; ~1% ECF.
- Key Regulatory Players:
- Organs: Bone, Kidneys, Intestine.
- Hormones: Parathyroid Hormone (PTH), Vitamin D (Calcitriol), Calcitonin, FGF23.

⭐ Ionized calcium is the physiologically active form and is tightly regulated.
PTH Deep Dive - Calcium's Chief
Parathyroid Hormone (PTH): Calcium's primary regulator.
- Source: Chief cells (parathyroid).
- Synthesis: PreproPTH → ProPTH → PTH.
- Secretion Stimuli: ↓ Serum $Ca^{2+}$, ↑ Serum $PO_4^{3-}$ (indirectly), ↓ $1,25-(OH)_2D_3$.
- Secretion Inhibitors: ↑ Serum $Ca^{2+}$ (via CaSR), ↑ $1,25-(OH)_2D_3$, severe ↓ Mg²⁺ (chronic).
- Actions:
- Bone: ↑ Resorption (via RANKL) → ↑ $Ca^{2+}$ & $PO_4^{3-}$ release.
- Kidney: ↑ $Ca^{2+}$ reabsorption (DCT), ↓ $PO_4^{3-}$ reabsorption (PCT), ↑ 1α-hydroxylase activity.
- Intestine (Indirect via Vit D): ↑ $Ca^{2+}$ & $PO_4^{3-}$ absorption.
- Net Effect: ↑ Serum $Ca^{2+}$, ↓ Serum $PO_4^{3-}$. 📌 PTH: Phosphate Trashing Hormone.
⭐ PTH increases renal phosphate excretion (phosphaturia) by inhibiting Na/Pi co-transporters in the proximal convoluted tubule (PCT).
synthesis, regulation, and target organ actions)
Loading diagram…
Vitamin D Voyage - Sunshine Soaker
- Sources:
- Diet: D₂ (ergocalciferol), D₃ (cholecalciferol)
- Skin: UV light on 7-dehydrocholesterol → D₃
- Activation Pathway:
Loading diagram…
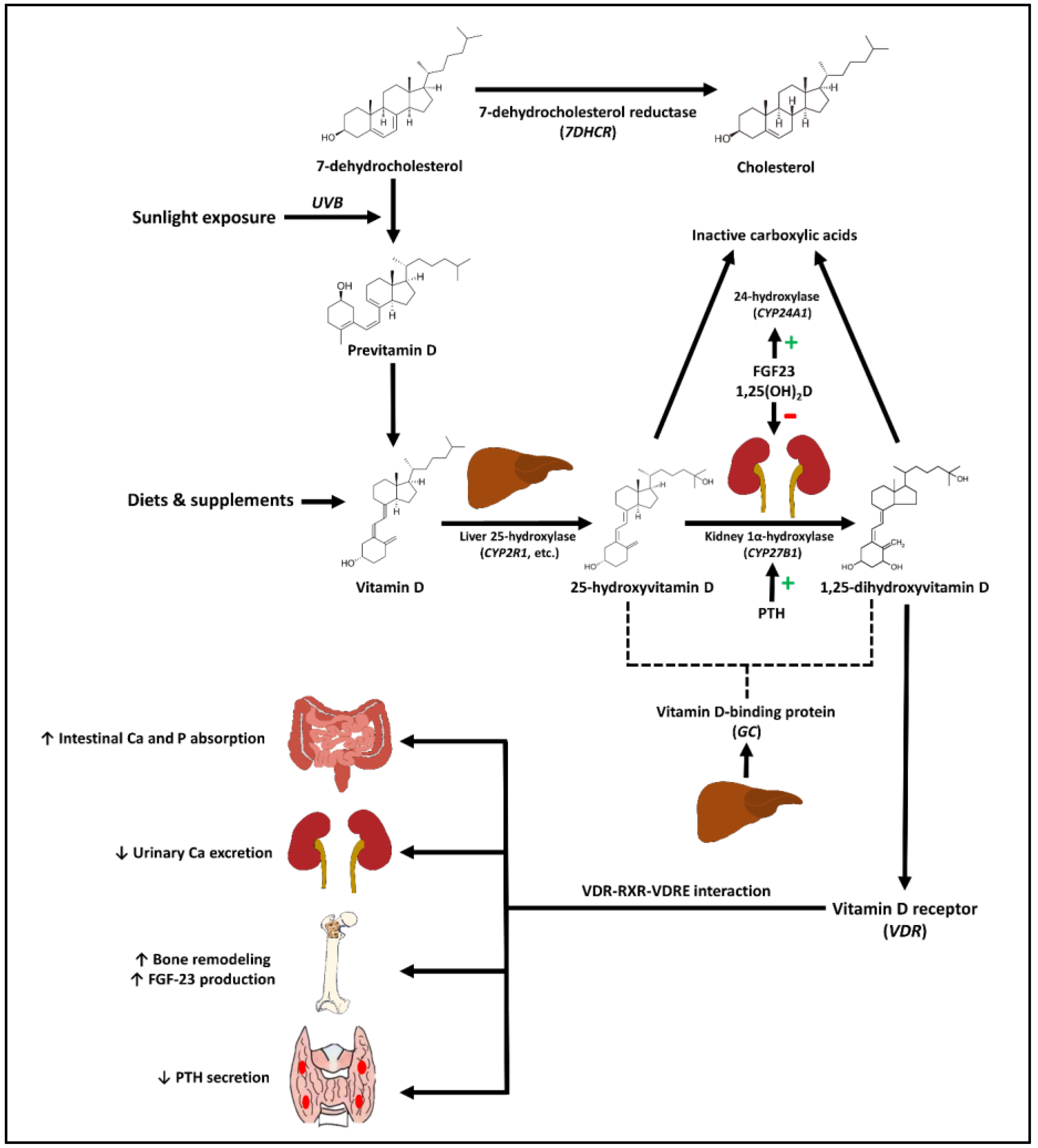
- Regulation of 1α-hydroxylase (Kidney):
- Stimulated by: PTH, ↓ Serum $Ca^{2+}$, ↓ Serum $PO_4^{3-}$
- Inhibited by: FGF23, ↑ 1,25(OH)₂D (Calcitriol)
- Actions of Calcitriol (1,25(OH)₂D):
- Intestine: ↑ $Ca^{2+}$ absorption (via calbindin-D9k), ↑ $PO_4^{3-}$ absorption
- Bone: Promotes mineralization (with adequate Ca/P); high doses + PTH → bone resorption
- Kidney: ↑ $Ca^{2+}$ & $PO_4^{3-}$ reabsorption (minor effect)
