Back
USMLE Step 3 Preparation: Build an Adaptive Plan with Oncourse AI
Create an adaptive USMLE Step 3 study plan that adjusts based on your weak areas, CCS performance, and rotation schedule. Master biostatistics, ethics, and chronic disease management with targeted daily workflows.

USMLE Step 3 Preparation: Build an Adaptive Plan with Oncourse AI
You are probably staring at your residency calendar wondering how you'll fit Step 3 prep between 60-hour weeks and unpredictable calls. Unlike Step 1 or Step 2 CK, Step 3 cant be conquered with pure memorization—this exam demands clinical judgment, time management across 12 CCS cases, and the ability to synthesize information while exhausted.
The secret isnt studying harder. Its building an adaptive plan that responds to your performance data daily.
Most residents approach Step 3 like a loose pile of question blocks. They do 50 questions one day, skip two days because of calls, then panic-cram CCS cases the weekend before. This scattered approach fails because Step 3 tests integration—biostatistics application, ethical decision-making under pressure, and longitudinal chronic disease management—not isolated facts.
An adaptive USMLE Step 3 study plan solves this by turning your prep window into specific daily tasks that adjust based on your weak areas, remaining time, and rotation schedule. Instead of generic "do questions," you get "complete 40 internal medicine questions targeting chronic disease management, then review 2 CCS cases focusing on acute-to-chronic transitions."
Why Step 3 Demands Different Preparation
Step 3 isnt Step 2 CK with harder questions. Its a completely different beast testing whether you can practice independently without supervision.
Day 1 (Foundations of Independent Practice) hits you with 232 questions across 6 blocks, emphasizing biostatistics interpretation, research methodology, ethics in complex scenarios, and health systems management. These arent straightforward "what antibiotic" questions—they test whether you can read a pharmaceutical advertisement, identify statistical manipulation, and make evidence-based decisions under time pressure. Day 2 (Advanced Clinical Medicine) starts with 180 MCQs, then throws you into 12-13 CCS cases where you manage patients in real-time through a simulated EHR. You order labs, advance the clock, adjust medications based on results, and move patients between clinical settings. Cases can span minutes to months of simulated time.
The integration challenge becomes clear when you hit a CCS case about a diabetic patient with acute chest pain. You need biostatistics knowledge to interpret stress test results, ethical reasoning to handle family disagreement about invasive procedures, and chronic disease management skills to adjust the patient's diabetes medications during acute illness.
Most residents fail Step 3 because they compartmentalize these domains instead of practicing them together in realistic scenarios.
Core Components of Adaptive Step 3 Preparation
Daily Task Generation Based on Performance
Traditional study plans give you the same schedule regardless of whether you're crushing cardiology or struggling with biostatistics. An adaptive approach analyzes your practice performance and generates specific daily targets.
For example, if your analytics show 60% accuracy in biostatistics questions but 85% in cardiology, tomorrow's plan prioritizes 20 biostatistics questions, 3 CCS cases with statistical interpretation components, and targeted review of confidence intervals—not random mixed practice.
Oncourse's Daily Plan feature does exactly this conversion from "I need to study Step 3" into concrete daily actions based on your evolving performance data. Instead of wondering what to tackle during your 90-minute evening slot, you get specific tasks: "Complete IM questions 156-195, review missed ethics concepts from yesterday, complete CCS case #7 (chronic disease exacerbation)."
Weak Area Analytics for Strategic Focus
Step 3 covers 15 major organ systems plus biostatistics, ethics, and health systems. Without performance analytics, you cant identify which domains need intensive work versus light maintenance.
Effective weak area tracking goes beyond simple percentage scores. You need to identify patterns like "strong in acute management but weak in chronic disease follow-up" or "solid medical knowledge but poor CCS time management." These insights determine whether you need content review, more practice questions, or CCS-specific training.
The key is granular data. Instead of "70% in internal medicine," you want "cardiology acute management 85%, cardiology chronic management 62%, biostatistics interpretation in cardiology contexts 45%." This specificity prevents you from over-studying your strengths while neglecting critical gaps.
