Back
USMLE Step 1 Is Pass/Fail Now — Here's What IMGs Actually Need to Do to Match in 2026
Step 1 pass/fail changed everything for IMGs. Here's the real impact on residency matching and what international medical graduates need to do differently in 2026.

USMLE Step 1 Is Pass/Fail Now — Here's What IMGs Actually Need to Do to Match in 2026
You probably opened this article because you heard that Step 1 scores dont matter anymore and wondered if that makes matching easier for IMGs. The short answer: it doesnt.
The reality hits differently when you look at the numbers. In 2024, IMG match rates dropped to 58.7% — the lowest in over a decade. Step 1 going pass/fail didnt level the playing field. It just moved the competition elsewhere, and residency programs adapted faster than most IMGs realized.
Here's what actually changed and what you need to do about it in 2026.
The Real Impact of Step 1 Pass/Fail for IMGs
When Step 1 became pass/fail in January 2022, many IMGs thought high Step 1 scores were their biggest differentiator. That was partly true — a 260+ Step 1 could compensate for other application weaknesses. But removing numerical scores didnt eliminate the fundamental challenges IMGs face.
What got harder:
Step 2 CK became the primary screening tool. Programs now filter by Step 2 scores more aggressively
Clinical experience requirements became stricter. US clinical experience (USCE) is now virtually mandatory for competitive specialties
Research expectations increased. IMGs need more publications and meaningful research involvement
Away rotations became more critical for networking and proving clinical competence
What stayed the same:
Visa sponsorship remains a major barrier. Only 40% of residency programs sponsor J1/H1B visas
Geographic limitations persist. IMGs still cluster in specific regions and hospital systems
Timeline pressure hasnt changed. You still need everything ready 18 months before starting residency
The pass/fail change essentially removed one pathway to differentiation without creating alternatives. Step 2 CK scores now carry the entire burden that Step 1 and Step 2 used to share.
Step 2 CK: Your New Make-or-Break Exam
With Step 1 scores gone, Step 2 CK became the numerical gatekeeper. Programs use Step 2 scores for initial screening, interview invitations, and rank lists. The target scores shifted upward because theres only one exam to evaluate knowledge.
Current Step 2 CK score targets for IMGs:
Competitive specialties (Dermatology, Radiation Oncology, Orthopedics): 270+
Moderately competitive (Internal Medicine at academic centers, Emergency Medicine): 250-260
Less competitive (Family Medicine, Psychiatry, Pathology): 240-250
Safety programs (Internal Medicine at community hospitals): 230+
These targets are 10-15 points higher than pre-pass/fail requirements because programs know they cant rely on Step 1 for differentiation anymore.
Step 2 CK timing strategy:
Take Step 2 CK by June of your application year (for Match in March of the following year). This gives you time for one retake if needed while still meeting application deadlines. Most IMGs who take Step 2 in August or later dont have time to improve their score if they underperform.
When preparing for Step 2 CK, use targeted question practice to identify weak areas early. The clinical vignettes are longer and more detailed than Step 1, requiring different preparation strategies.
Clinical Experience: The Non-Negotiable Requirement
US clinical experience (USCE) went from "strongly recommended" to practically mandatory. Programs want proof that you can function in the US healthcare system, communicate with patients and colleagues, and understand American clinical workflows.
Minimum USCE requirements by specialty:
Competitive specialties: 6+ months, including away rotations
Moderately competitive: 4-6 months with at least 2 months in your target specialty
Less competitive: 3-4 months with some exposure to your specialty
Types of USCE that matter: 1. Away rotations — Gold standard. You work directly with faculty who might interview or rank you 2. Observerships — Better than nothing, but limited impact. Youre watching, not doing 3. Research electives — Good for building relationships and publications simultaneously 4. Externships — Hands-on experience at international medical graduate-friendly programs
The key insight: USCE quality matters more than quantity. One month at a program where you connect with faculty beats three months of generic observerships. Programs want to see that attending physicians trust your clinical judgment and would work with you again.
