UPSC CMS Medicine: Use Clinical Rounds to Practice High-Yield Medicine Cases
Transform your UPSC CMS medicine prep from passive reading to clinical case practice. Master cardiology, respiratory, gastro, and emergency medicine through realistic patient scenarios and build exam-winning clinical reasoning skills.
UPSC CMS Medicine: Use Clinical Rounds to Practice High-Yield Medicine Cases
You open your UPSC CMS medicine book to page 47 of cardiology. Another list of facts about acute coronary syndromes stares back at you. Heart attack symptoms, ECG changes, troponin levels. You memorize them, close the book, and wonder: Will I recognize this when a 58-year-old presents with chest tightness and sweating?
That gap between knowing facts and applying them clinically is where most CMS aspirants struggle. Paper I throws 96 general medicine questions at you in 120 minutes. You dont just need to know that ST elevation suggests STEMI — you need to work through the differential, order the right tests, and start appropriate management. Fast.
The shift from passive reading to active case practice isnt optional. Its the difference between cramming disconnected facts and building the clinical reasoning patterns that Paper I actually tests.
Why Case-Based Practice Transforms CMS Medicine Prep
Traditional medicine prep treats symptoms, investigations, and management as separate silos. You memorize chest pain causes, then ECG interpretation, then cardiac medications — but never connect them in real time.
UPSC CMS doesnt test isolated facts. It tests clinical thinking through scenario-based MCQs that mirror actual patient presentations. A typical question gives you a clinical vignette (patient demographics, presenting complaint, key history points, examination findings) and asks you to make the next clinical decision.
Consider this CMS-style cardiology scenario:
"A 45-year-old male with diabetes presents with crushing chest pain for 2 hours, accompanied by sweating and nausea. ECG shows ST elevation in leads II, III, and aVF. What is the most appropriate immediate management?"
This question tests three integrated skills:
Pattern recognition: Connecting symptoms + demographics + ECG = inferior STEMI
Clinical prioritization: Understanding that time = myocardium in acute MI
Management protocols: Knowing first-line reperfusion strategies
Reading about each component separately wont prepare you for this integration. Case-based practice does.
High-Yield Medicine Areas for UPSC CMS Paper I
Paper I allocates 96 questions to general medicine — nearly 40% of your total score. Focus your case practice on these areas that repeatedly appear:
Cardiology (15-20 questions)
Acute coronary syndromes: STEMI vs NSTEMI presentations, ECG interpretation, thrombolysis criteria
Heart failure: Clinical classification, diagnostic workup, first-line management
Arrhythmias: Common rhythm disorders, emergency management, when to cardiovert
Hypertensive emergencies: Crisis vs urgency, target organ damage, step-down protocols
Respiratory Medicine (12-15 questions)
Acute respiratory presentations: Pneumonia severity scoring, oxygen therapy, ventilatory support indications
Obstructive disease: COPD exacerbations, asthma management, inhaler techniques
Pleural disorders: Pneumothorax management, pleural effusion workup
Respiratory failure: Type I vs Type II, NIV criteria, intubation indications
Gastroenterology & Hepatology (10-12 questions)
GI bleeding: Upper vs lower, risk stratification, endoscopy timing
Acute abdomen: Appendicitis, cholangitis, pancreatitis — when to operate
Liver disease: Acute hepatitis workup, cirrhosis complications, ascites management
Inflammatory bowel disease: Crohns vs UC presentations, flare management
Emergency Medicine (8-10 questions)
Shock recognition: Hypovolemic, cardiogenic, septic — rapid assessment and initial management
Poisoning protocols: Common toxidromes, antidote use, supportive care
Trauma priorities: ABCDE approach, when to activate protocols
Critical care basics: Ventilator modes, sedation, ICU monitoring
Infectious Diseases & Tropical Medicine (10-12 questions)
Fever workup: Sepsis recognition, blood culture timing, empirical antibiotic choice
Tropical diseases: Malaria types, dengue phases, typhoid complications
Healthcare-associated infections: MRSA, C. diff, antifungal use
Tuberculosis: Extrapulmonary presentations, drug-resistant patterns, contact management
When you practice cases in these areas, you build the pattern recognition that CMS questions demand. Instead of memorizing that "troponin rises in MI," you learn to spot the clinical presentation, order appropriate tests, and initiate evidence-based treatment — all under time pressure.
Moving from Passive Reading to Clinical Case Practice
Most CMS aspirants spend months reading medicine textbooks cover to cover. They know the pathophysiology behind heart failure but freeze when asked to manage acute pulmonary edema in a 72-year-old diabetic.
This happens because reading creates knowledge without application. Case practice creates both.
