Back
How to Prepare Neurology for UKMLA: High-Yield Topics and Clinical Reasoning Traps
Master UKMLA neurology preparation with clinical reasoning approaches, high-yield topics including stroke, seizures, and headaches, plus proven study strategies for 2026 success.
How to Prepare Neurology for UKMLA: High-Yield Topics and Clinical Reasoning Traps
You are probably staring at yet another neurology question that makes perfect sense until you reach the options. The patient clearly has a stroke, but the question asks about thrombolysis criteria. You know the anatomy inside out, but UKMLA doesnt care if you can draw the Circle of Willis. It wants to know: what happens next in the emergency department?
UKMLA neurology is consistently the hardest section because it tests clinical decision-making, not anatomical recall. While cardiology gives you clear ECG patterns and respiratory shows obvious X-ray findings, neurology hides behind longer reasoning chains and nuanced management steps.
Heres how to master the clinical reasoning that UKMLA actually tests.
Why UKMLA Neurology Is Different
Traditional neurology teaching starts with anatomy. Upper motor neuron versus lower motor neuron. Cranial nerve pathways. Spinal tract locations. UKMLA flips this approach completely.
UKMLA neurology questions rarely ask "what is the diagnosis?" Instead, they present a 47-year-old with sudden onset left-sided weakness and ask: "What is the most appropriate immediate investigation?" or "Which management option should be initiated first?"
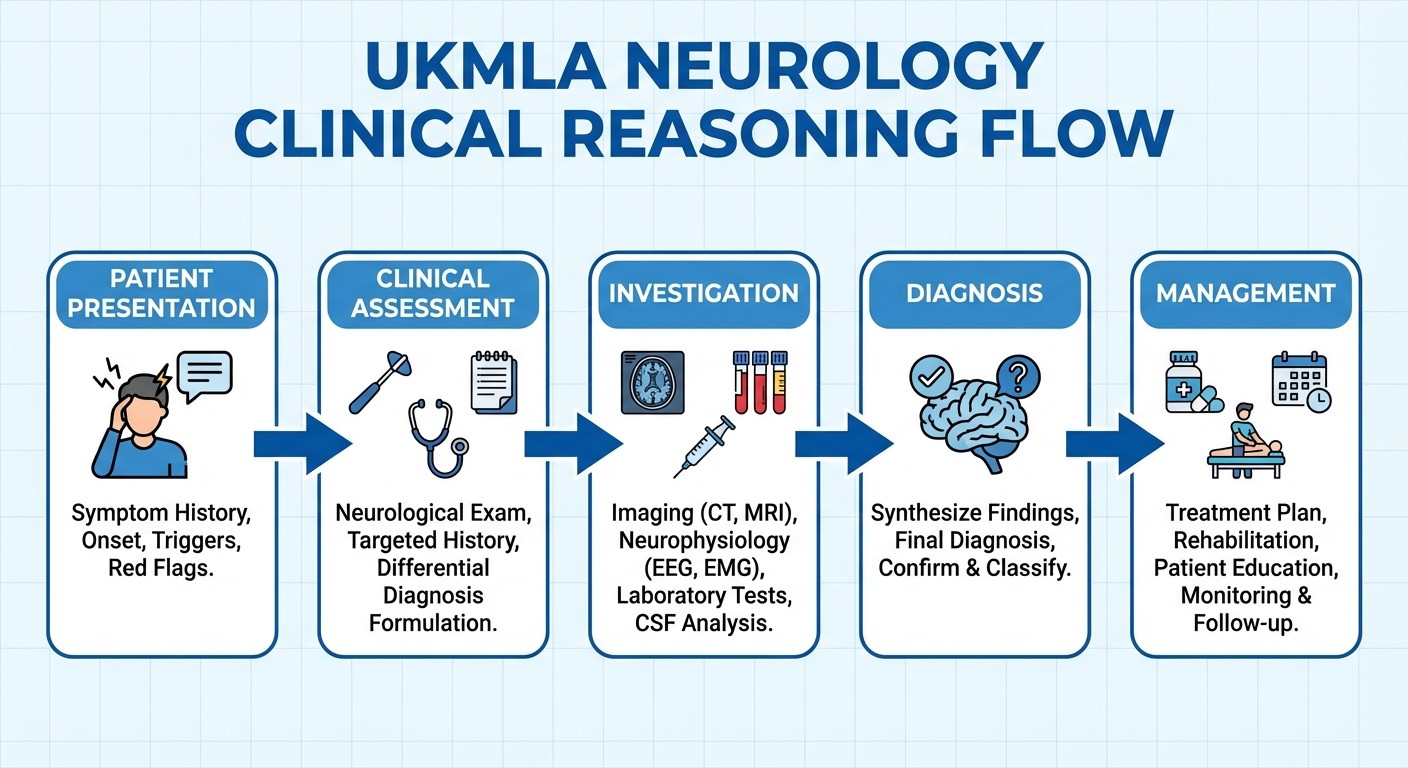
The clinical reasoning chain becomes: presentation → assessment → investigation → diagnosis → management. Each step requires specific knowledge that textbook anatomy doesnt cover. You need to know NIHSS scoring, CT versus MRI timing, thrombolysis contraindications, and NICE pathway decision points.
