

Intro & Impact - Little Ears, Big Deal
- Pediatric Hearing Loss (PHL): Impaired auditory function in infants and children, impacting sound perception. A common congenital condition.
- Prevalence: Affects 1-3 per 1000 live births; up to 1 in 50 for NICU graduates.
- Impact on Development: Profound. Delays can lead to:
- Impaired speech and language acquisition
- Reduced cognitive development
- Social-emotional difficulties
- Early Action is Key: Timely detection and intervention are vital.
- 📌 1-3-6 Rule: Screen by 1 month, Diagnose by 3 months, Intervene by 6 months.
⭐ The critical period for auditory pathway development underscores the urgency of the 1-3-6 month guidelines for optimal language acquisition.
Causes & Kinds - Why So Silent?
- Classification:
- Types: Conductive, Sensorineural (SNHL), Mixed.
- Onset: Congenital vs. Acquired.
- Timing (re: language): Pre-lingual vs. Post-lingual.
- Association: Syndromic vs. Non-syndromic.
- Etiology - Key Causes:
- Genetic: GJB2/Connexin 26 (📌 GJB2 - commonest genetic).
- Infections: CMV (most common congenital), 📌 TORCH (S).
- Perinatal: Hypoxia, hyperbilirubinemia.
- Ototoxic drugs, Trauma, Meningitis.
| Feature | Conductive (CHL) | Sensorineural (SNHL) |
|---|---|---|
| Site | Outer/Middle Ear | Inner Ear/Auditory Nerve |
| Weber | → Affected Ear | → Unaffected Ear |
| Rinne | BC > AC (Negative) | AC > BC (Positive) / ↓AC & BC |
⭐ Mutations in the GJB2 gene (encoding Connexin 26) are the most common cause of autosomal recessive non-syndromic sensorineural hearing loss in children.
Screening & Dx - Catching Quietness Early
- Universal Newborn Hearing Screening (UNHS): Early detection via staged screening.
Loading diagram…
-
Key Tests:
- Otoacoustic Emissions (OAE): TEOAE, DPOAE. Tests outer hair cell function. Initial screen. 📌 OAE: Outer hair cells.
- Auditory Brainstem Response (ABR/BERA): Screening AABR, Diagnostic ABR. Assesses auditory pathway integrity. Confirmatory. 📌 ABR: Auditory pathway Brainstem Response.
-
Behavioral Audiometry (Age-Specific):
Test Age Range BOA < 6 months VRA 6 months - 2.5 years CPA 2.5 - 5 years Conventional > 5 years -
Tympanometry: Assesses middle ear function.