When you encounter a case scenario, your brain works differently:
1. Active engagement: You must gather information, form hypotheses, test them
2. Pattern building: Similar presentations start linking together into recognizable clusters
3. Decision-making under pressure: You learn to prioritize interventions when multiple options exist
4. Mistake correction: Wrong choices get immediate feedback, preventing repetition
Clinical Rounds transforms this theory into practice by simulating real patient encounters. Instead of reading about chest pain, you take history from a 58-year-old with substernal pressure, examine findings, order ECGs, interpret results, and initiate treatment — just like on hospital rounds.
Each case follows the clinical reasoning process you'll use in practice:
History taking: Focused questions that reveal key diagnostic clues
Physical examination: Relevant findings that narrow your differential
Diagnostic testing: Choosing tests that change management, not just confirm suspicions
Treatment decisions: Evidence-based interventions with proper dosing and monitoring
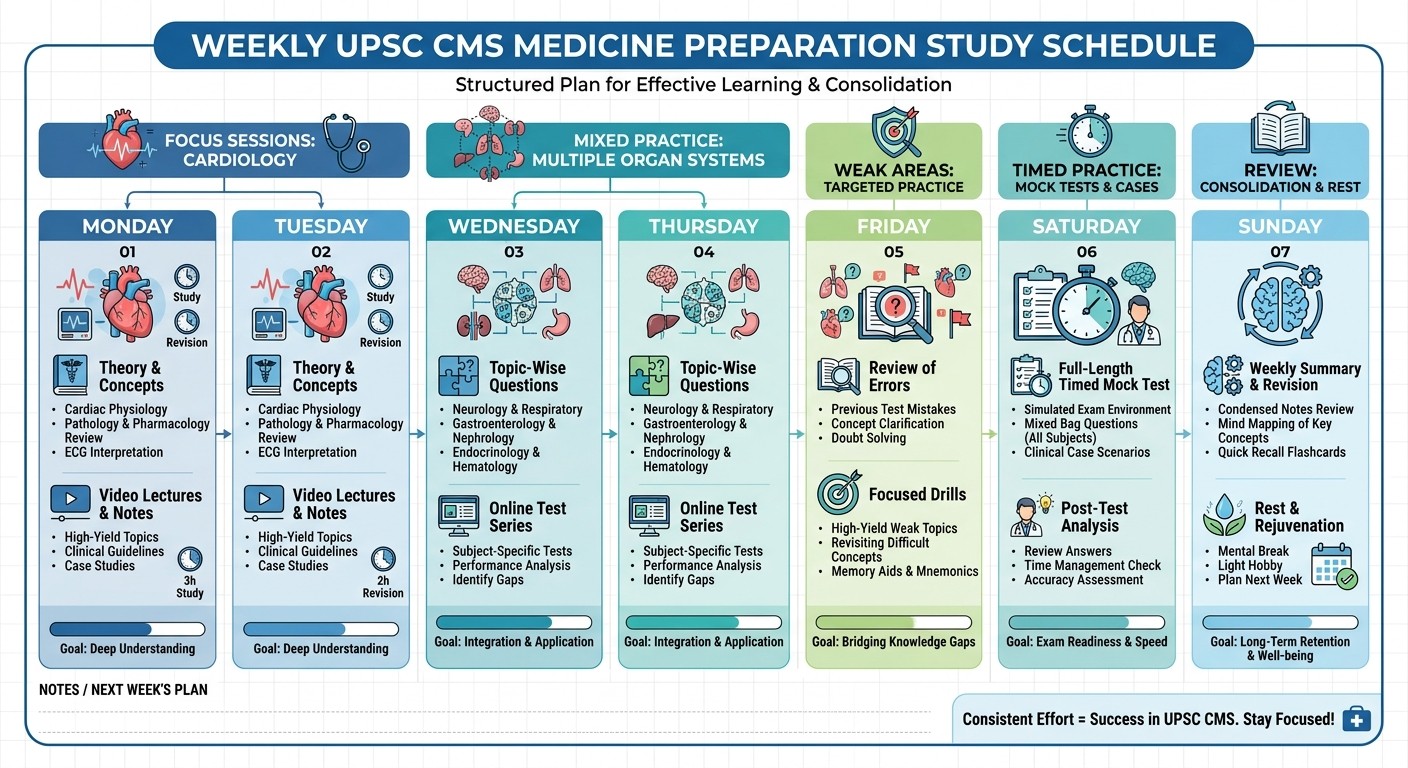
Building Your Weekly Case Practice Loop
Effective case practice needs structure. Random cases without systematic review waste time. Use this proven 4-step cycle:
Monday-Tuesday: Focus Sessions (2-3 cases per system)
Pick one high-yield area (cardiology, respiratory, gastro). Work through 2-3 cases systematically:
Read the presentation carefully
Form your differential before looking at options
Select your answer with reasoning
Review explanations thoroughly, even for correct answers
For cardiology focus, practice acute coronary syndromes, heart failure, and arrhythmia cases. Notice how presenting symptoms vary but diagnostic principles remain consistent.
