Back
USMLE Step 2 CK Pulmonology: High-Yield Topics, COPD vs Asthma Vignettes and Exam Strategy (2026)
Master USMLE Step 2 CK pulmonology with this complete guide covering COPD vs asthma differentiation, pneumonia antibiotic selection, PE workup algorithms, and high-yield vignette patterns for 2026.

USMLE Step 2 CK Pulmonology: High-Yield Topics, COPD vs Asthma Vignettes and Exam Strategy (2026)
You are probably staring at another pulmonology question, trying to figure out if that 67-year-old smoker with dyspnea has COPD exacerbation or heart failure. Or maybe you just got burned by a PE workup question because you picked CT-PA when the patient had renal dysfunction. Here's the thing: pulmonology makes up 8-12% of Step 2 CK questions, and the patterns are incredibly predictable once you know what to look for.
I scored 260+ on Step 2 CK, and pulmonology was my strongest subject — not because I memorized every drug mechanism, but because I cracked the vignette patterns. The exam tests clinical reasoning, not zebra diagnoses. Every COPD vs asthma question has the same decision points. Every pneumonia case follows the same workup logic. Every PE question tests your risk stratification.
This guide covers exactly what Step 2 CK tests: how to differentiate obstructive diseases through spirometry, when to use which imaging for pneumonia, how to navigate the PE workup without missing critical steps, and the clinical patterns that show up in 90% of pulmonology vignettes. No fluff, just the decision trees that get you points.
COPD vs Asthma: The Clinical Differentiation That Shows Up Everywhere
Step 2 CK loves putting these side by side because the management diverges completely. You cant treat a COPD exacerbation like asthma — different steroids, different bronchodilators, different monitoring.
Spirometry Patterns (Memorize These Numbers)
COPD spirometry:
FEV1/FVC ratio <0.70 (the key cutoff)
<12% reversibility with bronchodilator (defines fixed obstruction)
Reduced DLCO (emphysema destroys alveolar surface area)
Increased total lung capacity (air trapping)
Asthma spirometry:
FEV1/FVC ratio <0.80 during exacerbation
≥12% and 200mL improvement with bronchodilator (defines reversibility)
Normal DLCO between episodes
Normal lung volumes when controlled
The vignette will give you pre and post-bronchodilator values. Calculate the percent change: if FEV1 improves by 15-20%, think asthma. If it barely budges, think COPD. When practicing USMLE pulmonology MCQs, Oncourse's adaptive engine serves more spirometry interpretation questions when students struggle with this exact calculation.
Clinical Triggers and Presentations
COPD red flags:
Age >40 with 20+ pack-year smoking history
Progressive dyspnea over years (not episodic)
Chronic productive cough (usually morning)
Barrel chest, accessory muscle use
Exacerbations triggered by infections, not allergens
Asthma red flags:
Onset before age 40 (though adult-onset exists)
Episodic symptoms with trigger exposure
Nighttime awakening from cough/wheeze
Family history of asthma or allergies
Eczema, allergic rhinitis, nasal polyps
Step 2 CK often presents a mixed picture — 55-year-old smoker with episodic wheeze. The key is smoking history (COPD) vs reversibility pattern (asthma). Some patients have both.
Exacerbation Management (Where Students Get Tripped Up)
COPD exacerbation treatment:
Nebulized albuterol + ipratropium (NOT just albuterol)
Prednisolone 40mg daily x 5 days (short course)
Antibiotics if increased sputum purulence or fever
Consider NIV if pH 7.25-7.35 with hypercapnia
Asthma exacerbation treatment:
High-dose albuterol (ipratropium helps but not essential)
Prednisolone 1mg/kg (up to 80mg) x 5-7 days
No routine antibiotics unless pneumonia suspected
Consider magnesium sulfate for severe cases
The distinction: COPD patients need dual bronchodilation (beta-agonist + anticholinergic) because their obstruction is fixed. Asthma patients respond primarily to beta-agonists because their obstruction is inflammatory and reversible.
