

Overview: Premalignant Lesions - Danger Signs
- Precursors to invasive carcinoma (SCC > BCC).
- Etiology: Chronic UV exposure (main), HPV, arsenic, radiation, immunosuppression, chronic inflammation, genetic (XP).
- Monitor for malignant transformation.
- Danger Signs (Transformation):
- Rapid ↑ in size
- Ulceration, bleeding, crusting
- Induration, nodularity
- Persistent inflammation
- Pain or tenderness
- Color change

⭐ Bowen's disease (SCC in situ) has a 5-10% risk of progressing to invasive SCC if untreated.
Actinic Keratosis - Sun's Kiss
- Aka Solar Keratosis; most common premalignant skin lesion.
- Etiology: Chronic UV exposure (esp. UVB) → p53 mutations.
- Risk Factors: Fair skin (Fitzpatrick I/II), ↑age, male, immunosuppression, outdoor work.
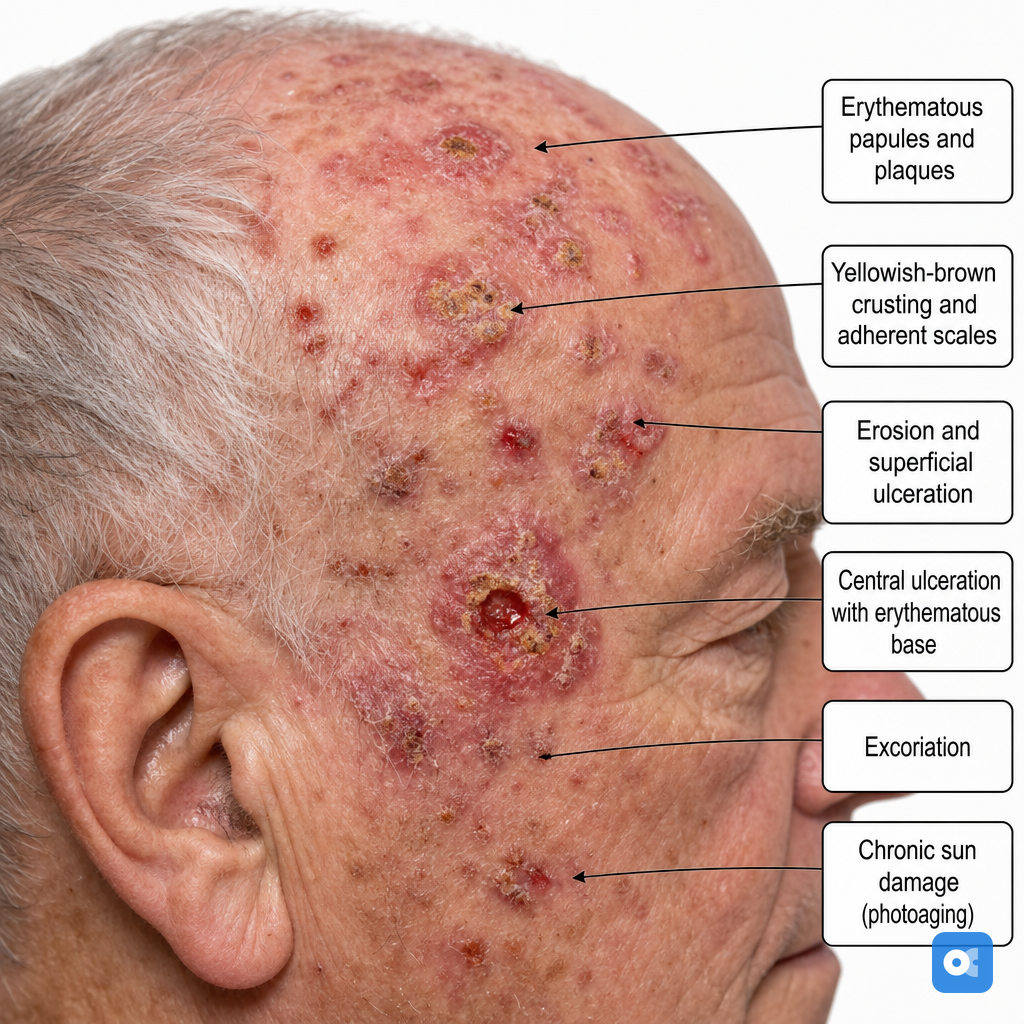
- Clinical:
- Ill-defined, erythematous, scaly papules/plaques (<1 cm).