For clinical reasoning practice that mirrors real patient encounters, try Probe Game — it simulates the diagnostic thinking process youll need during rotations.
Research and Publications: Building Academic Currency
With Step 1 scores gone, research became another primary differentiator. IMGs need publications to prove they can contribute to academic medicine, not just consume it.
Research targets by specialty:
Academic Internal Medicine: 5+ publications including 2-3 first-author papers
Emergency Medicine: 3-5 publications with at least 1 first-author
Family Medicine: 2-3 publications, case reports acceptable
Competitive specialties: 10+ publications with significant first-author contributions
Research strategy for IMGs:
Start research 24-36 months before applying. This timeline allows for manuscript writing, peer review, and publication delays. Focus on projects where you can be first author rather than contributing to many projects as a middle author.
Case reports offer the fastest path to publication for IMGs. Look for interesting cases during clinical rotations and write them up with supervising attendings. Most journals publish case reports within 6-12 months if they meet quality standards.
Systematic reviews work well for IMGs because they dont require access to specific patient populations or expensive lab equipment. Choose narrow topics with clear clinical relevance to your target specialty.
Application Strategy: Playing the Numbers Game Smarter
IMG applications require a fundamentally different strategy than US medical graduates. You need more applications, earlier submissions, and broader geographic flexibility.
Application numbers by competitiveness:
Highly competitive specialties: 80-120 applications
Moderately competitive: 60-80 applications
Less competitive: 40-60 applications
These numbers reflect the visa sponsorship bottleneck. Even qualified IMGs get filtered out because programs dont sponsor visas, not because of competency concerns.
Geographic strategy:
Target states with high IMG populations: New York, New Jersey, Michigan, Illinois, Texas, and Florida. These areas have more IMG-friendly programs and established support systems. California has many programs but extremely competitive match rates for IMGs.
Apply broadly within your score range rather than reaching for programs significantly above your qualifications. A family medicine position at a community hospital beats not matching at all.
Personal statement focus:
Your personal statement needs to address the "why America" question directly. Programs want to know why you chose US residency training over opportunities in your home country. Be specific about clinical experiences that influenced this decision rather than generic statements about advanced medical education.
