Back
USMLE Step 1 Biochemistry: How Mnemonics and Probe Game Build Faster Recall
Master USMLE Step 1 biochemistry with proven mnemonics and active recall strategies. Turn pathway memorization into rapid retrieval for exam success.

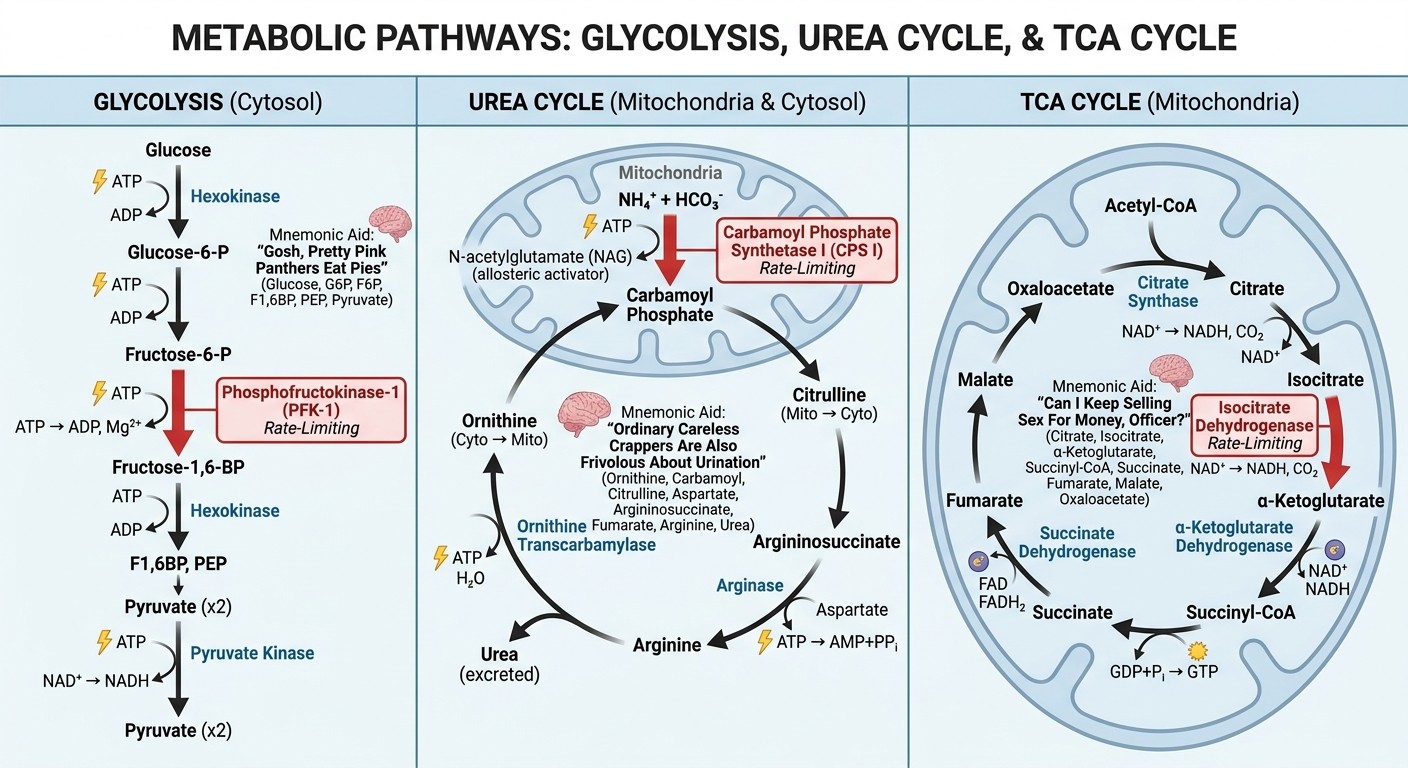
You probably know the feeling. You memorized "Orange Cola Coffee Alcohol of Argentina For Aggressive Urine" for the urea cycle intermediates last month. Today, you see a hyperammonemic infant on a practice question and your mind goes blank. The mnemonic sits there, useless.
