
Brain and Neuroanatomy

On this page
🧠 The Cerebral Architecture: Your Brain's Command Center
Your brain orchestrates every thought, movement, and sensation through an elegant architecture of lobes, circuits, and vascular highways-and when injury strikes, predictable deficits emerge that reveal this hidden geography. This lesson maps the cerebral landscape from cortical zones to white matter tracts, then bridges anatomy to bedside by teaching you how specific lesions produce recognizable syndromes and how targeted therapies exploit these networks. You'll gain the spatial literacy to localize pathology, predict clinical presentations, and intervene with precision, transforming abstract neuroanatomy into a practical diagnostic and therapeutic tool.

Hemispheric Dominance: The Brain's Executive Division
The cerebral hemispheres exhibit functional asymmetry that defines human cognitive capabilities:
-
Left Hemisphere Dominance (85-90% of population)
- Language processing: Broca's area (areas 44-45), Wernicke's area (area 22)
- Mathematical reasoning and logical analysis
- Sequential processing and temporal ordering
- Dominant hand motor control
-
Right Hemisphere Specialization
- Spatial processing and visuospatial awareness
- Emotional processing and prosody recognition
- Holistic pattern recognition
- Non-dominant hand coordination
📌 Remember: LADS - Left hemisphere: Analytical, Dominant language, Sequential processing
Lobar Organization: Functional Territories
| Lobe | Primary Functions | Key Areas | Clinical Correlations | Vascular Supply |
|---|---|---|---|---|
| Frontal | Executive function, motor control | Areas 4, 6, 8-11, 44-47 | Personality changes, motor deficits | ACA, MCA |
| Parietal | Sensory integration, spatial awareness | Areas 1-3, 5, 7, 39-40 | Neglect syndromes, apraxia | MCA, PCA |
| Temporal | Auditory processing, memory | Areas 20-22, 27-28, 34-38 | Memory loss, language deficits | MCA, PCA |
| Occipital | Visual processing | Areas 17-19 | Visual field defects | PCA |
| Insular | Autonomic integration | Areas 13-16 | Pain processing, addiction | MCA branches |
Surface Anatomy: Landmark Navigation
The cerebral surface features critical landmarks for clinical localization:
-
Central Sulcus (Rolandic fissure)
- Separates frontal from parietal lobes
- Contains hand knob at 85% depth from superior margin
- Motor cortex anterior, sensory cortex posterior
-
Sylvian Fissure (Lateral sulcus)
- Separates temporal from frontal/parietal lobes
- Contains middle cerebral artery branches
- Depth reveals insular cortex
-
Parieto-occipital Sulcus
- Separates parietal from occipital lobes
- Visible on medial hemisphere surface
- Corresponds to primary visual cortex location
💡 Master This: The central sulcus identification transforms clinical examination - everything anterior controls movement, everything posterior processes sensation.
Understanding hemispheric organization provides the foundation for interpreting cortical function maps and predicting lesion effects across functional domains.
🧠 The Cerebral Architecture: Your Brain's Command Center