Timeline: When to Do What for 2026 Match
The application timeline didnt change with Step 1 pass/fail, but the pressure points shifted. You need earlier clinical exposure and Step 2 preparation because theres less room for error.
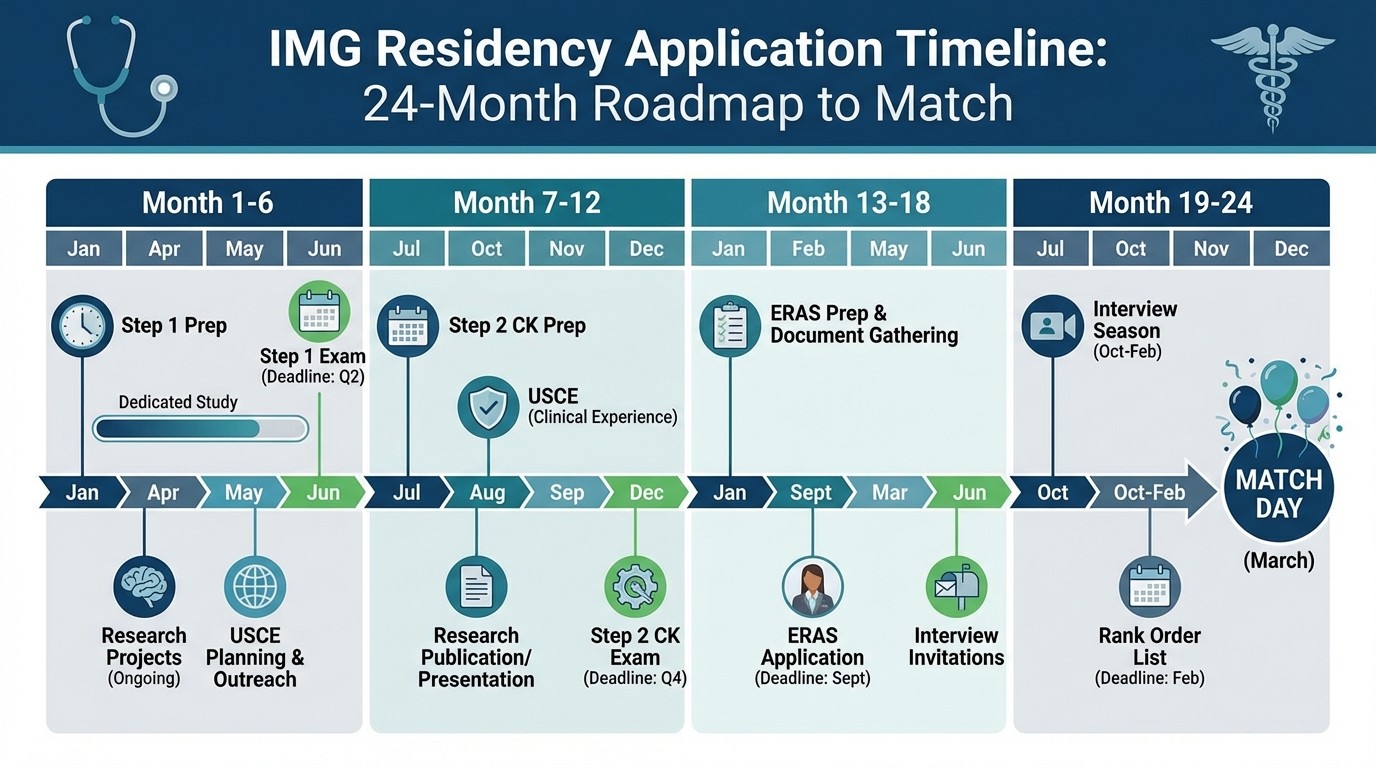
24 months before Match (March 2024 for March 2026 Match):
Pass Step 1 (aim for first attempt)
Begin USCE planning and applications
Start research projects
Take TOEFL if needed
18 months before Match (September 2024):
Complete first USCE rotations
Begin Step 2 CK preparation
Submit research abstracts to conferences
Network with attendings from rotations
12 months before Match (March 2025):
Take Step 2 CK by June 2025 at latest
Complete additional USCE rotations
Submit first-author publications
Begin ERAS application preparation
6 months before Match (September 2025):
Submit ERAS applications by September 15
Complete interviews October-January
Submit rank lists by February
This timeline assumes no exam failures or major setbacks. Build 2-3 months of buffer time for potential delays.
Step 3: The New Differentiator
Some IMGs now take Step 3 before residency to differentiate their applications. This wasnt common pre-pass/fail because Step 1 scores provided differentiation. Now, passing Step 3 shows youre serious about US practice and have advanced clinical knowledge.
Step 3 timing considerations:
Take after Step 2 CK and clinical rotations for best preparation
Complete by December of application year so scores appear in your file
Only attempt if confident you'll pass — failures hurt more than not taking the exam
Step 3 works best for IMGs with marginal Step 2 scores or limited clinical experience. If you have strong Step 2 scores (260+) and good USCE, Step 3 provides minimal additional benefit.
For comprehensive Step 3 preparation, review clinical decision-making scenarios that mirror the exam's clinical case simulations.
Letters of Recommendation: Quality Over Quantity
With fewer objective metrics, letters of recommendation carry more weight. Programs rely on letters to understand your clinical performance and work ethic since numerical Step 1 scores are unavailable.
Letter sources by priority:
1. US attending physicians from clinical rotations (minimum 2)
2. Department chairs or program directors who know your work
3. Research supervisors from significant projects
4. International faculty only if they trained in US or have US connections
Letter content that matters:
Letters should include specific examples of your clinical reasoning, patient interaction skills, and work ethic. Generic letters about being "hardworking and dedicated" dont differentiate you from thousands of other IMGs.