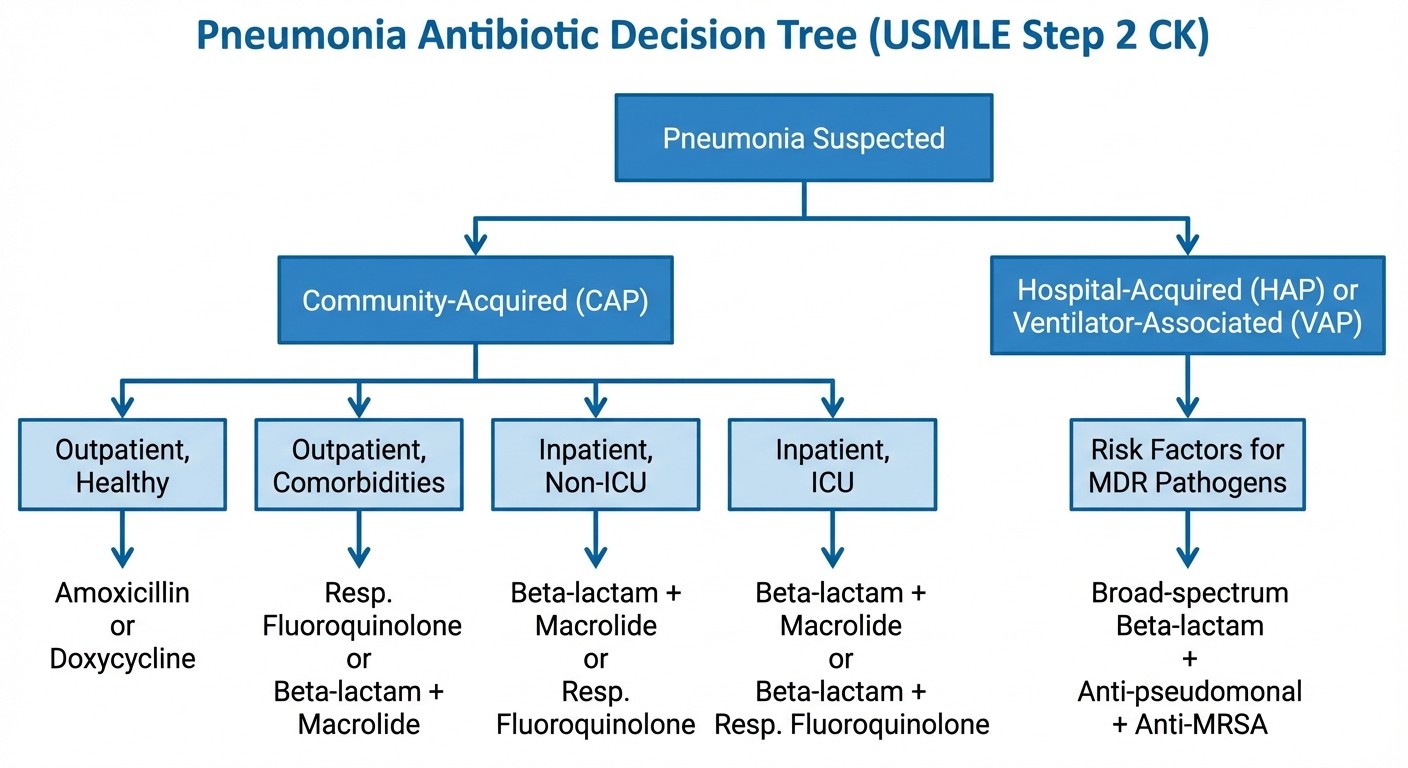
Pneumonia Vignettes: CAP vs HAP vs VAP Decision Trees
Pneumonia questions on Step 2 CK test your ability to choose the right antibiotic based on setting and risk factors. The patterns are rigid — memorize the decision points.
