

Upper Airways - Nose-to-Larynx Gateway
- Nasal Cavity:
- Septum: Vomer, perpendicular plate of ethmoid, septal cartilage.
- Conchae (Turbinates): Superior, Middle, Inferior. Meatuses & Sinus Openings:
- Sphenoethmoidal recess (above sup. concha): Sphenoid sinus.
- Superior meatus: Posterior ethmoidal air cells.
- Middle meatus: Frontal, Maxillary, Anterior & Middle ethmoidal air cells.
- Inferior meatus: Nasolacrimal duct.
- Blood Supply: Kiesselbach’s plexus (anterior epistaxis). Nerve Supply: CN I (olfaction), CN V1/V2 (sensation).
- Pharynx:
- Nasopharynx: Base of skull to soft palate. Contains pharyngeal tonsil (adenoids), Eustachian tube opening.
- Oropharynx: Soft palate to superior border of epiglottis. Contains palatine tonsils.
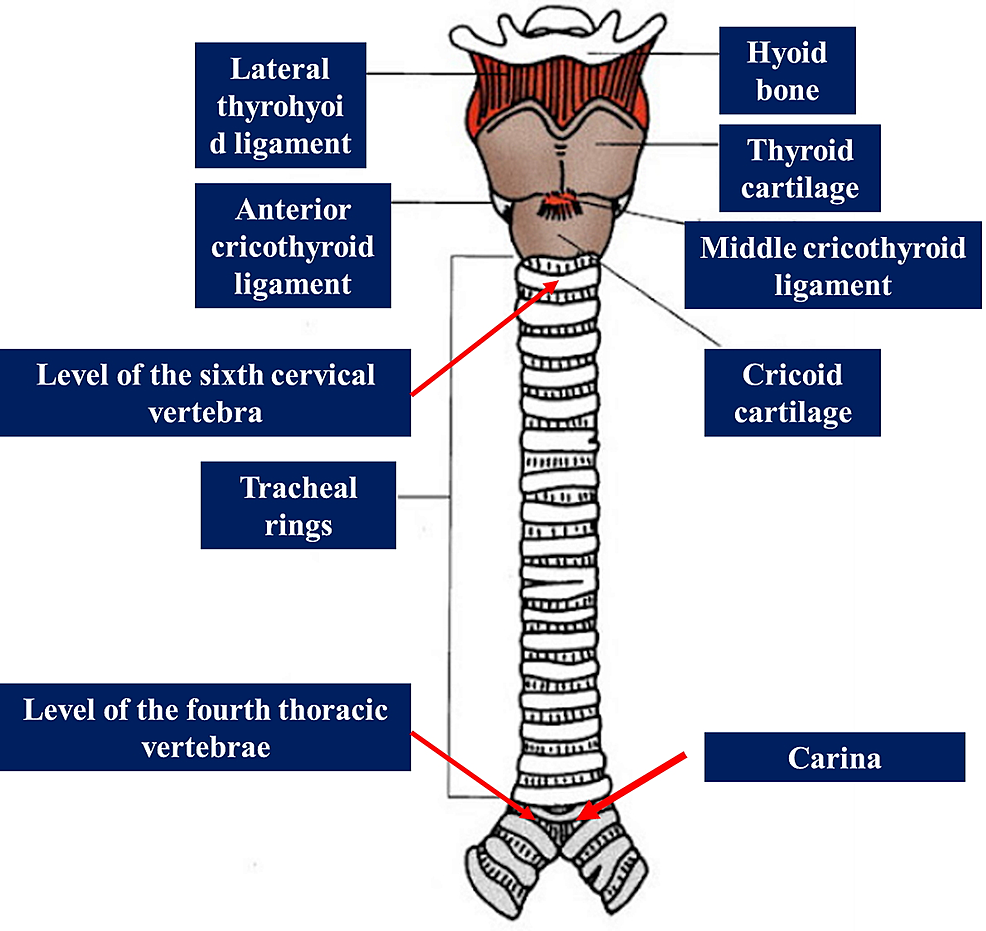
- Laryngopharynx: Superior border of epiglottis to inferior border of cricoid cartilage (vertebral level C6).
- Larynx (Voice Box):
- Cartilages: 📌 Unpaired (Thyroid, Cricoid, Epiglottis), Paired (Arytenoid, Corniculate, Cuneiform).
- Vocal Cords: True (sound production) & False (vestibular folds; protection).
- Nerve Supply:
- Superior Laryngeal Nerve: External branch (motor to cricothyroid), Internal branch (sensory above vocal cords).
- Recurrent Laryngeal Nerve: Motor to all intrinsic laryngeal muscles (except cricothyroid); sensory below vocal cords.
⭐ All intrinsic muscles of the larynx are supplied by the Recurrent Laryngeal Nerve (RLN) EXCEPT the Cricothyroid muscle, which is supplied by the External Laryngeal branch of the Superior Laryngeal Nerve.