Ask for letters at the end of successful rotations while your performance is fresh in attendings' minds. Provide them with your CV, personal statement, and specific examples of cases you worked on together.
Networking and Away Rotations: Your Interview Insurance
Away rotations became the primary networking opportunity for IMGs. These rotations allow programs to evaluate you directly rather than relying solely on application materials.
Away rotation strategy:
Apply to 8-12 programs for away rotations in your target specialty. This seems like overkill, but acceptance rates for IMGs are low. Submit applications as early as possible — many programs fill away rotation spots by May for the following academic year.
During away rotations, focus on building relationships rather than showing off medical knowledge. Programs know you have the knowledge (you passed Step 1 and Step 2). They want to see if youll integrate well with their team and patient population.
Networking beyond away rotations:
Attend national specialty conferences and local medical society meetings
Join IMG-specific organizations in your specialty
Connect with current residents and recent graduates from your target programs
Use LinkedIn to build professional relationships with faculty
Remember that networking is about building genuine professional relationships, not just asking for favors. Contribute to research projects, volunteer for committees, and offer value before requesting help.
Using spaced repetition tools like flashcards helps you retain the detailed clinical knowledge youll need during rotations and networking conversations.
Interview Performance: Making Every Opportunity Count
IMG interview rates dropped significantly after Step 1 became pass/fail. Programs invite fewer IMGs for interviews because they have fewer objective measures to evaluate candidates. This makes interview performance more critical than ever.
Common IMG interview questions:
"Why did you choose medicine and why in the United States?"
"How has your international background prepared you for US residency?"
"What challenges do you anticipate as an IMG, and how will you address them?"
"Tell us about a difficult patient interaction and how you handled it."
"How do you handle working with team members who may question your abilities?"
Interview preparation strategy:
Practice interviews with current residents and faculty, not just other medical students. Your answers need to sound natural and confident, not rehearsed. Record yourself answering questions and identify verbal tics or nervous habits.
Research each program thoroughly. Know their patient population, research interests, and recent achievements. Ask thoughtful questions about the program rather than generic inquiries about call schedules.
Virtual interview considerations:
Most interviews remain virtual or hybrid in 2026. Test your technology setup multiple times and have backup plans for internet or equipment failures. Use good lighting and a professional background — these details matter more in virtual formats.
Financial Planning: The Hidden Challenge
IMG residency applications cost significantly more than most students anticipate. Budget for these expenses early to avoid last-minute stress.
Typical IMG application costs:
USMLE exams: $4,500-6,000 (including potential retakes)
USCE programs: $3,000-8,000 per month
ERAS application: $350 base + $42 per program (60+ programs = $2,870)
Interview travel: $2,000-5,000 (even with virtual interviews)
Total: $15,000-25,000
These numbers dont include living expenses during USCE rotations or lost income from not working during preparation periods.
Funding strategies:
Apply for international student scholarships and grants
Consider educational loans designed for international medical graduates
Work part-time in research or clinical roles that enhance your application
Budget over 24-36 months rather than trying to fund everything in the application year
Backup Plans: What If You Dont Match
Despite perfect preparation, some qualified IMGs dont match due to factors beyond their control. Having backup plans reduces stress and provides alternative pathways to US residency.
Backup options: 1. SOAP — Participate in the Supplemental Offer and Acceptance Program for unfilled positions 2. Research year — Work as a research fellow while strengthening your application for next year 3. Preliminary positions — Accept transitional year or preliminary positions to get US residency experience 4. International opportunities — Consider residency programs in Canada, Australia, or your home country Strengthening your application for reapplication:
Improve Step 2 CK scores if they were marginal
Gain additional USCE and research experience
Expand geographic and specialty flexibility
Get additional letters from US physicians
Most IMGs who dont match on first attempt succeed on their second try if they address application weaknesses systematically.