Most students learn neurology backwards. They memorize lesion locations, then struggle when UKMLA presents real clinical scenarios requiring immediate decisions.
High-Yield UKMLA Neurology Topics
Stroke Management
Ischaemic vs Haemorrhagic Decision Trees
CT head timing: immediate for suspected haemorrhage
Thrombolysis window: 4.5 hours from symptom onset
Contraindications: recent surgery, anticoagulation, severe hypertension
NIHSS scoring for treatment eligibility
TIA Pathway
ABCD2 scoring for risk stratification
48-hour admission criteria
Dual antiplatelet therapy timing
Carotid imaging requirements
Seizure Management
First-Line AED Selection
Focal seizures: levetiracetam or lamotrigine
Generalised tonic-clonic: sodium valproate or lamotrigine
Absence seizures: ethosuximide or sodium valproate
Status epilepticus protocol: lorazepam → phenytoin → general anaesthesia
Clinical Considerations
Driving restrictions: 12 months seizure-free for Group 1 licence
Contraception interactions: enzyme-inducing AEDs reduce efficacy
Pregnancy planning: folic acid supplementation, teratogenicity risks
Headache Red Flags
Subarachnoid Haemorrhage
Thunderclap onset reaching maximum intensity within 60 seconds
CT head within 6 hours: 100% sensitivity
LP required if CT negative: xanthochromia after 12 hours
Secondary Headache Triggers
New onset after 50 years
Progressive frequency or severity
Associated fever, neck stiffness, or neurological signs
Worse with Valsalva manoeuvres
Peripheral Neuropathy
Diabetic Neuropathy Management
Distal sensorimotor pattern recognition
First-line neuropathic pain treatment: pregabalin or duloxetine
Foot care education and regular screening
B12 Deficiency
Combined systems degeneration: peripheral neuropathy + spastic paraparesis
Serum B12 levels: treat if <200 pmol/L
Replacement: hydroxocobalamin injections
The Most Common Study Mistake
Students approach neurology anatomically but UKMLA tests it clinically. You spend hours memorising cranial nerve pathways, then face questions about when to order urgent MRI versus CT in suspected cauda equina syndrome.
The disconnect happens because anatomy knowledge doesnt translate directly to clinical decision-making. Knowing that CN III controls extraocular muscles wont help when the question asks about pupillary response timing in head injury assessment.
Instead of anatomy-first learning:
Start with clinical presentations
Learn investigation sequences
Master management protocols
Connect anatomy only when clinically relevant
Clinical presentation approach:
