Back
Neuroanatomy Flashcards for USMLE Step 1 and NEET PG 2026: High-Yield Brain Regions, Spinal Cord Tracts and Cranial Nerve Mnemonics
Master neuroanatomy with high-yield flashcards for USMLE Step 1 and NEET PG 2026. Learn brain regions, spinal cord tracts, and cranial nerve mnemonics with clinical correlation strategies.

Neuroanatomy Flashcards for USMLE Step 1 and NEET PG 2026: High-Yield Brain Regions, Spinal Cord Tracts and Cranial Nerve Mnemonics
You are probably staring at your neuroanatomy flashcard deck wondering why you keep missing the same lesion localization questions. You flip through the cards — brain regions, check. Spinal cord tracts, memorized. Cranial nerve pathways, you know them cold. Yet when the exam throws a clinical vignette asking you to localize a Brown-Sequard syndrome or trace the corticospinal tract through three brainstem levels, you freeze.
Neuroanatomy makes up 12-15% of USMLE Step 1 and ranks among the highest-weighted anatomy topics for NEET PG 2026. The brutal truth? Most students treat it like a memorization game when it is actually a pattern recognition challenge. You dont just need to know what the posterior columns carry — you need to instantly connect "vibration loss below T10" to a specific lesion location while the exam clock ticks down.
The difference between knowing and actually recalling under pressure separates average scorers from those who dominate neuroanatomy questions. This guide shows you exactly which brain regions, spinal cord tracts, and cranial nerve patterns appear most frequently on both exams — plus the clinical pearl layer that turns passive flashcard knowledge into active diagnostic skills.
The Passive vs Active Recall Problem in Neuroanatomy
Most medical students start their neuroanatomy prep with community-curated Anki decks like AnKing. These decks are genuinely excellent as a foundational scaffold — they cover Netter diagrams, detailed spinal cord tract anatomy, and comprehensive cranial nerve pathways. The coverage is thorough, the images are high-quality, and the community has refined them over years.
The problem isnt with these decks. The problem is where students stop.
You flip a card showing the corticospinal tract, see the answer pathway, and think you know it. But knowing the tract exists is different from instantly localizing "upper motor neuron signs in the left leg only" to a specific brainstem level. Recognizing a CN III nucleus diagram is different from hearing "diplopia, ptosis, down-and-out gaze" and immediately thinking oculomotor palsy.
Active recall requires clinical integration. The best neuroanatomy learners use their foundational flashcard knowledge as a launching pad, then layer on clinical vignette practice and pattern recognition challenges. They dont just memorize the anatomy — they practice applying it under exam conditions.
This is where most students get stuck. They have the map (basic anatomical knowledge) but lack the GPS (clinical reasoning skills to navigate lesion localization questions efficiently).
High-Yield Brain Regions: The Big Four That Dominate Exams
1. Corticospinal Tract: Upper vs Lower Motor Neuron Lesions
The corticospinal tract appears in roughly 3-4 questions per USMLE Step 1 exam and is a NEET PG favorite for clinical correlation questions. Know these testable patterns:
Decussation at medulla (pyramids): 85% of fibers cross here
Above crossing: Upper motor neuron signs (spasticity, hyperreflexia, Babinski positive)
Below crossing: Lower motor neuron signs (flaccidity, hyporeflexia, fasciculations)
Clinical pearl: A lesion at C5 spinal level causes UMN signs in legs (tract already crossed) but LMN signs in arms (anterior horn cells affected). This mixed pattern is classic exam material.
For efficient review, each morning you can run through your foundational deck covering basic tract anatomy, then challenge yourself with Oncourse's daily mnemonic puzzles — like "I cross at the pyramids but spare the face — name my syndrome" to actively reconstruct the clinical picture rather than just recognizing it.
2. Thalamus: The Relay Station Everyone Forgets
Thalamic lesions create distinctive sensory patterns that both USMLE and NEET PG love testing:
VPL (Ventral Posterior Lateral): Body sensation below the neck VPM (Ventral Posterior Medial): Face sensation VPM lesions = contralateral hemifacial sensory loss VPL lesions = contralateral body sensory loss Clinical vignette pattern: "Pure sensory stroke" — sudden onset numbness affecting entire left side of face AND body points to right thalamic stroke affecting both VPM and VPL nuclei.
