

Congenital Malformations - Shaping Gone Wrong
- Definitions:
- Malformation: Primary structural defect; abnormal development (e.g., cleft lip).
- Deformation: Altered shape by mechanical forces (e.g., clubfoot from oligohydramnios).
- Disruption: Secondary breakdown of/interference with an originally normal developmental process (e.g., amniotic band syndrome).
- Dysplasia: Abnormal cell organization into tissues (e.g., achondroplasia).
Peak teratogen sensitivity: Weeks 3-8 (organogenesis).
Major Teratogens & Effects:
| Teratogen | Key Effects |
|---|---|
| 📌 TORCH | (Toxoplasmosis, Other, Rubella, CMV, HSV) |
| Alcohol | Fetal Alcohol Syndrome (FAS) |
| Thalidomide | Phocomelia (limb defects) |
| Valproate | Neural tube defects (e.g., spina bifida) |
| Warfarin | Skeletal abnormalities (nasal hypoplasia) |
- Chromosomal abnormalities (e.g., Down syndrome - Trisomy 21).
- Single gene mutations (e.g., Marfan syndrome).

⭐ The period of organogenesis, from week 3 to week 8 post-conception, is when the embryo is most susceptible to teratogenic agents causing major congenital malformations.
Neural Tube Defects - Brain & Spine Glitches
- Neural tube closure failure (3rd-4th week gestation).
- Diagnosis: ↑ Maternal Serum Alpha-Fetoprotein (MSAFP), ↑ Amniotic Fluid AFP & Acetylcholinesterase (AChE) (except spina bifida occulta). Ultrasound confirmation.
- Prevention: Folic acid supplementation (400 µg/day for general population; 4 mg/day for high-risk, e.g., prior NTD).
Major Types:
-
Anencephaly:
- Absence of forebrain, overlying skull, and scalp.
- Fatal; often associated with polyhydramnios.
-
Encephalocele:
- Herniation of brain and/or meninges through a skull defect (cranium bifidum).
- Commonly occipital.
-
Spina Bifida: Defect in vertebral arch fusion.
Type Sac Contents Key Features & Associations AFP Spina Bifida Occulta None (skin often overlies defect) Often asymptomatic; may have skin tuft, dimple, lipoma. Normal Meningocele Meninges, Cerebrospinal Fluid (CSF) Spinal cord usually in normal position; deficits rare. ↑ Myelomeningocele Meninges, CSF, neural tissue (cord/roots) Neurological deficits below lesion; Arnold-Chiari II malformation common. ↑
⭐ Maternal intake of folic acid before conception and during early pregnancy significantly reduces the incidence of neural tube defects.
Cardiac Malformations - Heartbeat Blips
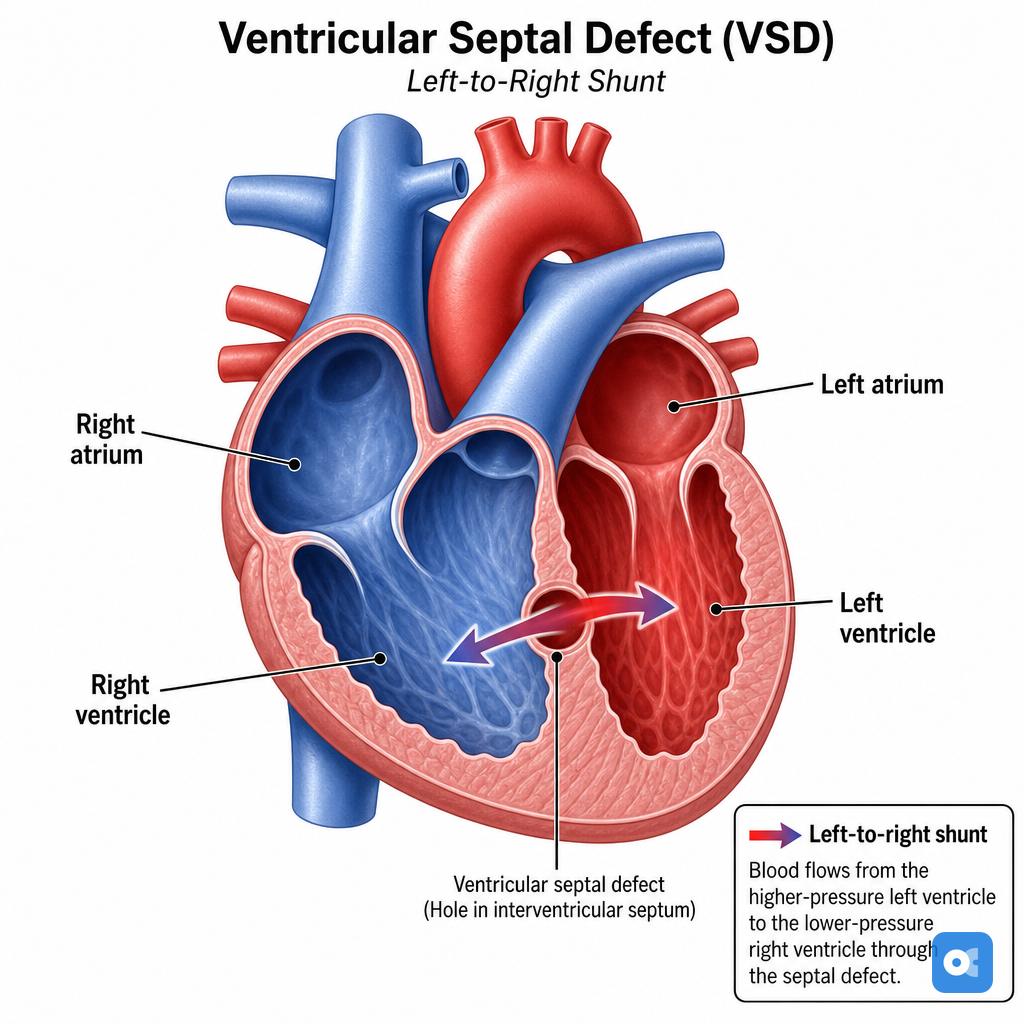
⭐ Ventricular Septal Defect (VSD) is the most common congenital heart defect overall, while Tetralogy of Fallot is the most common cyanotic congenital heart defect after the neonatal period.