CCS Integration with Clinical Reasoning Support
CCS practice is where most residents stumble. The interface is clunky, cases are time-pressured, and the scoring algorithm penalizes both wrong orders and correct orders done too late.
Effective CCS preparation requires three components: software familiarity, clinical decision-making frameworks, and post-case analysis. You cant just "do more cases"—you need structured review of your decision patterns and timing.
This is where targeted case-based reasoning becomes crucial. After completing a CCS case about sepsis management, you need to understand not just which orders to place, but the optimal sequencing: blood cultures before antibiotics, lactate monitoring every 6 hours, vasopressor initiation criteria, and appropriate timing for ICU transfer decisions.
Clinical reasoning support through platforms like Oncourse's Clinical Rounds helps bridge this gap by providing structured analysis of case-based decision trees and explanation of why certain management sequences score better than others.
Building Your Adaptive Step 3 Workflow
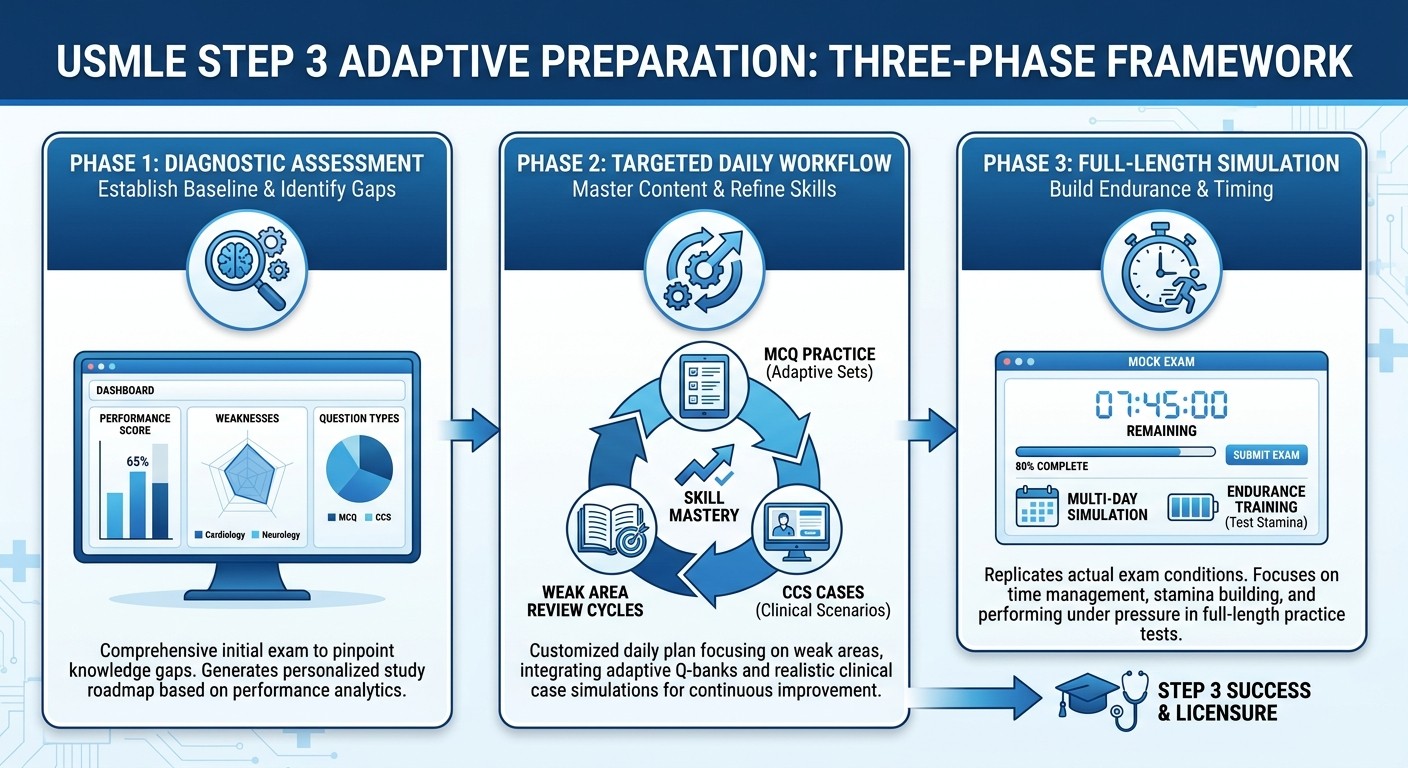
Phase 1: Baseline Assessment and Gap Analysis (Week 1)
Start with a comprehensive diagnostic assessment across all Step 3 domains. Take a 50-question mixed block covering biostatistics, ethics, and major clinical areas, plus complete 3-4 CCS cases spanning different acuity levels.