3. Basal Ganglia: Movement Disorders Made Simple
Focus on these two pathways:
Direct pathway: Cortex → Striatum → GPi/SNr (inhibited) → Thalamus (disinhibited) → Movement Indirect pathway: Cortex → Striatum → GPe → STN → GPi/SNr (activated) → Thalamus (inhibited) → No movement Parkinson's: Substantia nigra degeneration → indirect pathway dominates → bradykinesia, rigidity Huntington's: Striatal degeneration → direct pathway disrupted → chorea, hyperkinesia Exam trick: Questions often describe the movement pattern without naming the disease. "Progressive chorea with dementia in a 40-year-old" = Huntington's = striatal pathology.
4. Limbic System: Memory and Emotion Circuits
Hippocampus: Explicit memory formation (facts, events) Amygdala: Fear conditioning and emotional memory Mammillary bodies: Memory consolidation Classic lesion patterns:
Bilateral hippocampal damage: Anterograde amnesia (can't form new memories) — think patient H.M.
Wernicke-Korsakoff: Mammillary body damage → confabulation + anterograde amnesia
Klüver-Bucy syndrome: Bilateral amygdala lesions → hypersexuality, hyperorality, fearlessness
Consolidate your knowledge of these pathways with our comprehensive neuroanatomy lessons and test pattern recognition using targeted neuroanatomy questions.
Spinal Cord Tracts: The Four Syndromes You Must Know
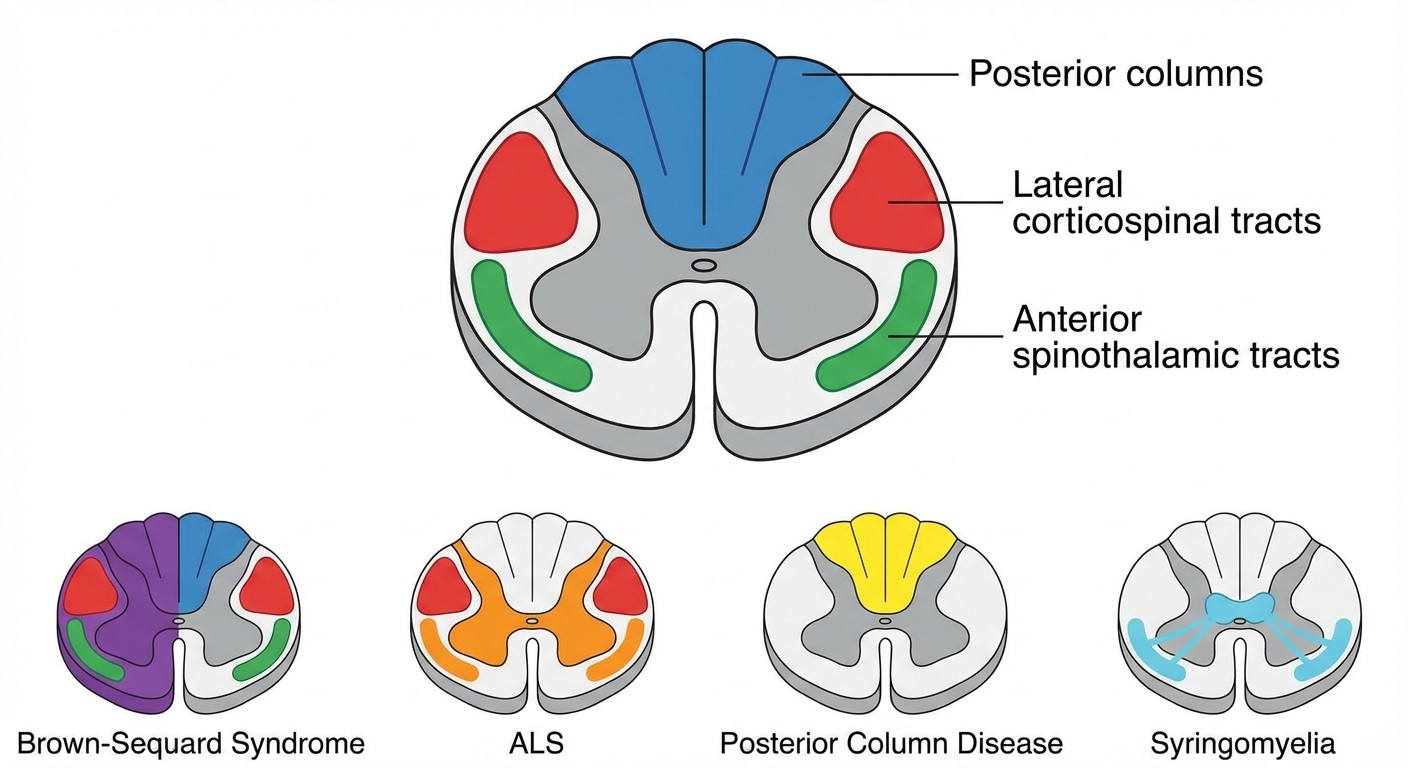
1. Brown-Sequard Syndrome: Hemisection Pattern
Lesion: Half of spinal cord destroyed (usually trauma) Ipsilateral findings:
Motor weakness (corticospinal tract)
Vibration/position loss (posterior columns)
Contralateral findings:
Pain/temperature loss (spinothalamic tract crosses immediately)
Exam clue: "Patient has right leg weakness with left leg pain sensation loss after knife wound"
2. Anterior Spinal Artery Syndrome
Blood supply: Anterior spinal artery supplies anterior 2/3 of cord Spared: Posterior columns (separate blood supply) Clinical pattern:
Bilateral motor weakness (corticospinal tracts)
Bilateral pain/temperature loss (spinothalamic tracts)
Preserved: Vibration and position sense
Exam presentation: "Sudden onset paraplegia with pain loss but intact vibration sense"
3. Posterior Column Disease: Tabes Dorsalis
Affected tracts: Fasciculus gracilis + cuneatus Cause: Tertiary syphilis (classic boards question) Clinical findings:
Loss of vibration below lesion level
Loss of position sense → sensory ataxia
Romberg positive: Can't balance with eyes closed
Exam pattern: "Unsteady gait that worsens in darkness" + positive RPR
4. Syringomyelia: Central Canal Expansion
Anatomical pattern: Central canal enlarges → damages crossing spinothalamic fibers Classic level: C8-T1 (cape-like distribution) Clinical presentation:
Dissociated sensory loss: Pain/temperature lost, vibration/position preserved
Distribution: Bilateral "cape" pattern over shoulders/arms