Community-Acquired Pneumonia (CAP)
Outpatient healthy patient:
First-line: amoxicillin 1g TID x 5 days
Macrolide allergy: doxycycline
Recent antibiotic use: fluoroquinolone
Outpatient with comorbidities (COPD, diabetes, heart disease):
Amoxicillin-clavulanate PLUS macrolide
OR fluoroquinolone alone
Inpatient non-ICU:
Ceftriaxone PLUS macrolide
OR fluoroquinolone alone
ICU pneumonia:
Beta-lactam (ceftriaxone, cefepime) PLUS macrolide
OR beta-lactam PLUS fluoroquinolone
Step 2 CK will describe a 45-year-old with fever, productive cough, and consolidation on chest X-ray. If they mention "works in an office" and no comorbidities, pick amoxicillin. If they mention COPD or diabetes, step up to combination therapy.
Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP)
HAP = pneumonia developing >48 hours after hospital admission
VAP = pneumonia in intubated patients >48-72 hours post-intubation
Risk factors for MDR organisms:
Recent IV antibiotic use (within 90 days)
Hospitalization ≥5 days
High local resistance rates
COPD with frequent exacerbations
Immunosuppression
HAP/VAP empiric therapy:
Low MDR risk: ceftriaxone or fluoroquinolone
High MDR risk: piperacillin-tazobactam OR cefepime OR meropenem PLUS vancomycin or linezolid
The vignette will tell you how long they've been hospitalized and whether they received antibiotics recently. Use spaced repetition flashcards to drill the HAP/VAP risk factors — these exact details determine the answer choice.
Imaging Decisions: CXR vs CT
Chest X-ray first for:
Typical pneumonia presentation
Young healthy patients
Clear clinical picture
Chest CT when:
CXR normal but high clinical suspicion
Complicated pneumonia (effusion, abscess)
Immunocompromised patients
Failed response to appropriate therapy
Step 2 CK often asks "what is the best next step" for a pneumonia workup. If the patient has classic symptoms, start with CXR. If they're immunocompromised or the CXR is negative, escalate to CT.
Pulmonary Embolism: Mastering the Wells Score and Imaging Cascade
PE questions are pure algorithm application. Step 2 CK gives you a clinical scenario, you calculate Wells score, and you follow the imaging pathway. No shortcuts, no clinical gestalt — just systematic evaluation.
Wells Criteria (Memorize the Point Values)
Clinical Feature | Points |
|---|---|
Clinical signs of DVT | 3 |
PE more likely than alternative diagnosis | 3 |
Heart rate >100 | 1.5 |
Immobilization >3 days or surgery within 4 weeks | 1.5 |
Previous PE/DVT | 1.5 |
Hemoptysis | 1 |
Cancer (active or within 6 months) | 1 |
Score interpretation:
≤4 points: PE unlikely
>4 points: PE likely
The subjective "PE more likely than alternative diagnosis" always trips students up. If the vignette presents clear evidence of pneumonia, heart failure, or another cause, dont give the 3 points. When working through pulmonology practice questions, Oncourse's AI explanations break down exactly how to score ambiguous clinical scenarios.
Imaging Algorithm
Wells ≤4 (PE unlikely):
1. Check D-dimer
2. If negative: stop workup
3. If positive: CT-PA
Wells >4 (PE likely):
1. Skip D-dimer, go straight to CT-PA
2. If CT-PA contraindicated: V/Q scan
CT-PA contraindications:
Renal dysfunction (creatinine >2.0 or eGFR <30)
Severe contrast allergy
Pregnancy (relative — V/Q preferred)
V/Q scan limitations:
Requires normal chest X-ray
COPD or other lung disease makes interpretation difficult
Often "intermediate probability" result
Step 2 CK will present a 35-year-old woman with pleuritic chest pain and tachycardia 2 weeks post-cesarean section. Calculate Wells (surgery +1.5, HR >100 +1.5, no other clear diagnosis +3 = 6 points). Skip D-dimer, order CT-PA. If they mention "creatinine 2.5," switch to V/Q scan.
Treatment Decisions
Anticoagulation:
Low bleeding risk: apixaban 10mg BID x 7 days, then 5mg BID
High bleeding risk or contraindication: IVC filter
Massive PE with shock: thrombolytic therapy (tPA)
Massive PE criteria:
Systolic BP <90 or drop >40 from baseline
Shock requiring vasopressors
Cardiac arrest
The anticoagulation choice depends on bleeding risk, not PE severity. A small PE in a patient with recent surgery might get an IVC filter. A large PE in a healthy patient gets full anticoagulation.