Wednesday-Thursday: Mixed System Practice (4-5 cases)
Combine cases from different systems to simulate Paper I's mixed question pattern. This builds mental flexibility — switching from respiratory to gastro to emergency medicine thinking.
Practice transitioning between different clinical reasoning patterns. A respiratory case might need oxygen calculation, while the next gastro case requires bleeding risk stratification.
Friday: Weak Area Targeting (3-4 focused cases)
Identify your weakest medicine areas from recent practice. If infectious diseases trips you up, spend Friday exclusively on fever workups, sepsis recognition, and antibiotic selection cases.
Use Rezzy AI to dig deeper into missed concepts. When you get a tropical medicine case wrong, chat with Rezzy about the specific pathophysiology and clinical pearls you missed. This targeted feedback prevents the same mistakes from recurring.
Saturday: Timed Mixed Practice (8-10 cases in 45 minutes)
Simulate Paper I conditions with mixed cases under strict time limits. This builds both speed and accuracy — essential for CMS success.
Track your performance patterns. Are you slow on gastro cases? Missing key findings in respiratory presentations? Struggling with emergency medicine priorities? Use these insights to adjust next week's focus.
Sunday: Review and Consolidation
Review the week's missed cases without looking at your previous answers. Can you get them right now? If not, the concept needs more reinforcement.
Create quick reference cards for high-yield patterns you struggled with. For example: "Chest pain + ST elevation in II, III, aVF = inferior STEMI. Check for RV involvement (V4R). Consider reperfusion within 12 hours."
How to Review Missed Cases Effectively
Missing a case isnt failure — its a learning opportunity. But most students review incorrectly, focusing on the right answer rather than understanding why they went wrong.
Step 1: Identify Your Error Type
Before looking at explanations, categorize your mistake:
Knowledge gap: Didn't know a key fact (e.g., troponin timeline in ACS)
Pattern misrecognition: Misread the clinical presentation
Priority confusion: Knew the diagnosis but chose wrong next step
Time pressure error: Rushed and misread details
Step 2: Deep-dive the Concept
Don't just memorize the correct answer. Understand the underlying principle:
Why was your choice wrong in this clinical context?
What red flags should have pointed toward the correct option?
How does this principle apply to similar presentations?
For example, if you missed a heart failure case by choosing diuretics over ACE inhibitors as first-line therapy, understand both the pathophysiology (neurohormonal activation in HF) and the evidence base (ACE inhibitors reduce mortality, diuretics just treat symptoms).
Step 3: Find Related Cases
One case teaches one pattern. Find 2-3 similar presentations with slight variations. If you missed an acute MI case, practice STEMI vs NSTEMI recognition, different ECG lead patterns, and contraindications to thrombolysis.
Use our comprehensive UPSC CMS cardiology lessons to build broader understanding beyond individual cases.
Step 4: Test Retention
Two days later, work through the same case without looking at your notes. If you get it right with proper reasoning, the concept has consolidated. If not, repeat the deep-dive process.
This spaced repetition approach — combined with our cardiology flashcards — moves knowledge from short-term memorization to long-term clinical reasoning patterns.
Integrating Case Practice with Traditional Study Methods
Case practice doesnt replace textbook reading — it transforms how you use it. Instead of passive absorption, you read with clinical questions in mind.
When reviewing respiratory medicine lessons, ask yourself: "How would this present in a case? What would the examination findings be? What investigations would I order?"
This active reading approach helps you spot high-yield details that commonly appear in CMS cases. For instance, when studying COPD exacerbations, focus on severity markers (pH, CO2 levels) and intervention thresholds (when to start NIV, when to intubate) — these decision points frequently appear in respiratory cases.
Create connections between textbook knowledge and case applications. If you're reading about acute pancreatitis, immediately think: "72-year-old with epigastric pain radiating to back, elevated lipase, CT showing pancreatic inflammation — what's my next management step?"
Practice with our targeted gastroenterology questions to reinforce these connections. Each question tests not just isolated facts but clinical reasoning chains you'll need for Paper I success.
Advanced Case Analysis: Management-First Thinking
CMS questions increasingly test management decisions rather than diagnostic recognition. You might get a case where the diagnosis is obvious, but choosing the right next step separates average scores from top performance.
Management-first thinking means approaching every case by asking: "What does this patient need right now to improve outcomes?"