- Parathyroid Gland: ↓ PTH synthesis (negative feedback)
- Net Effect: ↑ Serum $Ca^{2+}$, ↑ Serum $PO_4^{3-}$
⭐ The enzyme 1α-hydroxylase, located in the proximal tubules of the kidney, is the primary control point for Vitamin D activation and is tightly regulated by PTH, calcium, and phosphate levels.
Calcitonin, FGF23 & Integration - Fine-Tuning Fluids
- Calcitonin:
- Source: Thyroid C-cells. Stimulus: ↑ Serum $Ca^{2+}$.
- Actions: ↓ bone resorption; minor ↑ renal $Ca^{2+}$ excretion.
- Net: Weak ↓ Serum $Ca^{2+}$. Minor role; Paget's marker/tx.
- FGF23 (Fibroblast Growth Factor 23):
- Source: Osteocytes. Stimuli: ↑ Serum $PO_4^{3-}$, ↑ Calcitriol.
- Cofactor: Klotho. Actions (Kidney): ↓ $PO_4^{3-}$ reabsorption (phosphaturia); ↓ 1α-hydroxylase → ↓ Calcitriol.
- Net: ↓ Serum $PO_4^{3-}$, ↓ Calcitriol.
⭐ FGF23 is the principal phosphaturic hormone. It primarily acts on kidneys to decrease phosphate reabsorption and inhibits 1,25-dihydroxyvitamin D synthesis.
- Integrated Hormonal Response:
- Low $Ca^{2+}$: ↑PTH, ↑Calcitriol.
- High $Ca^{2+}$: ↓PTH, ↓Calcitriol, ↑Calcitonin (minor).
- Low $PO_4^{3-}$: ↓FGF23, ↑Calcitriol.
- High $PO_4^{3-}$: ↑FGF23, ↓Calcitriol (via FGF23).
High‑Yield Points - ⚡ Biggest Takeaways
- PTH ↑ serum Ca²⁺ (bone, kidney) & ↓ serum PO₄³⁻ (kidney).
- Vitamin D (Calcitriol) ↑ both Ca²⁺ & PO₄³⁻ absorption (gut, kidney).
- Calcitonin ↓ serum Ca²⁺ by inhibiting osteoclasts (minor role).
- Primary hyperparathyroidism: ↑ PTH, ↑ Ca²⁺, ↓ PO₄³⁻; commonest cause of hypercalcemia.
- Hypoparathyroidism: ↓ PTH, ↓ Ca²⁺, ↑ PO₄³⁻; presents with tetany.
- CKD causes secondary hyperparathyroidism (↓ Vit D, ↑ PO₄³⁻, ↓ Ca²⁺).
- Pseudohypoparathyroidism: PTH resistance; ↓ Ca²⁺, ↑ PO₄³⁻, ↑ PTH (Albright's hereditary osteodystrophy).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more