- "Sandpaper" texture.
- Sun-exposed sites: face, bald scalp, ears, dorsum hands/forearms.
- Variants: Hypertrophic, atrophic, pigmented, cutaneous horn.
- Progression: Risk of Squamous Cell Carcinoma (SCC) ~0.025-16% per lesion/year.
⭐ Multiple AKs indicate field cancerization, significantly increasing SCC risk.
- Diagnosis: Clinical; biopsy if suspicious (induration, pain, bleeding, rapid growth, >1 cm).
- Management:
Loading diagram…
- Prevention: Sunscreen, protective clothing. 📌 Mnemonic: "Sun's Kiss can turn Nasty (SCC)".
Bowen's & Erythroplasia - Red Alert
-
Bowen's Disease (BD): SCC in situ (intraepidermal).
- Etiology: HPV (esp. 16, 18), arsenic, UV, immunosuppression.
- Clinical: Solitary, sharply defined, erythematous, scaly patch/plaque.
- Histo: Full-thickness epidermal atypia, intact basement membrane.
- Risk: ~3-5% to invasive SCC.
- 📌 Mnemonic: Bowen's: Border sharp, Often HPV/arsenic, Whole epidermis atypical, Erythematous Nasty Scale.
-
Erythroplasia of Queyrat (EQ): SCC in situ of glans/prepuce (BD variant).
- Etiology: HPV (esp. 16), uncircumcised, poor hygiene.
- Clinical: Well-defined, velvety, shiny, erythematous plaque.
- Histo: Same as BD (full-thickness atypia).
- Risk: Higher, ~10-33% to invasive SCC.
- 📌 Mnemonic: EQ: Erythematous Queyrat (glans) plaque, HPV's mark.
⭐ Erythroplasia of Queyrat carries a significantly higher risk (
10-33%) of progressing to invasive squamous cell carcinoma compared to cutaneous Bowen's disease (3-5%).
Other Precursors (Leukoplakia, etc.) - Rogues' Gallery
- Leukoplakia:
- White patch/plaque, non-scrapable.
- Oral: Associated with tobacco, alcohol, HPV. Vulval: VIN precursor.
- Risk: Squamous Cell Carcinoma (SCC).
- Arsenical Keratosis:
- Cause: Chronic arsenic exposure.
- Appearance: Multiple, firm, yellowish, hyperkeratotic papules/plaques.
- Sites: Palms, soles, trunk.
- Risk: SCC, Basal Cell Carcinoma (BCC), Bowen's disease.
- Radiation Keratosis (Chronic Radiodermatitis):
- Cause: Ionizing radiation; long latency (often >10 years).
- Features: Atrophy, telangiectasia, hyper/hypopigmentation, keratotic papules.
- Risk: SCC.
- Keratoacanthoma (KA):
- Growth: Rapidly growing, dome-shaped nodule with central keratin plug. Sun-exposed areas.
- Nature: Controversial; often self-regressing but frequently treated as well-differentiated SCC. 📌 KA = Keratin crater, Acts fast.
⭐ Proliferative Verrucous Leukoplakia (PVL) is a high-risk form of oral leukoplakia with a very high rate of malignant transformation to SCC (often >70%).
High‑Yield Points - ⚡ Biggest Takeaways
- Actinic Keratosis (AK): Most common premalignant lesion; UV-induced, sandpaper texture; risk of SCC.
- Bowen's Disease: SCC in situ; full-thickness atypia; associated with HPV, arsenic.
- Leukoplakia: White mucosal patch, non-scrapable; oral form has malignant potential.
- Keratoacanthoma (KA): Rapid growth, central keratin plug; often excised, mimics SCC.
- Arsenical Keratoses: Multiple palmar/plantar lesions from chronic arsenic; high SCC risk.
- Cutaneous Horn: Conical keratin; biopsy base to exclude underlying SCC or AK.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more