Back
Sepsis and Septic Shock: High-Yield Clinical Reasoning and Management for NEET PG 2026
Master sepsis and septic shock for NEET PG 2026 with complete clinical reasoning framework covering Sepsis-3 definition, SOFA vs qSOFA scoring, cytokine cascade pathophysiology, vasopressor management, and 1-hour bundle protocols.

Sepsis and Septic Shock: High-Yield Clinical Reasoning and Management for NEET PG 2026
You are staring at a 65-year-old diabetic with fever, confusion, and blood pressure that wont respond to fluids. Heart rate 118, respirations 26, lactate 3.2 mmol/L. The stem screams septic shock, but the answer choices include distributive shock, SIRS, severe sepsis, and septic shock. This isnt about memorizing definitions — its about clinical reasoning that saves lives and gets you marks.
NEET PG 2026 expects you to think like an intensivist from the moment you see "fever + hypotension." The Sepsis-3 definition changed everything in 2016, throwing out SIRS criteria and bringing in organ dysfunction. Yet 47% of candidates still fall for SIRS-based trap answers. The cytokine cascade, SOFA scoring, and 1-hour antibiotic bundle aren't just high-yield — they are the foundation of every sepsis MCQ you will encounter.
Here's your complete clinical reasoning framework for sepsis mastery, built for the exam patterns that matter in 2026.
Understanding Sepsis-3 Definition: What Changed and Why It Matters
The 2016 Sepsis-3 definition eliminated the confusion that trapped students for decades. Forget SIRS criteria for sepsis diagnosis — they are gone. Sepsis is now defined as life-threatening organ dysfunction caused by dysregulated host response to infection.
Key terminology for NEET PG:
Sepsis: Suspected infection + SOFA score increase ≥2 points
Septic shock: Sepsis + persistent hypotension requiring vasopressors + lactate >2 mmol/L despite adequate fluid resuscitation
qSOFA: Bedside screening tool (altered mental status, SBP ≤100, RR ≥22)
The SIRS vs sepsis distinction is the #1 MCQ trap. SIRS (fever, tachycardia, tachypnea, leukocytosis) can occur without infection — burns, pancreatitis, trauma all trigger SIRS. Sepsis requires proven infection PLUS organ dysfunction. When Oncourse's AI-powered clinical case explanations walk through these scenarios, they emphasize the infection-first approach that distinguishes sepsis from sterile inflammation.
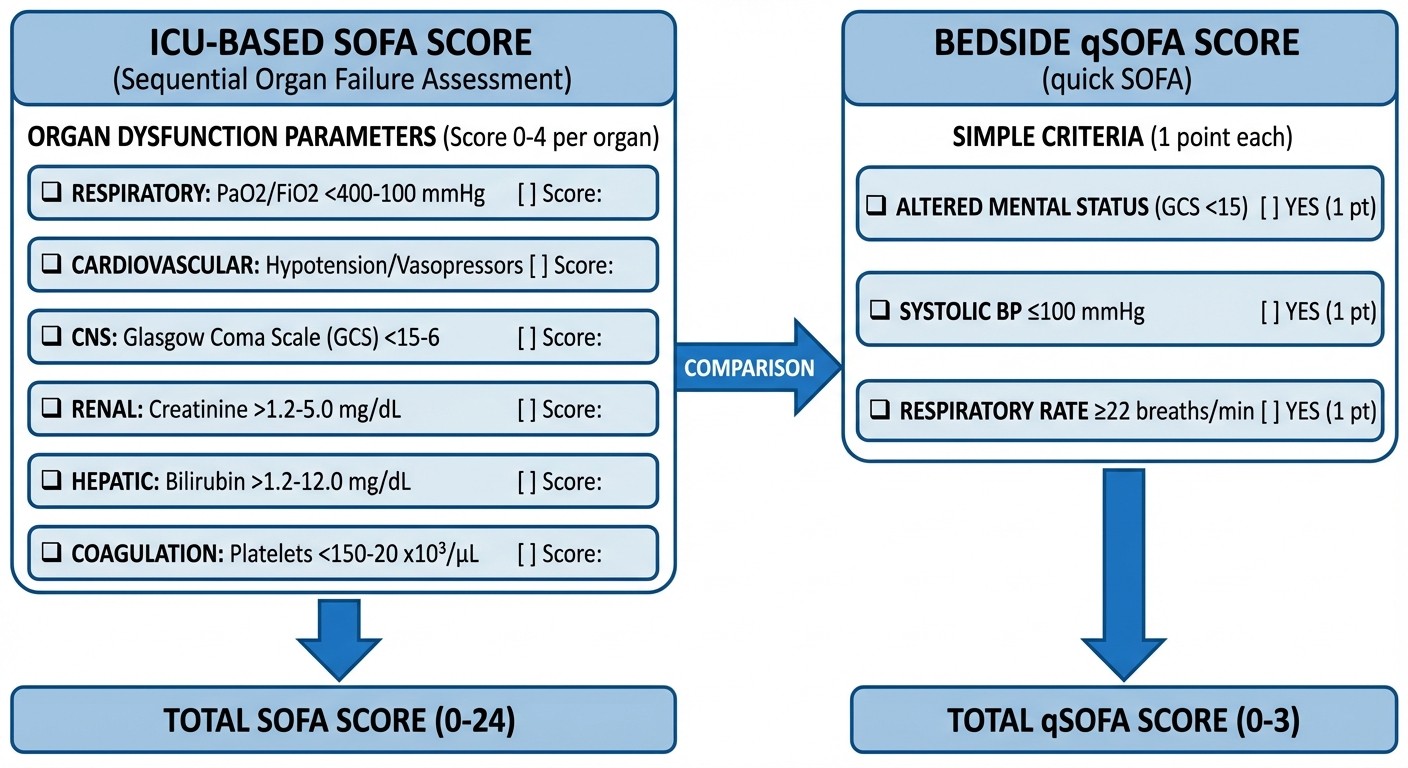
SOFA Score vs qSOFA: Clinical Application for NEET PG
Understanding when to use SOFA vs qSOFA determines your diagnostic accuracy in sepsis cases.
qSOFA (bedside screening):
Altered mental status (GCS <15)
Systolic blood pressure ≤100 mmHg
Respiratory rate ≥22/min