Associated: Often with Chiari malformation
Exam description: "Painless burns on hands, intact vibration sense"
The best way to cement these patterns is through spaced repetition with clinical correlation. Use spinal cord flashcards for anatomical foundation, then test syndrome recognition with clinical vignettes.
When reviewing these syndromes, try Oncourse's Synapses game — it generates neuroanatomy-specific word grouping challenges that force you to cluster symptoms into the right syndrome. Instead of just recognizing "Brown-Sequard" on a card, you actively group "ipsilateral motor loss, contralateral sensory loss, hemisection trauma" into the correct diagnosis.
Cranial Nerve Mnemonics: Beyond "Oh Oh Oh"
The Foundation Mnemonic
"Oh Oh Oh To Touch And Feel Very Green Vegetables AH"
(Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal)
This gets you the names. But exams dont ask for names — they ask for function and lesion patterns.
Functional Classification Tricks
All Motor: CN III, IV, VI, XI, XII (think "3-4-6-11-12") All Sensory: CN I, II, VIII (think "1-2-8") Mixed (motor + sensory): CN V, VII, IX, X (think "5-7-9-10")
High-Yield Cranial Nerve Lesion Patterns
#### CN III (Oculomotor) Palsy
Clinical triad: Diplopia + ptosis + "down and out" gaze
Pupil: If dilated → compressive lesion (aneurysm emergency)
Pupil: If normal → medical cause (diabetes, hypertension)
#### CN VII (Facial) Nerve
Upper motor neuron lesion: Forehead spared (bilateral innervation)
Lower motor neuron lesion: Complete facial paralysis including forehead
Bell's palsy pattern: LMN facial nerve palsy + hyperacusis + taste loss → lesion proximal to stylomastoid foramen
#### CN VIII (Vestibulocochlear)
Weber test: Conductive loss → sound lateralizes TO affected ear
Rinne test: Conductive loss → bone conduction > air conduction
Meniere's disease triad: Hearing loss + tinnitus + vertigo
#### CN X (Vagus) Lesion
Unilateral: Uvula deviates AWAY from lesion
Bilateral: Difficulty swallowing, lost gag reflex
For cranial nerve mastery, start with cranial nerve anatomy lessons to build your foundation, then practice pattern recognition with cranial nerve MCQs.
The daily Mnemonic challenge on Oncourse takes this further — instead of passively reviewing "CN III controls eye movement," you get clues like "I make the eye look down and out when damaged — which cranial nerve am I?" This active reconstruction builds the same mental pathways you'll use during the actual exam.
Beyond the AnKing Foundation: The Clinical Pearl Layer
The AnKing deck and similar community resources give you an excellent anatomical foundation. They cover every tract, every nucleus, every pathway with beautiful Netter illustrations. This foundational knowledge is absolutely essential — you need to know where things are before you can understand what happens when they break.