Your baseline isnt about the score—its about identifying specific knowledge gaps and skill deficiencies. Document every missed concept, timing error in CCS cases, and areas where you felt uncertain.
For biostatistics questions, track whether you struggled with study design interpretation, statistical test selection, or application to clinical scenarios. In ethics questions, note if issues involved informed consent, confidentiality, or professional boundaries. For CCS cases, analyze whether problems were medical knowledge, software navigation, or clinical sequencing.
This granular analysis forms the foundation of your adaptive plan. Instead of generic "review cardiology," you get specific targets like "reinforce biostatistics concepts in cardiology trials" or "practice acute-to-chronic transitions in cardiac patients."
Phase 2: Targeted Content and Practice Integration (Weeks 2-5)
Based on your baseline analysis, create focused daily workflows that combine content review, targeted practice questions, and CCS skill building.
A typical adaptive day might include:
Morning (30 minutes): 15 targeted questions in your weakest domain
Midday (15 minutes): Quick review of missed concepts using focused flashcards
Evening (45 minutes): 1 CCS case related to morning's question topics, followed by decision pattern analysis
The adaptive component means these targets shift based on your progress. If your biostatistics accuracy improves from 60% to 75%, the plan reduces biostatistics questions and increases focus on your next weakest area.
For example, if you initially struggled with chronic kidney disease management, your plan might assign 3 nephrology CCS cases this week. As your performance improves, next week shifts to pediatric cases or psychiatric scenarios based on your updated analytics.
Phase 3: Integration and Simulation (Weeks 6-8)
The final phase emphasizes full-length practice and exam simulation under realistic conditions. This isnt just about endurance—its about testing your adaptive decision-making when facing unexpected question patterns or challenging CCS scenarios.
Complete full-length practice exams (both MCQ blocks and CCS sections) under timed conditions. More importantly, analyze your performance patterns during these simulations. Do you make more errors in the final blocks when fatigued? Do you rush through CCS cases or spend too much time on early decisions?
This phase should confirm that your adaptive preparation successfully addressed your initial weak areas and that you can maintain performance across both testing days.
Conquering High-Yield Step 3 Domains
Biostatistics and Research Interpretation
Step 3 biostatistics questions dont test formula memorization—they assess your ability to interpret real research findings and apply them to patient care decisions.
Focus on these practical applications:
Study design recognition: Distinguishing case-control from cohort studies in clinical vignettes
Statistical significance vs clinical significance: When P<0.05 doesnt mean meaningful patient benefit
Screening test interpretation: Applying sensitivity, specificity, and predictive values to patient populations
Drug advertisement analysis: Identifying statistical manipulation in pharmaceutical marketing
Practice with questions that embed biostatistics within clinical scenarios. For example, interpreting whether a new cardiac marker adds clinical value beyond existing tests, or determining if a treatment's Number Needed to Treat justifies its cost and side effect profile.
The Oncourse platform's biostatistics and ethics lessons provide targeted practice with these integrated scenarios rather than isolated formula work.
Ethics in Complex Clinical Situations
Step 3 ethics questions go beyond basic consent and confidentiality. They test decision-making in gray areas where multiple ethical principles conflict.
High-yield scenarios include:
Capacity assessment: When patients can refuse treatment despite family objections
End-of-life decisions: Balancing autonomy, beneficence, and resource allocation
Professional boundaries: Managing conflicts of interest, dual relationships, and reporting obligations
Resource allocation: Making fair decisions when ICU beds or organs are limited
The key is practicing systematic ethical analysis: identify the ethical principles in conflict, consider stakeholder perspectives, and choose the course that best upholds patient autonomy while minimizing harm.