qSOFA ≥2 triggers suspicion, but doesnt diagnose sepsis. Think of it as a rapid screening tool for non-ICU settings. Sensitivity is only 59%, but specificity reaches 83% for mortality prediction.
SOFA Score (definitive assessment):
Organ System | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|---|
Respiratory (PaO2/FiO2) | >400 | 300-400 | 200-299 | 100-199 | <100 |
Cardiovascular | MAP ≥70 | MAP <70 | Dopamine ≤5 | Dopamine >5 or NE ≤0.1 | Dopamine >15 or NE >0.1 |
CNS (GCS) | 15 | 13-14 | 10-12 | 6-9 | <6 |
Renal (Creatinine mg/dL) | <1.2 | 1.2-1.9 | 2.0-3.4 | 3.5-4.9 | >5.0 |
Hepatic (Bilirubin mg/dL) | <1.2 | 1.2-1.9 | 2.0-5.9 | 6.0-11.9 | >12 |
Coagulation (Platelets) | >150 | 100-150 | 50-99 | 20-49 | <20 |
NEET PG trap: Questions present ICU patients and ask about qSOFA. Wrong. ICU patients get SOFA scoring. qSOFA is for wards, emergency, outpatient settings where full lab workup isnt immediately available.
Oncourse's spaced repetition system schedules these scoring criteria for optimal recall — SOFA cutoffs and vasopressor dosing thresholds appear repeatedly because they are classic stem elements in sepsis MCQs.
Pathophysiology: The Cytokine Cascade That Examiners Love
The inflammatory response in sepsis follows a predictable cascade that examiners test repeatedly. Master this sequence and you will recognize the pathophysiology behind every clinical manifestation.
Initial trigger: Pathogen-associated molecular patterns (PAMPs) from bacteria bind toll-like receptors on immune cells. Lipopolysaccharide (LPS) from gram-negative bacteria is the classic example. Cytokine storm: 1. TNF-α (tumor necrosis factor-alpha): First responder, triggers systemic inflammation 2. IL-1 (interleukin-1): Amplifies inflammatory response, causes fever 3. IL-6 (interleukin-6): Acute phase response, hepatic protein synthesis changes Compensatory Anti-inflammatory Response Syndrome (CARS): The body attempts to counterbalance with anti-inflammatory mediators like IL-10 and TGF-β. When this overshoots, patients become immunosuppressed and vulnerable to secondary infections. Distributive shock mechanism:
Massive vasodilation from nitric oxide release
Increased capillary permeability leading to third-spacing
Myocardial depression from cytokine effects
Microthrombosis and DIC from activated coagulation cascade
High-yield concept: Patients progress through compensated shock (normal blood pressure maintained by tachycardia and vasoconstriction) to decompensated shock (hypotension despite compensation). Lactate elevation reflects tissue hypoperfusion and anaerobic metabolism.
The microthrombi formation during DIC is a repeat-appearance topic that Oncourse's spaced repetition targets specifically — students often confuse the bleeding vs clotting phases of DIC in sepsis scenarios.