Pleural Effusion: Light's Criteria and Management Decisions
Pleural effusion questions test your ability to distinguish transudate from exudate and choose the appropriate next steps. The criteria are absolute — no clinical judgment required.
Light's Criteria for Exudate
Any one of these = exudate:
Pleural fluid LDH/serum LDH >0.6
Pleural fluid protein/serum protein >0.5
Pleural fluid LDH >2/3 upper limit of normal serum LDH
Transudate causes:
Heart failure (most common)
Cirrhosis
Nephrotic syndrome
Hypothyroidism
Exudate causes:
Pneumonia/parapneumonic effusion
Malignancy
PE
Autoimmune disease
Step 2 CK will give you pleural fluid values and ask you to classify. If pleural protein is 4.2 and serum protein is 7.0, calculate: 4.2/7.0 = 0.6. That meets criteria for exudate (>0.5), so look for infectious or malignant causes.
Parapneumonic Effusion Management
Simple parapneumonic effusion:
pH >7.30, glucose >60, LDH <1000
Treatment: antibiotics only
Complicated parapneumonic effusion:
pH 7.10-7.30, glucose 30-60, LDH >1000
Treatment: chest tube drainage
Empyema:
pH <7.10, glucose <30, positive gram stain/culture
Treatment: chest tube + fibrinolytics or surgery
The pH cutoff of 7.30 is critical. Above that, antibiotics work. Below that, you need drainage. When reviewing these cutoffs with pulmonology flashcards, the spaced repetition algorithm resurfaces weak cards until these exact numbers stick.
Interstitial Lung Disease: IPF vs Sarcoidosis vs Hypersensitivity Pneumonitis
ILD questions focus on pattern recognition. Each disease has characteristic clinical features, imaging findings, and demographics. Step 2 CK wont ask you to interpret HRCT directly, but theyll describe findings.
Idiopathic Pulmonary Fibrosis (IPF)
Demographics: Men >60, often with smoking history Clinical: Progressive dyspnea over months, dry cough, finger clubbing Imaging: Lower lobe honeycombing, minimal ground-glass Pulmonary function: Restrictive pattern, reduced DLCO Treatment: Antifibrotics (nintedanib, pirfenidone), lung transplant evaluation
Sarcoidosis
Demographics: Young adults, often African American women Clinical: Often asymptomatic, may have fever, arthritis, erythema nodosum Imaging: Bilateral hilar lymphadenopathy, upper lobe predominance Lab: Elevated ACE level, hypercalcemia Treatment: Corticosteroids for symptomatic disease
Hypersensitivity Pneumonitis
Demographics: Exposure history (farmer's lung, bird breeder's lung) Clinical: Acute symptoms after exposure, fever, chills Imaging: Ground-glass opacities, upper lobe predominance Lab: Positive precipitating antibodies Treatment: Exposure avoidance, corticosteroids
The key distinguishing features: IPF affects older smokers with lower lobe disease. Sarcoidosis affects younger patients with hilar adenopathy. HP requires exposure history with acute symptoms.
Lung Cancer: Presentation Patterns and Paraneoplastic Syndromes
Lung cancer questions usually test paraneoplastic syndromes or staging workup. Know the associations between cell types and endocrine effects.
Small Cell vs Non-Small Cell Patterns
Small Cell Lung Cancer (SCLC):
Central location, smoking history
Rapid growth, early metastasis
Paraneoplastic syndromes common
Treatment: chemotherapy (rarely surgical)
Non-Small Cell Lung Cancer (NSCLC):
Peripheral or central location
Slower growth
Surgical resection if early stage
Subtypes: adenocarcinoma, squamous cell
Paraneoplastic Syndromes (High-Yield)
SIADH (hyponatremia):
Most common with small cell
Mechanism: ADH production by tumor
Treatment: fluid restriction, demeclocycline
Cushing syndrome:
ACTH production by tumor
Rapid onset, severe symptoms
Bilateral adrenal hyperplasia on imaging
Hypercalcemia:
PTH-related protein production
More common with squamous cell NSCLC
Treatment: fluids, bisphosphonates
Eaton-Lambert syndrome:
Antibodies against voltage-gated calcium channels
Muscle weakness that improves with exercise
Associated with small cell
Step 2 CK presents a 65-year-old smoker with new onset weakness that improves after walking. Think Eaton-Lambert, look for lung mass. The exercise improvement distinguishes it from myasthenia gravis.