CCS Case Sequencing and Time Management
CCS success depends on developing consistent workflows that optimize both patient care and scoring algorithms.
Emergency presentations (chest pain, dyspnea, altered mental status): 1. Initial stabilization (0-2 minutes): Vitals, monitoring, IV access, oxygen if indicated 2. Immediate workup (2-5 minutes): Essential tests based on presentation (EKG, chest X-ray, basic labs) 3. Empiric treatment (5-10 minutes): Time-sensitive interventions while awaiting results 4. Results review and adjustment (10-15 minutes): Modify treatment based on initial data 5. Disposition and monitoring (15-20 minutes): Appropriate setting, follow-up plans Outpatient chronic disease management (diabetes, hypertension, COPD): 1. Current status assessment: Symptoms, adherence, home monitoring data 2. Targeted examination: Focus on disease-specific complications 3. Laboratory review: Trend analysis, not just current values 4. Medication optimization: Evidence-based adjustments with safety monitoring 5. Long-term planning: Lifestyle counseling, screening schedules, complication prevention
The timing matters as much as the content. Ordering the right antibiotic 10 minutes too late in a sepsis case costs significant points, while rushing through a stable diabetes case without proper counseling also reduces your score.
Chronic Disease Management Integration
Step 3 heavily emphasizes longitudinal patient care and chronic disease management across multiple encounters. Unlike acute presentations that focus on immediate diagnosis and treatment, chronic disease scenarios test your ability to adjust therapy over time, monitor for complications, and coordinate care across different settings.
Diabetes Management Across Care Transitions
CCS cases often present diabetes patients during acute illness, testing whether you can maintain chronic disease management while addressing immediate concerns.
Key decision points include:
Perioperative management: When to hold metformin, adjust insulin protocols, monitor for complications
Acute illness modifications: Stress-dose steroids in diabetic patients, sliding scale versus basal-bolus during hospitalization
Discharge planning: Ensuring medication reconciliation, follow-up scheduling, and complication screening
Practice scenarios where you manage a diabetic patient from ED presentation through hospital stay to discharge, adjusting medications at each transition point while maintaining appropriate monitoring.
Cardiovascular Risk Management
Step 3 expects you to apply evidence-based guidelines for cardiovascular prevention and chronic management, not just acute cardiac events.
Critical areas include:
Statin therapy decisions: Risk calculators, goal LDL levels, monitoring for side effects
Blood pressure management: Target goals in different populations, combination therapy strategies
Anticoagulation decisions: Balancing stroke prevention with bleeding risk in atrial fibrillation
CCS cases may present patients with multiple cardiovascular risk factors requiring simultaneous management decisions and long-term monitoring plans.
Daily Workflow Implementation
Morning Question Blocks (30-45 minutes)
Start each study day with targeted question practice based on your current weak areas. If analytics show poor performance in biostatistics, dedicate 20-30 questions to this domain rather than random mixed practice.
Use immediate review strategy: after completing a question block, spend equal time analyzing explanations for both correct and incorrect answers. This reinforces learning patterns and identifies knowledge gaps requiring additional review.
Focus on pattern recognition rather than individual facts. Step 3 questions often test the same underlying concepts through different clinical presentations, so identifying these patterns improves efficiency across multiple domains.
CCS Practice Sessions (20-30 minutes)
Complete 1-2 CCS cases daily, focusing on different clinical settings and acuity levels. Rotate between emergency presentations, inpatient management, and outpatient follow-up to build versatility.
After each case, conduct structured analysis:
Timeline review: Were critical orders placed with appropriate timing?
Setting management: Did you move the patient to the correct clinical environment?
Monitoring decisions: Were follow-up labs and vital signs checked appropriately?
Disposition planning: Was discharge or transfer handled with proper planning?
This analysis builds the clinical reasoning frameworks that improve performance across different case types.