Clinical Recognition: Reading the Sepsis Case Stem
NEET PG sepsis questions follow predictable patterns. Train your pattern recognition with these stem elements:
Classic presentation triad: 1. Infection source: UTI, pneumonia, cellulitis, abdominal infection 2. Systemic manifestations: Fever/hypothermia, altered mental status, tachycardia 3. Organ dysfunction: Hypotension, oliguria, hypoxemia, thrombocytopenia Red flag combinations that scream sepsis:
Elderly diabetic + fever + confusion + hypotension = septic shock until proven otherwise
Post-operative patient + fever + tachycardia + increased oxygen requirement = hospital-acquired sepsis
Immunocompromised patient + any combination of fever/hypothermia + hemodynamic instability = sepsis
Lactate thresholds for NEET PG:
Normal: <2 mmol/L
Septic shock: >2 mmol/L + hypotension requiring vasopressors
Severe tissue hypoperfusion: >4 mmol/L (consider alternative causes)
When practicing with Oncourse's Clinical Rounds game, students make real-time septic shock management decisions under timed pressure, reinforcing the 1-hour bundle protocols and dopamine-vs-norepinephrine sequences that mirror exam conditions.
The Golden Hour: Sepsis Management Bundle
The 1-hour sepsis bundle is non-negotiable for NEET PG. Every element has been tested, and the sequence matters for MCQ answers.
Hour 1 priorities (all within 60 minutes): 1. Blood cultures before antibiotics (but dont delay antibiotics for cultures) 2. Broad-spectrum antibiotics based on suspected source 3. Lactate measurement for shock identification 4. Fluid resuscitation with crystalloids 5. Vasopressors if hypotension persists after fluid challenge
Fluid Resuscitation: Crystalloids First, Volume Matters
Initial fluid challenge: 30 mL/kg of crystalloid within 3 hours for hypotension or lactate ≥4 mmol/L. For a 70 kg patient, thats 2.1 liters. Crystalloid choice:
Normal saline (0.9% NaCl): Most commonly used, risk of hyperchloremic acidosis with large volumes
Balanced crystalloids (Ringer's lactate, PlasmaLyte): Preferred in recent guidelines, lower chloride content
NEET PG traps:
Colloids (albumin, HES) are NOT first-line for sepsis resuscitation
Avoid hypotonic fluids (5% dextrose) in septic patients
Dont restrict fluids in early sepsis due to fear of fluid overload
Fluid responsiveness assessment:
Stroke volume variation >13% on mechanical ventilation
Passive leg raise test showing >10% cardiac output increase
Central venous pressure is unreliable for fluid responsiveness
Vasopressor Therapy: Norepinephrine First-Line
When mean arterial pressure remains <65 mmHg despite adequate fluid resuscitation, vasopressors become essential.
First-line: Norepinephrine
Dosing: Start 0.01-0.03 mcg/kg/min, titrate up to 3 mcg/kg/min
Mechanism: α1-adrenergic agonist (vasoconstriction) + mild β1 effect
Target: MAP ≥65 mmHg
Second-line options:
Vasopressin: Add when norepinephrine >0.25 mcg/kg/min, dose 0.03 units/min (fixed dose)
Epinephrine: When norepinephrine + vasopressin insufficient, start 0.05-0.5 mcg/kg/min
Dobutamine: Add when cardiac index <2.5 L/min/m² despite adequate preload, dose 2-20 mcg/kg/min
Classic NEET PG trap: Dopamine is no longer first-line for septic shock. Increased arrhythmia risk compared to norepinephrine. Only consider in highly selected patients with low heart rate and low stroke volume. Steroid therapy: Hydrocortisone 200 mg/day only if shock remains refractory to high-dose vasopressors. Not routine first-line therapy.
Source Control: Timing Is Everything
Identifying and controlling the infection source determines survival more than any other intervention.
Immediate source control (within 6-12 hours):
Perforated viscus requiring surgical repair
Cholangitis requiring biliary decompression
Necrotizing fasciitis requiring debridement
Large abscesses amenable to drainage
Source control options:
Surgical: Open drainage, debridement, removal of infected devices
Percutaneous: CT or ultrasound-guided drainage of collections
Endoscopic: ERCP for biliary obstruction, bronchoscopy for pneumonia
Device removal: Central lines, urinary catheters, prosthetic material should be removed if infected, unless absolutely essential for life support.
Antibiotic Strategy: Empiric to Targeted
Broad-spectrum empiric antibiotics within 1 hour, then de-escalate based on culture results and clinical response.