USMLE Step 1 has 280 questions. You have 100 seconds each. Biochemistry makes up 15-20% of the exam — roughly 42-56 questions that could make or break your score. The students who ace biochemistry dont just memorize more mnemonics. They turn mnemonics into retrieval loops that fire instantly under pressure.
Here's how to build biochemistry recall that sticks when it counts.
The Mnemonic Problem: Memory Without Retrieval
Most students collect mnemonics like trading cards. "ABCDEF" for fat-soluble vitamins. "PVT TIM HALL" for essential amino acids. "Very Poor Carbohydrate Metabolism" for glycogen storage diseases.
The problem? You need more than passive recognition. Step 1 questions dont ask "what does the mnemonic stand for?" They bury the pathway in a clinical vignette. A 3-month-old with hepatomegaly, lactic acidosis, and hypoglycemia after fasting isnt obviously "Type I glycogen storage disease" until you connect the dots.
The missing piece is retrieval practice. Mnemonics become useful when you practice going backward — from clinical picture to pathway to mechanism. That takes active recall, not passive review.
Active Recall: The Missing Link in Biochemistry Mastery
Active recall means testing yourself without looking at the answer first. Instead of reading "glucose-6-phosphatase deficiency causes Von Gierke disease," you start with "infant with severe fasting hypoglycemia and hepatomegaly" and work backward to the enzyme.
This approach mirrors how Step 1 actually tests biochemistry. Questions start with symptoms, lab values, or metabolic states. You need to trace backward through pathways to find the broken step.
Try this with the urea cycle. Instead of reciting "CPS I is the rate-limiting enzyme," start with a clinical scenario: newborn with lethargy, vomiting, and ammonia level of 400 μmol/L. Work through the differential. Why is ammonia high? Which enzymes could be deficient? How would you distinguish CPS I deficiency (no orotic aciduria) from OTC deficiency (elevated orotic acid)?
When you use Oncourse's Synapses mnemonic tool, the memory cues get embedded into these retrieval chains, making the pathway connections automatic rather than effortful.
Rate-Limiting Enzymes: The High-Yield Targets
Step 1 loves testing rate-limiting enzymes because they control entire pathways. Master these 8 and you unlock most biochemistry questions:
Glycolysis: PFK-1 (Phosphofructokinase-1)
Mnemonic: "AMP and F-2,6-BP Go; ATP and Citrate Stop"
Clinical hook: Think fasting vs fed states. Low energy (high AMP) pushes glycolysis. High energy (high ATP) slams the brakes.
Gluconeogenesis: FBPase-1 (Fructose-1,6-bisphosphatase)
Reciprocal regulation: When PFK-1 is active, FBPase-1 is inhibited and vice versa
Clinical hook: Glucagon activates gluconeogenesis by increasing cAMP
Urea Cycle: CPS I (Carbamoyl Phosphate Synthetase I)
Activator: N-acetylglutamate (NAG)
Clinical hook: CPS I deficiency shows hyperammonemia without orotic aciduria
TCA Cycle: Isocitrate Dehydrogenase
Regulation: Inhibited by ATP and NADH (energy sufficient)
Clinical hook: Links to thiamine deficiency affecting pyruvate entry
Cholesterol Synthesis: HMG-CoA Reductase
Inhibitors: Statins target this enzyme
Clinical hook: Familial hypercholesterolemia questions
Fatty Acid Oxidation: CPT-I (Carnitine Palmitoyltransferase I)
Inhibitor: Malonyl-CoA (fed state)
Clinical hook: MCAD deficiency and fasting hypoglycemia
Heme Synthesis: ALA Synthase
Cofactor: Vitamin B6
Clinical hook: Lead poisoning affects downstream steps
HMP Shunt: G6PD (Glucose-6-Phosphate Dehydrogenase)
Function: Generates NADPH for antioxidant defense
Clinical hook: Hemolytic anemia with oxidative stress
The key insight: these enzymes dont work in isolation. Theyre controlled by hormonal signals (insulin, glucagon, cortisol) and energy status (ATP/ADP ratios, NAD+/NADH). Practice connecting the clinical state to the hormonal signal to the enzyme regulation.