Success Stories: What Actually Works
The IMGs who successfully matched after Step 1 became pass/fail share common strategies:
Successful IMG profile example:
Step 1: Pass (first attempt)
Step 2 CK: 255
USCE: 6 months including 2 away rotations
Research: 4 publications (2 first-author)
Applied to: 75 programs in Internal Medicine
Interviews: 12
Matched: Academic Internal Medicine program in New York
Key success factors:
1. Early planning (started USCE applications 18 months before Match)
2. Geographic flexibility (applied to programs in 15 states)
3. Strong Step 2 CK performance on first attempt
4. Meaningful research with US faculty
5. Excellent letters from away rotation attendings
The pattern is clear: successful IMGs compensated for the loss of Step 1 differentiation by excelling in multiple areas rather than relying on one strong component.
For comprehensive exam preparation that mirrors successful candidates' study methods, try Rezzy AI tutoring for personalized learning adapted to your specific knowledge gaps.
Specialty-Specific Considerations
Different specialties adapted differently to Step 1 pass/fail changes. Understanding your target specialty's specific requirements helps focus your preparation efforts.
Internal Medicine:
Most IMG-friendly specialty
Strong Step 2 CK scores (250+) essential for academic programs
Research expectations increased but remain manageable (3-5 publications)
USCE highly valued, especially in subspecialty areas
Family Medicine:
Continues to welcome IMGs
Lower score thresholds but still need solid Step 2 CK performance (240+)
Community involvement and underserved population experience valued
Less research required but case reports helpful
Emergency Medicine:
Becoming more competitive for IMGs
High Step 2 CK scores needed (255+)
EM rotations and away rotations critical
Research in emergency medicine specifically preferred
Psychiatry:
Moderate competitiveness for IMGs
Step 2 CK scores around 245+ competitive
Clinical experience in psychiatry settings important
Research in mental health topics preferred
Radiology/Pathology:
Research-heavy specialties
Fewer positions but more predictable match rates
Strong academic preparation required
Less emphasis on clinical rotations, more on research productivity
Technology and Preparation Tools
Modern USMLE preparation requires sophisticated study tools that adapt to the current exam format and scoring changes. The key is using platforms that understand both the content and the strategic implications of pass/fail scoring.
Active recall and spaced repetition work better than passive reading for Step 2 CK preparation. The clinical vignettes require pattern recognition that develops through repeated exposure to varied question stems and answer explanations.
When reviewing difficult concepts, using mnemonics and memory aids helps retain complex information during high-stress clinical rotations and exam situations.
Frequently Asked Questions
Is Step 1 easier to pass now that its pass/fail?
No, the passing standard didnt change. You need the same knowledge level to pass Step 1 in 2026 as you did when it was scored. The difference is that programs cant see how far above the passing standard you scored.
Should IMGs take Step 3 before residency?
Only if you have marginal Step 2 CK scores or limited clinical experience. Step 3 provides minimal benefit if you already have strong application components. Focus on Step 2 CK excellence first.
How many programs should IMGs apply to?
Apply to 60-80 programs for moderately competitive specialties, 80-120 for highly competitive ones. The visa sponsorship requirement means you need more applications than US graduates to generate the same number of interviews.
Can low Step 1 scores from before pass/fail hurt my application?
If you took Step 1 before January 2022 and received a low score, some programs may still see those scores. However, most programs now focus primarily on Step 2 CK scores and dont weigh old Step 1 scores heavily.
Is USCE really mandatory for IMGs?
Practically, yes. While some programs dont officially require USCE, competitive candidates all have significant US clinical experience. Budget for at least 3-4 months of USCE for any specialty.
What if I fail Step 2 CK?
Retake it as soon as possible after identifying and addressing knowledge gaps. Most programs dont automatically eliminate candidates with one failure if the retake score is strong. Multiple failures significantly hurt your competitiveness.
The path to residency matching as an IMG in 2026 requires more strategic planning than ever before. Step 1 pass/fail didnt make things easier — it just moved the competition to Step 2 CK scores, clinical experience, and research productivity. Success comes from excelling across multiple application components rather than relying on one standout element.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE success. Download free on Android and iOS.