Empiric antibiotic choices by source:
Community-acquired pneumonia: Ceftriaxone + azithromycin or fluoroquinolone
Hospital-acquired pneumonia: Piperacillin-tazobactam, meropenem, or cefepime
Complicated UTI: Fluoroquinolone or ceftriaxone
Intra-abdominal: Piperacillin-tazobactam or ceftriaxone + metronidazole
Special populations:
Neutropenic patients: Anti-pseudomonal β-lactam (cefepime, meropenem) + vancomycin if MRSA risk
Post-surgical: Cover skin flora (S. aureus) with vancomycin or linezolid if MRSA prevalent
Duration: 7-10 days for most infections, shorter courses (5-7 days) if rapid clinical improvement and source controlled.
Sepsis-3 vs SIRS: The MCQ Trap That Catches Everyone
Understanding why SIRS criteria were abandoned helps you avoid wrong answers.
Problems with SIRS-based sepsis definition:
Too sensitive: 90% of ICU patients meet SIRS criteria
Not specific: Occurs in non-infectious conditions (burns, pancreatitis)
Didnt predict mortality better than clinical judgment
Sepsis-3 advantages:
Organ dysfunction focus matches clinical reality
SOFA scoring provides objective measurement
Better mortality prediction than SIRS criteria
NEET PG application: When a question presents fever + tachycardia + leukocytosis but no organ dysfunction, the answer is SIRS, not sepsis. Sepsis requires organ dysfunction (SOFA increase ≥2).
Pediatric Sepsis: Age-Specific Considerations
Pediatric sepsis has different diagnostic criteria and management approaches.
Age-specific vital signs for SIRS:
0-1 month: HR >180, RR >50
1-12 months: HR >180, RR >40
1-5 years: HR >140, RR >30
6-12 years: HR >130, RR >25
Fluid resuscitation differences:
Initial bolus: 20 mL/kg over 5-20 minutes
Reassess after each bolus, may need multiple boluses
Watch for hepatomegaly as sign of fluid overload
Inotrope differences:
Epinephrine often used earlier in pediatric shock
Dobutamine preferred over dopamine for inotropic support
Frequently Asked Questions
What is the difference between sepsis and SIRS in the Sepsis-3 definition?
SIRS (Systemic Inflammatory Response Syndrome) is a non-specific inflammatory response that can occur with or without infection. It includes fever, tachycardia, tachypnea, and abnormal white cell count. Sepsis, under Sepsis-3, specifically requires suspected infection PLUS organ dysfunction (SOFA score increase ≥2 points). SIRS can occur in burns, trauma, or pancreatitis without infection, while sepsis always implies infectious cause with organ dysfunction.
When do you use qSOFA versus SOFA score for sepsis assessment?
Use qSOFA for rapid bedside screening in non-ICU settings (emergency department, medical wards) when you suspect sepsis but havent completed full laboratory workup. qSOFA requires only altered mental status, systolic BP ≤100 mmHg, and respiratory rate ≥22/min. Use SOFA score for definitive sepsis diagnosis and severity assessment, especially in ICU settings where complete lab values and monitoring are available.
What is the first-line vasopressor for septic shock and why?
Norepinephrine is first-line because it provides potent vasoconstriction (α1-adrenergic effect) to counteract the distributive shock of sepsis, with minimal cardiac stimulation compared to dopamine. Start at 0.01-0.03 mcg/kg/min and titrate to maintain MAP ≥65 mmHg. Dopamine is no longer first-line due to increased arrhythmia risk and less favorable hemodynamic profile.
What lactate level defines septic shock in the Sepsis-3 criteria?
Septic shock requires lactate >2 mmol/L plus persistent hypotension requiring vasopressors despite adequate fluid resuscitation. This combination indicates cellular hypoperfusion and circulatory failure. Lactate >4 mmol/L suggests severe tissue hypoperfusion and warrants aggressive resuscitation even without hypotension.
How much fluid should be given in the initial resuscitation of sepsis?
Give 30 mL/kg of crystalloid within the first 3 hours for patients with sepsis-induced hypotension or lactate ≥4 mmol/L. For a 70 kg patient, this equals 2.1 liters. Use balanced crystalloids when possible. Reassess after each 500 mL bolus and stop if signs of fluid overload develop.
What is the time frame for antibiotic administration in sepsis?
Administer broad-spectrum antibiotics within 1 hour of sepsis recognition. This is part of the hour-1 bundle that significantly reduces mortality. Choose empiric antibiotics based on suspected source and local resistance patterns, then de-escalate based on culture results and clinical response after 48-72 hours.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.
For comprehensive sepsis study materials, explore our NEET PG sepsis lessons, practice with sepsis MCQs, and reinforce key concepts using sepsis flashcards.