

Hypopharynx 101 - Cancer's Entry Point
- Definition: Malignancy of the hypopharynx (lowest part of pharynx: pyriform sinus, postcricoid area, posterior pharyngeal wall).
- Indian Epidemiology: High incidence, especially in males; linked to tobacco/betel quid.
- Key Risk Factors:
- Tobacco (smoking/chewing) & Alcohol (synergistic ↑↑ risk)
- Nutritional deficiencies (Iron: Plummer-Vinson Syndrome; Vitamins A, C, E)
- HPV: Less common than oropharynx (approx. 5-10% positive).
- 📌 Mnemonic: PATH to cancer - Plummer-Vinson, Alcohol, Tobacco, HPV.

⭐ Over 90-95% of hypopharyngeal cancers are Squamous Cell Carcinomas (SCC).
Anatomic Hotspots - Where Trouble Brews
Hypopharynx: Hyoid (sup.) to cricopharyngeus (inf.); larynx (ant.) to prevertebral fascia (post.). 📌 PPP Subsites:
- Pyriform Sinus (PS): ~60-70% (most common). Lateral to larynx. Spread: thyroid cartilage, paraglottic. Nodes: jugulodigastric. Symptoms: dysphagia, otalgia.
- Postcricoid (PCA): ~20-25%. Behind cricoid. Spread: esophagus; Plummer-Vinson link. Nodes: paratracheal. Symptoms: progressive dysphagia.
- Posterior Wall (PPW): ~10-15%. Vallecula to cricopharyngeus. Spread: prevertebral fascia. Nodes: retropharyngeal. Symptoms: dysphagia, odynophagia.
⭐ The pyriform sinus is the most common subsite for hypopharyngeal cancer, often presenting with referred otalgia.
Symptom Spotlight - Whispers of Disease
- Late presentation is common; early stages are often 'silent'.
- Key symptoms (📌 DOWNHill mnemonic):
- Dysphagia: Progressive (solids then liquids); prominent in post-cricoid.
- Otalgia: Referred (CN IX/X); an early sign in pyriform sinus lesions.
- Weight loss: Significant and unexplained.
- Neck mass: Often the first sign (nodal metastasis).
- Hoarseness: Indicates laryngeal involvement.
- Also: Persistent sore throat, foreign body sensation, odynophagia.
⭐ Referred otalgia is a significant early symptom in pyriform sinus cancers due to sensory innervation by Arnold's nerve (auricular branch of vagus).
Detective Work - Unmasking the Foe
- Clinical Evaluation:
- Indirect Laryngoscopy (Mirror).
- Flexible Nasopharyngolaryngoscopy (NPL).
- Gold Standard Diagnosis:
- Direct Laryngoscopy & Hypopharyngoscopy (DLH) with Biopsy under General Anesthesia (GA).
- Imaging for Staging:
- CECT (Neck & Chest): Assesses primary tumor extent, nodal status, and chest metastases.
- MRI: Superior soft tissue detail, perineural invasion (PNI).
- PET-CT: Detects distant metastases, synchronous second primaries (SSP), and recurrence.
- Final Assessment:
- TNM Staging (AJCC 8th Ed.).
- Panendoscopy: To rule out SSPs.
Loading diagram…
⭐ Hypopharyngeal cancers have a high propensity for early submucosal spread and bilateral cervical lymph node metastasis.
Battle Plan - Attack & Conquer
MDT approach is crucial. Goals: Maximize cure, preserve function (organ preservation strategies using primary RT or CRT).
- Core Modalities:
- Surgery: Total/Partial Laryngopharyngectomy, Neck Dissection.
- Radiotherapy (RT): EBRT/IMRT, definitive or adjuvant. Typical dose ~70 Gy.
- Chemotherapy: Cisplatin-based. Concurrent (CRT), induction, or palliative.