But here's what separates students who dominate neuroanatomy from those who struggle: the clinical pearl layer.
The foundation layer: Corticospinal tract crosses at the pyramids The clinical layer: A C5 lesion causes mixed UMN/LMN findings because the tract has already crossed for the legs but the local anterior horn cells are damaged for the arms The foundation layer: CN III controls most eye movements The clinical layer: Pupil-sparing CN III palsy in a diabetic = microvascular cause; pupil-involving palsy = consider posterior communicating artery aneurysm emergency The foundation layer: Posterior columns carry vibration and position The clinical layer: Patient with syphilis who falls in the shower with lights off = tabes dorsalis affecting posterior columns = Romberg positive
This clinical integration doesnt replace your foundational deck — it builds on top of it. The most efficient approach is a two-layer retention strategy: morning review of anatomical basics for breadth, evening practice with clinical vignettes for depth.
The Pattern Recognition Upgrade
Once you have solid anatomical knowledge, the next level is training pattern recognition under time pressure. Traditional flashcards show you isolated facts. Clinical questions test your ability to synthesize multiple clues into a diagnosis.
Example synthesis question:
"A 45-year-old diabetic presents with diplopia. Examination shows ptosis, eye positioned down and out, normal pupil size. Most likely diagnosis?"
Step 1: Recognize CN III palsy pattern (ptosis + down-and-out + diplopia) Step 2: Note pupil-sparing (rules out compressive lesion) Step 3: Connect diabetes history (microvascular cause) Answer: Diabetic CN III palsy
This multi-step reasoning is exactly what word grouping games train. When Oncourse generates a Synapses challenge grouping "ptosis, diplopia, diabetes, normal pupil" you're practicing the same synthesis pattern the exam tests.
Your 2-Week Neuroanatomy Sprint Strategy
Week 1: Foundation Building
Days 1-3: Complete cranial nerve basics using your existing flashcard deck + cranial nerve flashcards Days 4-5: Master spinal cord tract anatomy + basic lesion patterns Days 6-7: Brain region review focusing on thalamus, basal ganglia, limbic system
Week 2: Clinical Integration
Days 8-10: Clinical vignette practice — start with isolated syndrome recognition Days 11-12: Mixed practice combining multiple systems Days 13-14: Speed rounds + weak area review Daily routine throughout:
Morning: 30 minutes anatomical foundation review
Evening: 15 minutes clinical pattern practice using active recall challenges
Before bed: 5 minutes mnemonic reconstruction without looking at answers
High-Yield Resources by Exam Type
For USMLE Step 1 students:
Focus on lesion localization patterns over pure anatomy
Emphasize clinical correlations and pathophysiology
Practice with USMLE-specific neuroanatomy questions
For NEET PG 2026:
Equal weight on pure anatomy and clinical applications
Know classical presentations and eponymous syndromes
Master brain blood supply patterns (frequently tested)
Review with NEET PG neuroanatomy content
The key insight: neuroanatomy success comes from layering clinical reasoning on top of solid anatomical knowledge. Your existing foundation serves as the map — clinical integration gives you the GPS to navigate lesion localization questions efficiently.
Frequently Asked Questions
How long should I spend on neuroanatomy flashcards daily?
30-45 minutes total: 20-30 minutes for foundational anatomy review, 10-15 minutes for clinical vignette practice. Consistency beats marathon sessions.
Are community Anki decks enough for USMLE Step 1?
Community decks like AnKing provide excellent anatomical foundation, but you need to layer clinical correlation practice on top. Pure anatomy recognition doesnt equal lesion localization skills.
What's the highest-yield neuroanatomy topic for NEET PG?
Cranial nerve anatomy and clinical correlations. NEET PG heavily emphasizes classical presentations and syndrome recognition patterns.
Should I memorize every spinal tract pathway?
Focus on the big four: corticospinal, spinothalamic, posterior columns, and spinocerebellar. Know their lesion patterns cold rather than memorizing obscure tract details.
How do I improve at lesion localization questions?
Practice active synthesis: given a set of symptoms, work backwards to identify the anatomical location. Word grouping games help train this pattern recognition.
What's the best way to remember cranial nerve functions?
Layer functional mnemonics on top of the basic name sequence. Know the "3-4-6-11-12" motor pattern and practice connecting symptoms to specific nerve lesions.
Neuroanatomy mastery comes from building strong foundations then adding the clinical reasoning layer that separates top performers from the rest. The anatomy gives you the vocabulary — clinical integration teaches you to speak the language fluently.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 1 and NEET PG. Download free on Android and iOS.