Lysosomal Storage Diseases: Pattern Recognition Made Simple
LSDs follow predictable patterns. Instead of memorizing 15+ individual diseases, learn the organizational framework:
The Accumulation Pattern
Sphingolipidoses: Fatty buildup → neurodegeneration
Mucopolysaccharidoses: Sugar mess → skeletal/organ abnormalities
Glycogen storage: Enzyme + organ system affected
High-Yield Disease Clusters
Cherry-Red Macula Club:
Tay-Sachs: GM2, hexosaminidase A, NO hepatosplenomegaly
Niemann-Pick: sphingomyelin, sphingomyelinase, YES hepatosplenomegaly
Hepatosplenomegaly Group:
Gaucher: "crumpled tissue paper" macrophages
Pompe: cardiomegaly dominates
Corneal Clouding Distinction:
Hurler: YES corneal clouding
Hunter: NO corneal clouding ("Hunters see clearly")
The pattern works like this: see the clinical picture → identify the accumulating substrate → match to the deficient enzyme. Most questions give you enough clues to narrow down the category, then you differentiate within that group.
Vitamin Deficiencies: Clinical Scenarios to Pathways
Step 1 vitamin questions follow templates. Learn the clinical pattern for each vitamin, then connect to the biochemical mechanism:
Thiamine (B1): The Energy Crisis Vitamin
Clinical pattern: Alcoholic with confusion + ataxia + eye movement problems
Biochemical hook: TPP cofactor for pyruvate dehydrogenase
Key insight: Never give glucose before thiamine in alcoholics
Niacin (B3): The 4 D's
Clinical pattern: Dermatitis, diarrhea, dementia, death
Biochemical hook: NAD+/NADP+ dependent enzymes
High-yield connection: Hartnup disease, carcinoid syndrome, isoniazid therapy
Folate vs B12: The Megaloblastic Distinction
Folate: No neurologic symptoms
B12: Neurologic symptoms (subacute combined degeneration)
Biochemical hook: Methylmalonyl-CoA pathway (B12 specific)
When practicing on Oncourse's Step 1 biochemistry lessons, focus on the clinical vignette → pathway connection rather than isolated vitamin facts.
The Probe Game Strategy: Rapid Weak-Area Detection
Heres where most students fail: they review what they already know instead of finding what they dont. The Probe Game approach flips this. You use rapid-fire questions to identify weak pathways, then drill those specific areas.
The 3-Second Rule
If you cant identify the pathway and rate-limiting enzyme within 3 seconds of reading a biochemistry question stem, thats a weak area. Mark it for focused review.
The Mistake Analysis Loop
1. Identify the miss: What pathway did you confuse? 2. Find the trigger: Which clinical detail should have pointed to the correct pathway? 3. Create the connection: Build a memory link between that clinical detail and the pathway 4. Test the connection: Use spaced repetition to verify the link sticks
For example, if you miss that "musty body odor in an intellectually disabled child" points to phenylketonuria, create this connection: musty odor → phenylalanine buildup → phenylalanine hydroxylase deficiency → PKU. Then test this connection repeatedly until its automatic.
Using Oncourse's Probe Game specifically for weak biochemistry topics helps you find these gaps quickly without wasting time on concepts you already know.
Building Retrieval Chains: From Symptoms to Enzymes
The strongest Step 1 performers dont just know pathways — they build retrieval chains that connect clinical presentations to mechanisms. Here's how to build them:
Chain Structure: Symptom → Substrate → Enzyme → Pathway
Take glycogen storage disease Type V (McArdle):
Symptom: Exercise intolerance in a teenager
Substrate: Muscle glycogen cant break down
Enzyme: Muscle phosphorylase deficiency
Pathway: Glycogen metabolism
Key detail: "Second wind" phenomenon
Practice Retrieval Forward and Backward
Forward: Start with enzyme deficiency → predict clinical picture
Backward: Start with clinical picture → identify enzyme deficiency
Use Clinical Anchors
Each pathway needs a memorable clinical anchor:
Urea cycle: Newborn with vomiting and lethargy
Glycolysis: Hemolytic anemia with oxidative stress (G6PD)
TCA cycle: Lactic acidosis with thiamine deficiency
Fatty acid oxidation: Hypoglycemia after prolonged fasting
The anchors give you a starting point when you see similar presentations on the exam.
Weak-Area Review: The Adaptive Approach
Most students review biochemistry in the same order every time. The adaptive approach focuses your time where it matters most.
