

FHR Monitoring Basics - Heartbeat Hints
- Goal: Detect fetal hypoxia & acidosis to prevent injury.
- Methods:
- Intermittent Auscultation (IA): Fetoscope/Doppler; for low-risk.
- Continuous Electronic Fetal Monitoring (EFM/CTG): External (ultrasound, toco) or internal (scalp electrode, IUPC).
- FHR Control:
- Autonomic Nervous System: Sympathetic (↑FHR), Parasympathetic (↓FHR, dominant).
- Chemoreceptors: Respond to fetal $O_2$, $CO_2$, pH changes.
- Baroreceptors: Respond to fetal blood pressure.
⭐ The most common cause of decreased FHR variability is fetal sleep cycle (lasting 20-40 minutes).
CTG Components - Tracing Tales
Cardiotocography (CTG) assesses fetal well-being. Key components:
- Baseline Fetal Heart Rate (FHR): Average FHR over 10 min.
- Normal: 110-160 bpm
- Bradycardia: < 110 bpm
- Tachycardia: > 160 bpm
- Variability: Fluctuations in FHR around baseline.
- Absent: Undetectable
- Minimal: ≤ 5 bpm
- Moderate (Normal): 6-25 bpm
- Marked: > 25 bpm
- Accelerations: Abrupt ↑ FHR (≥15 bpm for ≥15s if ≥32w; ≥10 bpm for ≥10s if <32w). Reassuring.
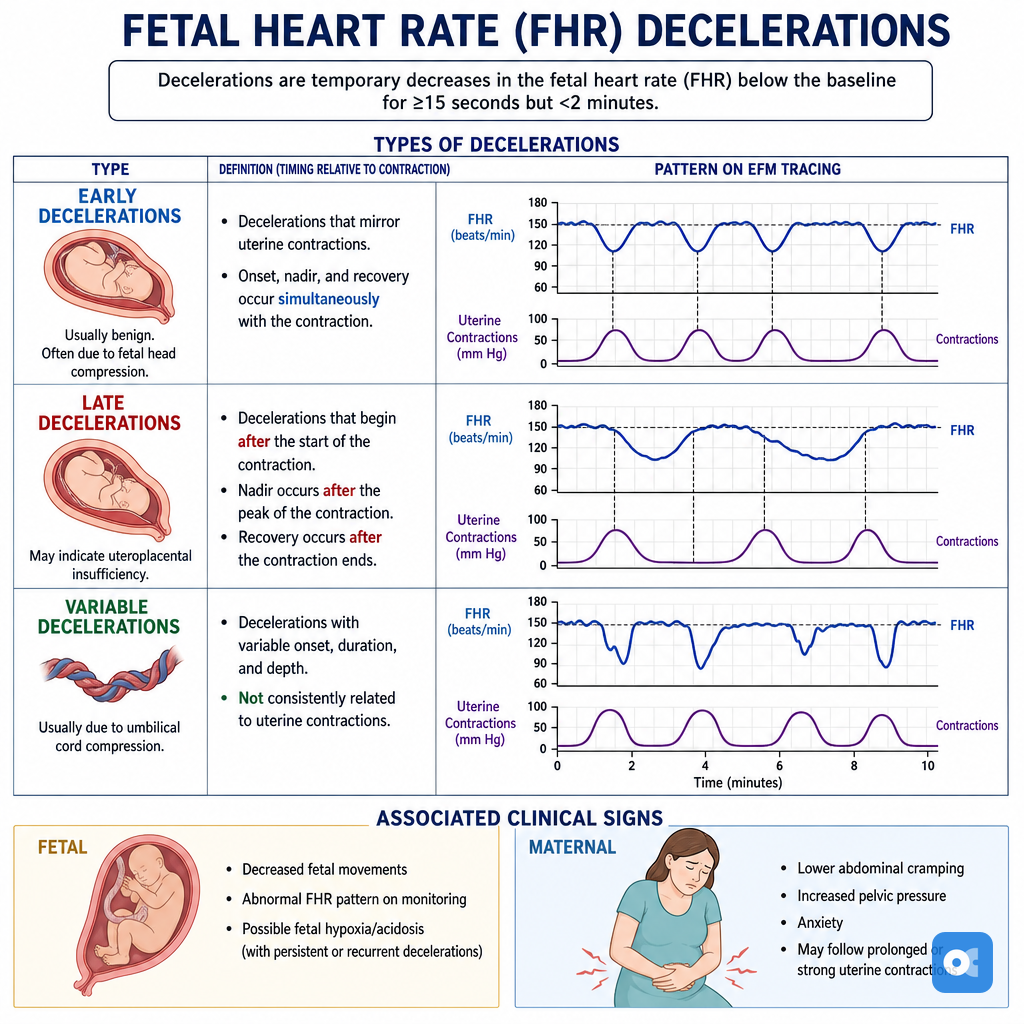
- Decelerations: Transient ↓ FHR.