| Defect Type | Shunt Direction | Key Feature | Examples |
|---|---|---|---|
| Acyanotic | L → R | ↑Pulm. blood flow, Late cyanosis (Eisenmenger's) | VSD, ASD, PDA, Coarctation of Aorta |
| Cyanotic | R → L | Early cyanosis | ToF, TGA, Truncus Arteriosus, Tricuspid Atresia |
- Ventricular Septal Defect (VSD): Most common. Holosystolic murmur.
- Atrial Septal Defect (ASD): Fixed wide split S2.
- Patent Ductus Arteriosus (PDA): Continuous machinery murmur. Close with **Indomethacin**; keep open with **Prostaglandin E1** for duct-dependent lesions.
- Coarctation of Aorta: Blood pressure difference (Upper Extremity > Lower Extremity). Rib notching on X-ray. Associated with Turner's syndrome.
- Cyanotic Defects (R→L Shunt):
- Tetralogy of Fallot (ToF): 📌 PROVe (Pulmonary stenosis, Right Ventricular Hypertrophy, Overriding aorta, VSD). Boot-shaped heart on X-ray. "Tet spells".
- Transposition of Great Arteries (TGA): Severe cyanosis from birth. "Egg on a string" appearance on X-ray. Prostaglandin E1 vital for survival pre-surgery.
- Truncus Arteriosus: Single arterial trunk supplies systemic, pulmonary, and coronary circulation.
- Tricuspid Atresia: Absence of tricuspid valve, hypoplastic right ventricle. Requires ASD and VSD/PDA for viability.
Loading diagram…
GI & GU Malformations - Gut & Kidney Quirks
- GI Malformations
- Tracheoesophageal fistula (TEF): Polyhydramnios. 📌 VACTERL (Vertebral, Anal, Cardiac, TEF, Renal, Limb).
- Pyloric Stenosis: Non-bilious projectile vomiting (2-8 wks), 'olive' mass.
⭐ Pyloric stenosis typically presents with non-bilious projectile vomiting in infants aged 2-8 weeks and a palpable 'olive-shaped' mass in the epigastrium.
- Hirschsprung Disease: Aganglionic megacolon; delayed meconium passage.
- Duodenal Atresia: 'Double bubble' sign on X-ray; associated with Down syndrome.
- Omphalocele vs. Gastroschisis:
Feature Omphalocele (Sac+) Gastroschisis (Sac-) Location Midline, umbilical ring Right of umbilicus (usu.) Bowel Normal Edematous, matted Anomalies Common (cardiac, chrom.) Less common (atresia)
- GU Malformations
- Hypospadias: Ventral urethral opening.
- Epispadias: Dorsal urethral opening; often with bladder exstrophy.
- Horseshoe Kidney: Fused lower poles; trapped by Inferior Mesenteric Artery.
- Posterior Urethral Valves (PUV): Male urethral obstruction; hydronephrosis.
- Renal Agenesis: Potter sequence (oligohydramnios → pulmonary hypoplasia, facial/limb defects).
High‑Yield Points - ⚡ Biggest Takeaways
- TORCH infections are major teratogenic agents causing diverse congenital malformations.
- Neural Tube Defects (NTDs) are largely preventable with maternal folic acid supplementation.
- Organogenesis (embryonic weeks 3-8) is the critical period for teratogen-induced malformations.
- VACTERL association is a recognized pattern of multiple congenital anomalies.
- Potter sequence, due to oligohydramnios, features pulmonary hypoplasia and characteristic facies.
- Amniotic band syndrome can cause constrictive defects, amputations, and fetal disruptions.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more