The 70/20/10 Rule
70% of time: Pathways you miss frequently
20% of time: Pathways you sometimes miss
10% of time: Pathways you consistently get right
Weekly Pathway Audit
Every week, track which pathway categories cause the most mistakes:
Carbohydrate metabolism
Lipid metabolism
Amino acid metabolism
Nucleic acid metabolism
Vitamin biochemistry
Focus the following week's study on your weakest category.
Mistake Pattern Analysis
Look for patterns in your biochemistry mistakes:
Missing rate-limiting enzymes?
Confusing similar diseases?
Forgetting cofactor requirements?
Mixing up clinical presentations?
Each pattern suggests a different review strategy.
Putting It All Together: Your 4-Week Biochemistry Plan
Week 1: Foundation Building
Master the 8 rate-limiting enzymes with their mnemonics
Build retrieval chains for high-yield pathways
Complete 50 biochemistry questions in tutor mode
Week 2: Disease Pattern Recognition
Focus on lysosomal storage diseases and glycogen storage diseases
Learn vitamin deficiency clinical patterns
Practice biochemistry questions with immediate review
Week 3: Weak-Area Targeting
Use Probe Game strategy to identify knowledge gaps
Focus 70% of time on consistently missed topics
Create new mnemonics for problem areas
Week 4: Integration and Speed
Practice biochemistry questions under timed conditions
Focus on connecting pathways to clinical vignettes
Final review of rate-limiting enzymes and disease patterns
Advanced Integration: Connecting Biochemistry to Clinical Medicine
The highest-scoring students dont see biochemistry as isolated pathways. They connect metabolic concepts to clinical medicine:
Diabetes and Glucose Homeostasis
Connect gluconeogenesis regulation to diabetic ketoacidosis. When insulin is deficient, glucagon dominates → activates gluconeogenesis → worsens hyperglycemia.
Heart Failure and Energy Metabolism
Connect fatty acid oxidation to heart failure. The failing heart shifts from fatty acid metabolism back to glucose metabolism for efficiency.
Liver Disease and Detoxification
Connect urea cycle to hepatic encephalopathy. When the liver cant convert ammonia to urea, ammonia crosses the blood-brain barrier → altered mental status.
These connections help you see the clinical relevance of biochemical pathways, making them more memorable and useful for Step 2 CK preparation.
Common Pitfalls and How to Avoid Them
Pitfall 1: Mnemonic Overload
Problem: Collecting mnemonics without practicing retrieval Solution: For every mnemonic you learn, practice 5 retrieval scenarios
Pitfall 2: Isolated Pathway Study
Problem: Learning pathways without connecting to clinical presentations Solution: Always pair pathway study with clinical vignette practice
Pitfall 3: Passive Review
Problem: Re-reading notes instead of active recall Solution: Use question-based review and self-testing
Pitfall 4: Equal Time Distribution
Problem: Spending equal time on strong and weak areas Solution: Use mistake analysis to guide time allocation
Frequently Asked Questions
How many biochemistry questions should I expect on Step 1?
Step 1 includes 42-56 biochemistry questions (15-20% of 280 total questions). Focus on high-yield topics like metabolic pathways, vitamin deficiencies, and genetic disorders.
Which biochemistry topics are highest yield for Step 1?
Rate-limiting enzymes, vitamin deficiencies (especially B vitamins), glycogen storage diseases, lysosomal storage diseases, and urea cycle disorders appear most frequently.
How long should I spend memorizing biochemistry mnemonics?
Spend 20% of your time learning mnemonics and 80% practicing retrieval. A mnemonic is only useful if you can apply it to clinical scenarios quickly.
Should I use First Aid or other resources for biochemistry?
First Aid provides the framework, but supplement with question banks and active recall tools. The key is connecting biochemical concepts to clinical presentations.
How do I remember all the enzyme deficiencies and their presentations?
Group diseases by patterns (substrate accumulation, organ systems affected) rather than memorizing individual diseases. Focus on distinguishing features within each group.
What's the best way to review biochemistry mistakes?
Create retrieval chains: clinical presentation → pathway → enzyme → mechanism. Practice both forward (enzyme → symptoms) and backward (symptoms → enzyme) retrieval.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 1. Download free on Android and iOS.