- 📌 VEAL CHOP Mnemonic:
- Variable → Cord Compression
- Early → Head Compression
- Acceleration → Okay
- Late → Placental Insufficiency
- 📌 VEAL CHOP Mnemonic:
Loading diagram…
- Sinusoidal Pattern: Smooth, sine-wave like, 3-5 cycles/min, amplitude 5-15 bpm. Ominous (severe fetal anemia/hypoxia).
⭐ Late decelerations are the most ominous pattern, indicating significant fetal hypoxic stress due to uteroplacental insufficiency.
CTG Interpretation - Code Red or Green?
- Systematic approach: DR C BRAVADO (Define Risk, Contractions, Baseline Rate, Variability, Accelerations, Decelerations, Overall).
- FIGO 2015 3-Tier System:
Category Key Criteria Normal Baseline 110-160 bpm, Variability 5-25 bpm, No repetitive decelerations. Accelerations present. Suspicious One non-reassuring feature (e.g., baseline 100-109; variability <5 for 30-50 min), others normal. Pathological ≥2 non-reassuring, sinusoidal pattern, bradycardia <100, or prolonged deceleration >3 min.
⭐ Sinusoidal pattern is ominous, strongly associated with severe fetal anemia or hypoxia.
Fetal Distress Management - Rescue Rangers
- Non-Reassuring Fetal Status (NRFS): Clinical signs suggesting fetal hypoxia or acidosis.
- Common Causes: Placental insufficiency, cord compression, maternal hypotension, uterine tachysystole.
- Signs of Distress:
- CTG: Pathological trace (e.g., persistent late decelerations, absent variability, bradycardia, sinusoidal pattern).
- Meconium-stained amniotic fluid (MSAF).
- Fetal acidosis: Scalp $pH$ < 7.20.
- Intrauterine Resuscitation (📌 LIONS):
- Left lateral maternal position.
- IV fluid bolus.
- Oxygen administration (5-10 L/min via non-rebreather mask).
- Stop uterotonics (e.g., oxytocin).
- Consider Tocolysis (e.g., terbutaline 0.25 mg SC) if uterine tachysystole is present.
- Fetal Scalp Blood Sampling (FSBS): If NRFS persists and delivery is not imminent. $pH$ < 7.20 or $lactate$ > 4.8 mmol/L indicates significant acidosis requiring intervention.
- Urgent/Emergent Delivery: Indicated for persistent NRFS despite resuscitative measures or confirmed significant fetal acidosis.
⭐ Persistent late decelerations on CTG, especially when combined with reduced baseline variability, are highly indicative of uteroplacental insufficiency and fetal hypoxia, warranting prompt action.
High‑Yield Points - ⚡ Biggest Takeaways
- Normal FHR: 110-160 bpm. Moderate variability (6-25 bpm) is the most crucial sign of fetal well-being.
- Accelerations (↑15 bpm for ≥15s) are reassuring.
- Early decelerations indicate fetal head compression and are benign.
- Late decelerations suggest uteroplacental insufficiency and are ominous.
- Variable decelerations result from umbilical cord compression; severe ones are concerning.
- Sinusoidal pattern implies severe fetal anemia/hypoxia and is highly ominous.
- Address non-reassuring FHR patterns with intrauterine resuscitation (O2, fluids, position change).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more