1. Patient presents with specific symptoms
2. What red flags require immediate action?
3. Which investigations confirm or exclude serious causes?
4. What treatment pathway does NICE recommend?
5. How do you monitor response and adjust management?
Clinical Reasoning Approach for UKMLA Neurology
Step 1: Recognise the Clinical Pattern
UKMLA presents neurology as clinical scenarios, not isolated symptoms. Learn to recognise:
Stroke alert presentations requiring immediate thrombolysis assessment
Seizure types determining AED selection
Headache patterns suggesting secondary causes
Neuropathy distributions indicating specific aetiologies
Step 2: Apply Investigation Sequencing
Each neurological presentation has an optimal investigation sequence based on urgency and diagnostic yield:
Acute stroke: CT head → CT angiography → consider MRI
Suspected epilepsy: EEG → MRI brain → consider video telemetry
Neuropathy: nerve conduction studies → consider specific blood tests
Step 3: Follow NICE Pathways
UKMLA questions often test knowledge of specific NICE guidelines:
TIA and stroke pathway timelines
Epilepsy diagnosis and management algorithms
Headache investigation protocols
Multiple sclerosis diagnostic criteria
Step 4: Consider Real-World Constraints
UKMLA includes practical considerations that pure medical knowledge misses:
ED resource availability affecting investigation timing
Patient factors influencing treatment choices
Follow-up requirements and monitoring protocols
Week-by-Week UKMLA Neurology Preparation
Week 1-2: Master High-Yield Clinical Presentations
Focus on pattern recognition for stroke, seizure, headache, and peripheral neuropathy. Use Oncourse's stroke and TIA lessons to build clinical reasoning frameworks rather than memorising isolated facts.
Practice with UKMLA neurology questions that emphasise decision-making over recall. Each question should build your ability to move from presentation to next appropriate step.
Week 3-4: Build Investigation and Management Protocols
Learn NICE pathway decision points and investigation sequences. Focus on when to choose specific imaging, which blood tests confirm diagnoses, and how treatment protocols progress.
Week 5-6: Integrate Clinical Reasoning Chains
Practice full clinical reasoning sequences: presentation → assessment → investigation → diagnosis → management. Use Oncourse's Clinical Rounds feature to work through complex neurology cases that mirror UKMLA's multi-step reasoning requirements.
Week 7-8: Consolidate with Spaced Repetition
Lock in the dense factual material using neurology flashcards. Focus on NIHSS criteria, AED dosing protocols, and headache red flag criteria so clinical reasoning isnt interrupted by knowledge gaps.
Oncourse AI for UKMLA Neurology Success
Clinical Rounds: Oncourse's neurology cases are built around real clinical presentations rather than anatomy drills. Work through stroke alerts, seizure workups, and headache differentials exactly as UKMLA presents them — as urgent clinical decisions requiring systematic reasoning. AI Probe Feature: Ask Oncourse "why is tissue plasminogen activator contraindicated here?" and receive clinical reasoning walkthroughs that build the logical chain, not just the answer. Essential for neurology where the "why" is what UKMLA actually tests. Spaced Repetition (Synapses): Lock in dense factual material — NIHSS thresholds, AED dosing, headache red flag criteria — so clinical reasoning sessions arent interrupted by gaps in baseline knowledge.
Frequently Asked Questions
How long does UKMLA neurology preparation take?
Plan 8 weeks for comprehensive neurology preparation. The clinical reasoning chains take longer to master than straightforward recall subjects. Allow 2 weeks each for stroke/TIA, epilepsy, headaches, and peripheral neuropathy.
Should I focus on anatomy or clinical presentations first?
Start with clinical presentations. UKMLA tests decision-making, not anatomical recall. Learn anatomy only when it directly impacts clinical management — like understanding stroke territories for thrombolysis decisions.
Which neurology guidelines are most important for UKMLA?
Focus on NICE guidelines for TIA/stroke pathways, epilepsy management, and headache investigation protocols. These directly inform UKMLA question content and clinical reasoning requirements.
How do I improve clinical reasoning speed for neurology questions?
Practice full reasoning chains repeatedly: presentation → red flags → investigations → management. Use Oncourse's Clinical Rounds to build systematic approaches that become automatic under exam pressure.
What are the most common UKMLA neurology traps?
Students often choose investigations that would eventually be needed rather than the next most appropriate step. Always consider urgency, resource availability, and NICE pathway sequences when selecting answers.
How important are drug interactions and side effects in UKMLA neurology?
Very important. Know AED interactions with contraception, monitoring requirements for different seizure medications, and contraindications for thrombolysis. These clinical considerations frequently appear in UKMLA questions.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for UKMLA success. Download free on Android and iOS.