Consider this emergency medicine scenario:
"A 28-year-old female presents with severe abdominal pain, hypotension, and positive pregnancy test. Ultrasound shows free fluid in pelvis. Next immediate step?"
The diagnosis (ruptured ectopic pregnancy) is clear. But the question tests your management priorities:
Stabilize hemodynamics (IV access, fluids, blood type/crossmatch)
Prepare for emergency surgery
NOT detailed diagnostic workup when patient is unstable
This management-first approach applies across all medicine areas:
Cardiology: STEMI patient needs reperfusion, not detailed echo assessment
Respiratory: Tension pneumothorax needs immediate decompression, not CT chest
Gastro: Severe GI bleeding needs resuscitation and urgent endoscopy, not detailed history
Infectious disease: Septic shock needs empirical antibiotics within the hour, not culture results
Practice cases that specifically test these management decisions. Look for clinical scenarios where time-sensitive interventions take priority over diagnostic perfection.
Using Analytics to Identify Weak Areas
Most CMS aspirants practice randomly without tracking performance patterns. They might be strong in cardiology but consistently struggle with infectious diseases, wasting time on areas they've already mastered while neglecting problem areas.
Smart preparation means data-driven weak area identification:
Track performance by system:
Cardiology: 78% accuracy (strong area)
Respiratory: 65% accuracy (needs work)
Gastroenterology: 71% accuracy (moderate)
Emergency medicine: 58% accuracy (priority focus)
Infectious diseases: 62% accuracy (needs improvement)
Analyze mistake patterns:
Do you consistently miss diagnosis questions but get management right?
Are you strong on common presentations but struggle with rare variants?
Do time-pressured questions trip you up more than untimed practice?
Adjust study allocation accordingly:
Instead of equal time across all systems, spend 40% of your case practice on emergency medicine and infectious diseases, 30% on respiratory and gastro, and just 30% on cardiology maintenance.
This targeted approach maximizes score improvement by focusing effort where it matters most.
The Clinical Reasoning Difference: Beyond Memorization
Traditional CMS prep creates medical students who know facts but cant think clinically. They memorize that "chest pain + ST elevation = STEMI" but dont develop the nuanced reasoning that distinguishes top performers.
Clinical reasoning means understanding the why behind medical decisions:
Pattern recognition: Not just "fever + headache = meningitis" but recognizing subtle presentations, atypical demographics, and red flag combinations that suggest serious pathology. Probabilistic thinking: Understanding that most chest pain isnt cardiac, most headaches arent dangerous — but knowing which clinical features shift those probabilities dramatically. Management prioritization: Recognizing that unstable patients need stabilization before diagnosis, that some interventions cant wait for test results, that clinical judgment sometimes overrules protocol. Error awareness: Understanding common diagnostic pitfalls (anchoring bias, premature closure) and building systematic approaches that reduce mistakes.
When you practice with Clinical Rounds, each case builds these reasoning patterns. Instead of memorizing isolated facts, you develop the clinical thinking patterns that make complex decisions feel intuitive.
For example, after working through multiple acute coronary syndrome cases, you'll automatically consider ACS in atypical presentations (elderly women with epigastric pain, diabetics with silent ischemia) — pattern recognition that textbook reading alone rarely develops.
Frequently Asked Questions
How many cases should I practice daily for CMS medicine?
Start with 5-7 cases daily, focusing on quality over quantity. Spend 8-10 minutes per case including review time. As you build speed and pattern recognition, increase to 10-12 cases per day closer to the exam.
Which medicine topics appear most frequently in Paper I?
Cardiology (15-20 questions), respiratory medicine (12-15), gastroenterology (10-12), and emergency medicine (8-10) consistently show high weightage. Prioritize case practice in these areas while maintaining coverage of other systems.
Should I practice cases from all systems or focus on weak areas?
Use a mixed approach: 60% of practice time on weak areas, 40% maintaining strong areas. Complete system neglect leads to score drops in previously mastered topics.
How do I improve speed without sacrificing accuracy?
Practice timed sessions regularly, starting with generous time limits and gradually reducing. Focus on rapid pattern recognition in the first 30 seconds — most CMS cases can be solved quickly once you identify the key clinical pattern.
What's the difference between case practice and MCQ practice?
Case practice develops clinical reasoning through integrated scenarios. MCQ practice often tests isolated facts. CMS increasingly uses case-based MCQs, making clinical reasoning practice more relevant than pure factual recall.
How long before the exam should I start case-based practice?
Begin case practice as soon as you complete initial medicine reading (typically 3-4 months before CMS). Early case practice helps identify knowledge gaps while you still have time for targeted review.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for UPSC CMS. Download free on Android and iOS.