- Stage-Adapted Strategy: (See flowchart for early vs. advanced disease)
Loading diagram…
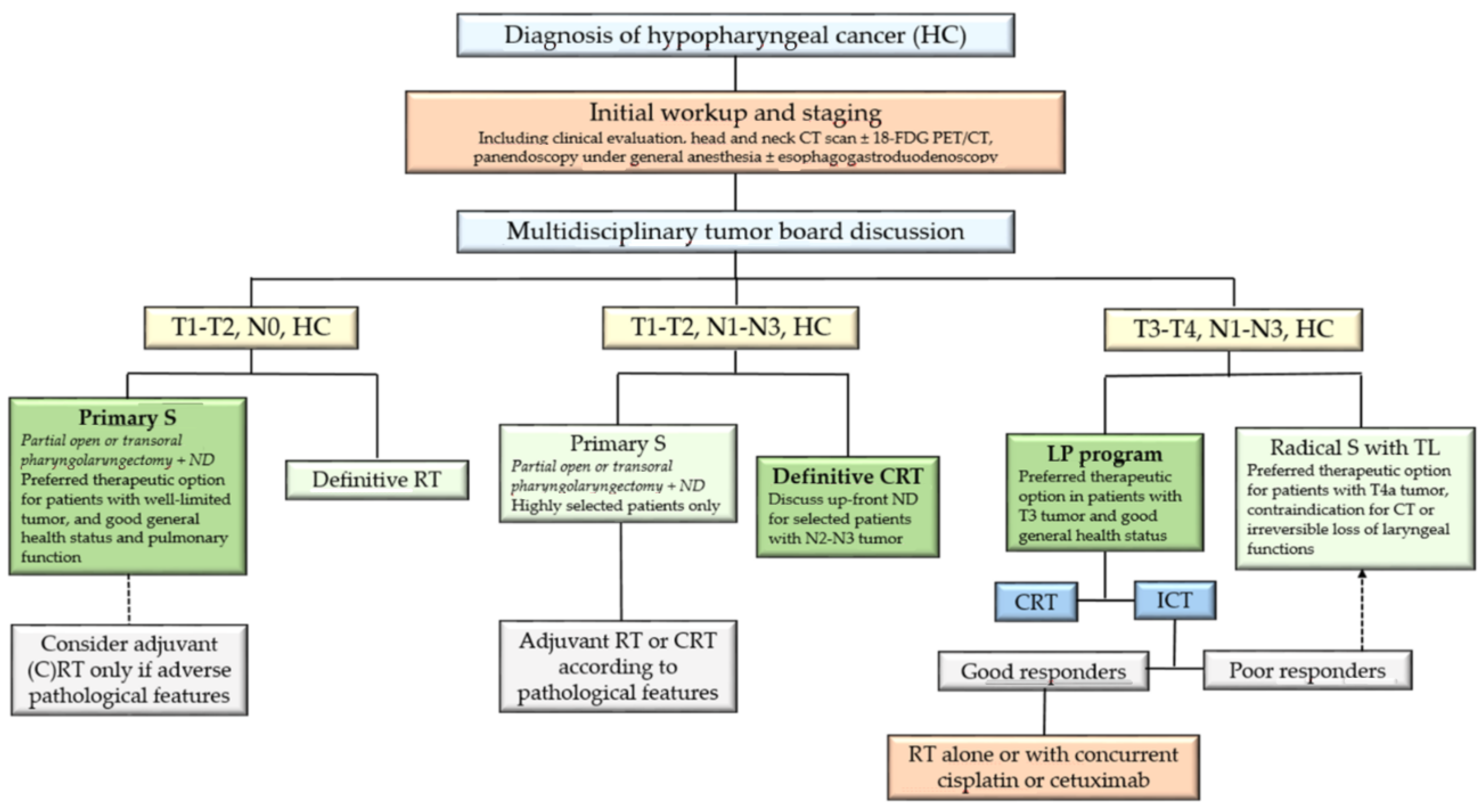
> ⭐ Concurrent Chemoradiotherapy (CCRT) is standard for most locally advanced, resectable hypopharyngeal cancers aiming for organ preservation.
- Unresectable/Metastatic Disease: Palliative care is paramount.
High‑Yield Points - ⚡ Biggest Takeaways
- Pyriform sinus is the most common site of hypopharyngeal cancer.
- Smoking and alcohol are the strongest synergistic risk factors.
- Late presentation is typical: dysphagia, referred otalgia, neck mass.
- High incidence of early cervical lymph node metastasis, often bilateral.
- Prognosis is generally poor due to late detection and aggressive nature.
- Treatment is usually multimodal: surgery (total laryngopharyngectomy) and radiotherapy.
- Postcricoid cancer is linked to Plummer-Vinson syndrome, especially in females.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more