⭐ Otoacoustic emissions (OAEs) screen outer hair cell function; Auditory Brainstem Response (ABR) confirms auditory pathway integrity up to the brainstem.
Syndromes Spotlight - Name That Tune-Loss
| Syndrome | HL Type | Key Features |
|---|---|---|
| Usher Syndrome | SNHL | Retinitis Pigmentosa. 📌 Can't see, can't hear |
| Pendred Syndrome | SNHL | Goiter, Mondini malformation. 📌 Puffy neck, Poor hearing |
| Waardenburg Syndrome | SNHL | Pigmentary anomalies (white forelock, heterochromia), dystopia canthorum. 📌 White hair, Wide eyes, Wonky hearing |
| Alport Syndrome | SNHL | Renal disease, ocular issues. |
| Jervell and Lange-Nielsen Syndrome | SNHL | Long QT interval, syncope. |
| BOR Syndrome | Mixed/CHL/SNHL | Branchial anomalies (fistulae/cysts), Otologic anomalies (pits/tags), Renal anomalies. |
| Treacher Collins Syndrome | CHL | Craniofacial anomalies (mandibulofacial dysostosis), ear anomalies. |
⭐ Usher syndrome, characterized by sensorineural hearing loss and progressive retinitis pigmentosa, is the most common cause of combined deafness and blindness.
Management & More - Turning Up Volume
- Core Team: ENT, Audiologist, Speech Therapist.
- Amplification:
- Hearing Aids (HA): BTE/ITE for most HL.
- Bone Conduction Devices (BAHA): For conductive/mixed HL.
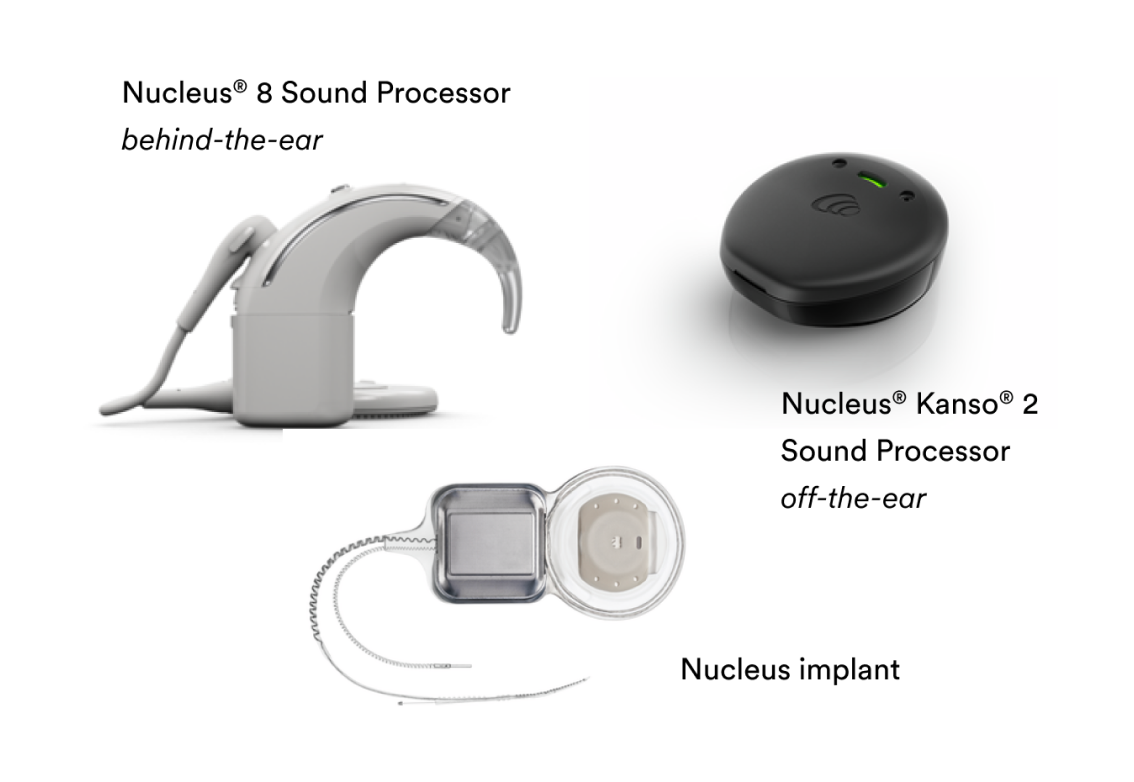
- Cochlear Implants (CI): For severe-profound SNHL.
- Candidacy: Bilateral SNHL >90 dB, poor HA trial, age (e.g., >12 mo).
- Therapy: Auditory Verbal Therapy (AVT)/Speech Therapy.
- Other Rx: PE tubes for OME.
| Device | Mechanism | Indication (SNHL) |
|---|---|---|
| Hearing Aids | Acoustic amplification | Mild to Severe |
| Cochlear Implants | Electrical stimulation (auditory nerve) | Severe-Profound (>90 dB) |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||
| flowchart TD |
HL["👂 Hearing Loss
• Sensory deficit• Clinical concern"]
SNHL_DEG["📋 Degree SNHL
• Audiogram check• Assess severity"]
HA_BENEFIT["📋 Adequate HA?
• Functional gain• Speech scores"]
HA_TRIAL["💊 Hearing Aids
• Trial period• Amplification"]
CI_EVAL["🔬 Cochlear Eval.
• Surgical screen• Implant candidacy"]
THERAPY["💊 Speech Therapy
• AVT sessions• Communication"]
HL --> SNHL_DEG SNHL_DEG -->|Mild-Severe| HA_TRIAL SNHL_DEG -->|Severe > 90dB| HA_BENEFIT
HA_BENEFIT -->|Yes| HA_TRIAL HA_BENEFIT -->|No| CI_EVAL
HA_TRIAL --> THERAPY CI_EVAL --> THERAPY
style HL fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style SNHL_DEG fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style HA_BENEFIT fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style HA_TRIAL fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style CI_EVAL fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style THERAPY fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534

> ⭐ **Cochlear implantation** is indicated for children with bilateral severe to profound sensorineural hearing loss who receive limited benefit from appropriately fitted hearing aids, ideally before the critical period of language development closes.
## High‑Yield Points - ⚡ Biggest Takeaways
> * **Genetic factors** (e.g., **Connexin 26**) are the **leading cause** of **congenital hearing loss**.
> * **TORCH infections** significantly cause **non-hereditary sensorineural hearing loss (SNHL)** in newborns.
> * **OAE** and **ABR (BERA)** are crucial for **newborn hearing screening**.
> * **Intervention before 6 months** is vital for **optimal language development**.
> * **Otitis Media with Effusion (OME)** is the **most frequent cause** of **childhood conductive hearing loss**.
> * **Cochlear implants** are for **severe-profound bilateral SNHL** unresponsive to hearing aids.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more