Obstructive Sleep Apnea: Risk Factors and Management
OSA questions are straightforward — recognize the clinical pattern and know when to order sleep studies vs when to start treatment.
Clinical Presentation
Symptoms:
Loud snoring with witnessed apneas
Morning headaches
Daytime sleepiness
Poor concentration
Risk factors:
Obesity (BMI >30)
Male gender
Age >40
Neck circumference >17 inches (men), >16 inches (women)
Craniofacial abnormalities
Physical exam:
Crowded oropharynx (Mallampati 3-4)
Large tongue/tonsils
Retrognathia
Diagnostic Approach
Sleep study indications:
High pretest probability
Epworth Sleepiness Scale >10
Witnessed apneas with daytime symptoms
CPAP trial indications:
Obvious clinical OSA in high-risk patient
Can start without sleep study if classic presentation
The key decision point: if the patient has obvious OSA (obese man with loud snoring and daytime sleepiness), you can start CPAP without a sleep study. If the presentation is atypical, order polysomnography first.
Respiratory Failure: Type 1 vs Type 2 and ABG Interpretation
Respiratory failure questions test ABG interpretation and ventilation decisions. Know the cutoffs and when to intubate.
Type 1 vs Type 2 Respiratory Failure
Type 1 (hypoxemic):
PaO2 <60 on room air
Normal or low CO2
Causes: pneumonia, PE, ARDS
Treatment: supplemental oxygen
Type 2 (hypercapnic):
PaCO2 >50 with acidosis
Often with hypoxemia
Causes: COPD, neuromuscular disease
Treatment: ventilation support
ABG Interpretation Steps
1. pH: Acidic (<7.35) or alkalotic (>7.45)
2. Primary disorder: Respiratory (CO2) or metabolic (HCO3)
3. Compensation: Appropriate or not
4. Oxygenation: PaO2 and A-a gradient
Normal values:
pH: 7.35-7.45
PaCO2: 35-45 mmHg
HCO3: 22-26 mEq/L
PaO2: 80-100 mmHg
Intubation Indications
Absolute:
Respiratory arrest
Severe hypoxemia despite maximum oxygen
Severe acidosis (pH <7.25)
Altered mental status with inability to protect airway
Relative:
Progressive fatigue
Worsening hypercapnia
Work of breathing
Step 2 CK will present ABG values and ask about next steps. If pH is 7.20 with CO2 of 80 in a COPD patient, think about non-invasive ventilation first. If they dont improve in 1-2 hours, intubate.
Vignette Approach: How Step 2 CK Frames Pulmonology Cases
After doing 2000+ Step 2 CK questions, the patterns become obvious. Every pulmonology vignette follows predictable structures.
Common Stem Patterns
Pattern 1: Chief complaint + risk factors + physical exam
"A 45-year-old man with a 30 pack-year smoking history presents with progressive dyspnea..."
Pattern 2: Hospital course + complication
"A 70-year-old woman is hospitalized for pneumonia. On day 4 of treatment, she develops..."
Pattern 3: Diagnostic workup + results
"A 35-year-old woman presents with chest pain. Chest X-ray shows... CT angiogram reveals..."
Question Types You'll See
Management questions (40%):
"What is the most appropriate next step?"
"What is the best initial treatment?"
Diagnostic questions (35%):
"What is the most likely diagnosis?"
"What test would confirm the diagnosis?"
Prognostic/counseling questions (25%):
"What should you tell the patient?"
"What is the most likely outcome?"