Lower Airways - Trachea & Bronchial Tree
-
Trachea (Windpipe):
- Extent: Cricoid cartilage (C6) to carina (T4/T5, sternal angle); length 10-12 cm.
- Structure: 16-20 C-shaped hyaline cartilage rings anteriorly; posterior trachealis muscle (smooth muscle).
- Carina: Ridge at bifurcation (T4/T5); highly sensitive cough reflex.
-
Bronchial Tree - Branching Pattern:
Loading diagram…
-
Main (Primary) Bronchi:
- Right: Wider, shorter (~2.5 cm), more vertical (~25° angle to trachea).
- Left: Narrower, longer (~5 cm), more oblique (~45° angle to trachea).
⭐ Right main bronchus is wider, shorter, and more vertical; hence, inhaled foreign bodies are more likely to enter it. 📌 Mnemonic: "Inhale a bite? Goes down the Right."
-
Lobar (Secondary) Bronchi: Supply lobes.
- Right: 3 (Superior, Middle, Inferior).
- Left: 2 (Superior, Inferior).
-
Segmental (Tertiary) Bronchi: Supply bronchopulmonary segments (BPS).
- Right: 10 segmental bronchi.
- Left: 8-10 segmental bronchi.
- BPS: Smallest, functionally independent, surgically resectable lung unit.
-
Structural Changes Down the Tree:
- Cartilage: C-rings (trachea) → irregular plates (bronchi) → absent (bronchioles).
- Smooth Muscle: Relative amount ↑ as cartilage ↓.
- Epithelium: Pseudostratified ciliated columnar → ciliated simple columnar → ciliated simple cuboidal.
- Glands & Goblet cells: ↓ progressively, absent in terminal bronchioles.
Lungs & Pleura - Spongy Exchange Zones
- Lungs: Paired, essential for respiration.
- Right Lung: 3 lobes (Sup, Mid, Inf); 2 fissures (Oblique, Horizontal).
- Left Lung: 2 lobes (Sup, Inf); 1 fissure (Oblique); Lingula.
- Apex: Projects into neck. Base: On diaphragm.
- Hilum (Root):
- Contents: Main bronchus, pulmonary artery & veins, bronchial vessels, nerves, lymphatics.
- 📌 Mnemonic RALS: Pulmonary Artery is Right Anterior to bronchus, Left Superior to bronchus.
- Bronchopulmonary Segments (BPS):
- Surgically resectable units.
- Numbers: 10 in Right lung, 8-10 in Left lung.
- Pleura: Serous sac.
- Parietal: Lines chest wall, diaphragm, mediastinum. Nerve supply: Intercostal & Phrenic nerves.
- Visceral: Covers lungs.
- Pleural Cavity: Potential space; ~5-15 ml fluid.
- Recesses: Costodiaphragmatic (inferior), Costomediastinal (anterior).
⭐ Parietal pleura is sensitive to pain (somatic innervation); visceral pleura is insensitive (autonomic innervation).
Microanatomy & Support - Histo, Vessels, Nerves
-
Histology:
- Epithelium: Pseudostratified ciliated columnar → simple cuboidal (bronchioles) → simple squamous (alveoli).
- Club cells (bronchioles): Surfactant-like secretion, detox, stem cells.
- Alveolar cells:
- Type I pneumocytes: 95% surface, gas exchange.
- Type II pneumocytes: Surfactant (DPPC), ↓ surface tension, repair.
- Alveolar macrophages: Dust cells.
- Blood-Air Barrier (~0.5 µm): Surfactant, Type I cell, fused basal laminae, capillary endothelium.
⭐ Type II pneumocytes produce surfactant, reducing alveolar surface tension, preventing collapse.
-
Blood Supply:
- Pulmonary A.: Deoxygenated blood to lungs. Pulm V.: Oxygenated to heart.
- Bronchial A. (aorta): Supply lung tissue. Bronchial V.: Drain to azygos.
-
Innervation (Pulmonary Plexus):
- Sympathetic: Bronchodilation.
- Parasympathetic (Vagus): Bronchoconstriction, ↑ mucus.
-
Lymphatics: Superficial & deep plexuses → hilar → tracheobronchial nodes.
High‑Yield Points - ⚡ Biggest Takeaways
- Right lung: 3 lobes. Left lung: 2 lobes & lingula.
- Tracheal bifurcation at carina (T4-T5 vertebral level).
- Type II pneumocytes produce surfactant, preventing alveolar collapse.
- Diaphragm (phrenic nerve C3-C5) is chief inspiratory muscle.
- Pulmonary artery to bronchus: RALS (Right Anterior, Left Superior).
- Aspiration: commonest in RUL posterior segment (supine), RLL superior segment (erect).
- Pancoast tumor (lung apex) can cause Horner's syndrome (ptosis, miosis, anihidrosis).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more