Targeted Review and Reinforcement (15-20 minutes)
Use your weak area analytics to focus brief review sessions on specific concepts that appeared in morning question blocks or CCS cases.
Rather than broad chapter review, target specific topics like "confidence interval interpretation in therapeutic trials" or "capacity assessment in psychiatric patients." This focused approach maximizes retention while fitting into busy residency schedules.
Utilize spaced repetition for concepts that repeatedly appear as weak areas in your analytics. Brief daily exposure to challenging concepts builds long-term retention more effectively than intensive cramming sessions.
Advanced Integration Strategies
Multi-Domain Question Analysis
Step 3 questions frequently integrate multiple domains within single clinical scenarios. Develop skills to identify and address each component systematically.
For example, a question about starting a new diabetes medication might test:
Biostatistics: Interpreting trial data showing Number Needed to Treat
Ethics: Obtaining informed consent about potential side effects
Clinical management: Appropriate dosing and monitoring protocols
Health systems: Insurance coverage and cost considerations
Practice identifying these multi-domain questions and addressing each component methodically rather than focusing only on the primary clinical decision.
Time-Pressured Decision Making
Both MCQ blocks and CCS cases test your ability to make appropriate decisions under time constraints. This skill requires specific practice beyond content knowledge.
For MCQ sections, develop systematic approaches to eliminate obviously incorrect answers and make educated decisions when uncertain. Practice timed question blocks regularly to build stamina and pacing skills.
For CCS cases, practice consistent opening sequences that address immediate patient safety while gathering essential information efficiently. Develop mental templates for common presentations that allow rapid initial assessment and management.
Frequently Asked Questions
How long should I spend preparing for USMLE Step 3?
Most residents need 6-8 weeks of focused preparation, studying 15-25 hours weekly. Lighter schedules may extend to 12 weeks, while intensive preparation can compress to 4-5 weeks if you have lighter rotation duties. The key is consistent daily practice rather than sporadic long sessions.
What's the most efficient way to practice CCS cases?
Complete 30-40 CCS cases during your preparation, focusing on systematic analysis after each case rather than just volume. Spend equal time reviewing your decision patterns and timing as you do completing new cases. Practice with the actual CCS interface whenever possible to avoid day-of navigation issues.
How much time should I dedicate to biostatistics review?
Biostatistics comprises roughly 11-13% of Step 3 questions. Dedicate about 15% of your study time to biostatistics, emphasizing application to clinical scenarios rather than formula memorization. Focus on interpreting research findings and applying statistical concepts to patient care decisions.
Should I space Day 1 and Day 2 apart?
Many residents benefit from spacing the exam days 3-5 days apart, using the interval for focused CCS practice and MCQ review. This approach allows targeted preparation based on Day 1 performance while maintaining momentum. However, some prefer consecutive days to minimize overall exam stress.
How do I balance Step 3 prep with residency duties?
Build your study schedule around your rotation intensity. During demanding rotations, focus on brief daily question blocks (20-30 questions) and maintain consistency rather than attempting long study sessions. Use lighter rotation weeks for intensive CCS practice and comprehensive review.
What should I do if I'm consistently weak in specific domains?
Use targeted practice questions and focused content review for persistent weak areas. If biostatistics remains challenging after initial review, dedicate 40% of your daily questions to this domain until performance improves. Consider additional resources like Oncourse's targeted biostatistics lessons for structured reinforcement.
Building Long-Term Success Patterns
Step 3 preparation teaches valuable skills that extend beyond the exam itself. The analytical approach to identifying weak areas, systematic practice with performance feedback, and integration of multiple knowledge domains mirrors the clinical reasoning required for independent practice.
Your adaptive preparation workflow becomes a template for lifelong learning during residency and beyond. The same principles—targeted practice based on performance data, systematic analysis of clinical decisions, and integration across multiple domains—apply to board certification, continuing education, and clinical practice improvement.
The investment in building these analytical and systematic learning approaches pays dividends throughout your medical career, making Step 3 preparation valuable professional development beyond just exam passage.
Prepare smarter with Oncourse AI—adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 3. Download free on Android and iOS.