Reading the Vignette Strategically
Look for key words:
Age + smoking = think COPD/lung cancer
Recent surgery/travel = think PE
Fever + cough = think pneumonia
Progressive dyspnea = think ILD
Use the timeline:
Acute onset (hours): PE, pneumothorax
Subacute (days-weeks): pneumonia, heart failure
Chronic (months-years): COPD, ILD
Pay attention to numbers:
Specific lab values usually matter
Normal values rule out diseases
Extreme values suggest specific diagnoses
When practicing with adaptive question banks, Oncourse analyzes your weak patterns and serves more questions targeting those gaps. If you keep missing PE workup questions, the engine will focus on Wells score and imaging decisions until you master the approach.
Common Pitfalls and How to Avoid Them
These are the mistakes I see students make repeatedly, even after months of preparation.
Mistake 1: Confusing COPD and Asthma Management
The error: Using SABA alone for COPD exacerbation The fix: COPD always needs SABA + LAMA (albuterol + ipratropium). The obstruction is fixed, not just inflammatory.
Mistake 2: Missing PE Workup Steps
The error: Ordering CT-PA for everyone with chest pain The fix: Calculate Wells score first. If ≤4, check D-dimer. If >4 or D-dimer positive, then CT-PA.
Mistake 3: Misreading ABGs
The error: Focusing only on pH and missing compensation The fix: Use the systematic approach. pH → primary disorder → compensation → oxygenation. Every step matters.
Mistake 4: Wrong Pneumonia Antibiotic Choice
The error: Using the same regimen for all pneumonia The fix: Setting determines therapy. Outpatient healthy = amoxicillin. ICU = dual coverage. HAP/VAP = anti-pseudomonal.
Mistake 5: Overcomplicating Pleural Effusion
The error: Ordering multiple tests before thoracentesis The fix: Large effusion = tap it. Use Light's criteria to guide further workup. pH <7.30 = needs drainage.
Frequently Asked Questions
How much time should I spend on pulmonology during Step 2 CK prep?
Dedicate 8-10% of your study time to pulmonology since it represents 8-12% of the exam. For a 6-week dedicated period, thats about 4-5 days of focused pulmonology review. Start with high-yield topics (COPD/asthma, pneumonia, PE) then move to lower-yield areas.
What's the best way to memorize Wells criteria and Light's criteria?
Use spaced repetition for exact numbers. Practice calculating scores with real vignettes until its automatic. The criteria are objective — no clinical judgment involved. Most students find mnemonics helpful: "DVT-3, PE likely-3, HR>100-1.5" for Wells.
How do I approach complex cases with multiple possible diagnoses?
Start with the most common causes and work systematically. A 60-year-old smoker with dyspnea could have COPD, heart failure, or lung cancer. Look for specific clues: smoking history + fixed obstruction = COPD. JVD + bilateral edema = heart failure. Weight loss + hemoptysis = cancer.
Should I memorize every antibiotic regimen for pneumonia?
Focus on the decision framework rather than every possible drug combination. Know the first-line choices for each setting: amoxicillin for outpatient healthy, ceftriaxone + macrolide for inpatient non-ICU. The principles matter more than memorizing 15 different regimens.
How detailed should my knowledge be for interstitial lung diseases?
Know the classic presentation patterns and key distinguishing features. You wont need to interpret HRCT images, but you should recognize clinical descriptions: IPF = older male smoker with lower lobe honeycombing. Sarcoidosis = young African American woman with bilateral hilar adenopathy.
What's the most common mistake students make on pulmonology questions?
Overthinking the clinical decision-making. Step 2 CK tests algorithms, not complex medical reasoning. If the Wells score is >4, order CT-PA. If the pleural fluid pH is <7.30, drain it. Trust the criteria and follow the pathways.
---
Pulmonology success on Step 2 CK comes from pattern recognition and systematic thinking. Master the key clinical criteria, practice the decision algorithms until they're automatic, and focus your energy on the high-yield topics that appear most frequently. The exam rewards students who can quickly identify the correct pathway and follow it to the right answer.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.