⚡ Cortical Cartography: The Brain's Functional GPS
Primary Cortical Areas: Core Processing Hubs
The primary cortical areas handle fundamental sensory and motor functions:
-
Primary Motor Cortex (M1, Area 4)
- Located in precentral gyrus
- Somatotopic organization: medial leg, lateral face
- 30% of neurons project directly to spinal cord
- Hand area occupies 25% of total motor strip
-
Primary Somatosensory Cortex (S1, Areas 1-3)
- Postcentral gyrus organization
- Area 3a: muscle proprioception
- Area 3b: cutaneous touch (largest representation)
- Areas 1-2: texture and shape discrimination
-
Primary Visual Cortex (V1, Area 17)
- Calcarine cortex in occipital lobe
- 140 million neurons process visual input
- Retinotopic mapping with macular sparing
- 6 cortical layers with specialized functions
-
Primary Auditory Cortex (A1, Areas 41-42)
- Superior temporal gyrus (Heschl's gyri)
- Tonotopic organization: high frequencies medial
- Bilateral representation of each ear
- Critical for temporal processing
📌 Remember: MASH - Motor precentral, Auditory superior temporal, Sensory postcentral, Hallucinations visual occipital
Association Areas: Integration Powerhouses
Association cortices integrate primary sensory inputs into complex perceptions and behaviors:
-
Prefrontal Association Areas
- Dorsolateral (Areas 9, 46): Working memory, executive control
- Orbitofrontal (Areas 10-11): Emotional regulation, decision-making
- Anterior Cingulate (Area 24): Attention, conflict monitoring
- Ventromedial (Area 25): Social cognition, empathy
-
Parietal Association Areas
- Superior Parietal (Area 7): Spatial attention, visuomotor integration
- Inferior Parietal (Areas 39-40): Language, mathematical processing
- Angular Gyrus (Area 39): Reading, semantic processing
- Supramarginal Gyrus (Area 40): Phonological processing
Loading diagram…
⭐ Clinical Pearl: Prefrontal lesions impair executive function in 90% of cases, while inferior parietal damage causes calculation deficits in 75% of dominant hemisphere lesions.
Language Networks: Communication Command Centers
Language processing involves distributed cortical networks with hemispheric specialization:
| Language Area | Location | Function | Lesion Effect | Frequency |
|---|---|---|---|---|
| Broca's Area | Areas 44-45 | Speech production | Expressive aphasia | 85% left hemisphere |
| Wernicke's Area | Area 22 | Speech comprehension | Receptive aphasia | 95% left hemisphere |
| Angular Gyrus | Area 39 | Reading, writing | Alexia, agraphia | 80% left hemisphere |
| Supramarginal | Area 40 | Phonological processing | Conduction aphasia | 70% left hemisphere |
| Arcuate Fasciculus | White matter tract | Connects language areas | Repetition deficits | Bilateral representation |
Understanding cortical functional maps enables precise localization of neurological deficits and guides targeted rehabilitation strategies across cognitive domains.
⚡ Cortical Cartography: The Brain's Functional GPS
🛣️ Neural Superhighways: The Brain's Information Networks
Association Fibers: Intrahemispheric Connections
Association fibers connect cortical areas within the same hemisphere, enabling integrated processing:
-
Short Association Fibers (U-fibers)
- Connect adjacent gyri
- 2-6 cm in length
- Most numerous white matter tracts
- Critical for local cortical integration
-
Long Association Fibers
- Superior Longitudinal Fasciculus (SLF): Frontal-parietal-temporal connections
- Inferior Longitudinal Fasciculus (ILF): Temporal-occipital visual processing
- Uncinate Fasciculus: Frontal-temporal emotional circuits
- Cingulum Bundle: Limbic system connections
Projection Fibers: Cortical-Subcortical Highways
Projection fibers carry information between cortex and subcortical structures:
-
Corona Radiata
- Fan-shaped fiber arrangement
- Connects cortex to internal capsule
- Anterior: Frontal connections
- Posterior: Parietal-occipital pathways
-
Internal Capsule Organization
- Anterior Limb: Frontopontine fibers, anterior thalamic radiations
- Genu: Corticobulbar fibers to cranial nerve nuclei
- Posterior Limb: Corticospinal tract, sensory radiations
- Retrolenticular: Optic radiations, temporopontine fibers
- Sublenticular: Auditory radiations, inferior optic radiations
Loading diagram…
📌 Remember: PLIC - Posterior Limb Internal Capsule contains corticospinal tract (motor) and sensory radiations
Commissural Fibers: Interhemispheric Bridges
Commissural fibers enable communication between cerebral hemispheres:
-
Corpus Callosum (200 million fibers)
- Rostrum: Orbitofrontal connections
- Genu: Frontal lobe connections
- Body: Motor and sensory connections
- Splenium: Parietal, temporal, occipital connections
-
Anterior Commissure
- Anterior part: Olfactory connections
- Posterior part: Temporal lobe connections
- Smaller than corpus callosum (3 million fibers)
-
Posterior Commissure
- Pretectal connections
- Pupillary light reflex pathway
- Superior colliculus connections
| Tract | Function | Clinical Significance | Lesion Effects |
|---|---|---|---|
| Corpus Callosum | Interhemispheric transfer | Split-brain syndrome | Disconnection symptoms |
| Arcuate Fasciculus | Language connectivity | Conduction aphasia | Repetition deficits |
| Optic Radiations | Visual processing | Quadrantanopia | Visual field cuts |
| Corticospinal Tract | Motor control | Hemiplegia | Contralateral weakness |
| Uncinate Fasciculus | Emotional processing | Temporal lobe epilepsy | Memory/emotional deficits |
Functional Connectivity Networks
Modern neuroimaging reveals large-scale brain networks:
-
Default Mode Network
- Medial prefrontal cortex, posterior cingulate, angular gyrus
- Active during rest and introspection
- Decreased activity during focused tasks
- Altered in depression, Alzheimer's disease
-
Executive Control Network
- Dorsolateral prefrontal cortex, posterior parietal cortex
- Goal-directed attention and cognitive control
- Working memory and decision-making
- Impaired in ADHD, schizophrenia
-
Salience Network
- Anterior insula, dorsal anterior cingulate
- Switches between internal and external attention
- Error detection and conflict monitoring
- Disrupted in autism, anxiety disorders
💡 Master This: White matter tract organization predicts disconnection syndromes - understanding pathway anatomy enables precise localization of cognitive deficits.
Mastering white matter anatomy transforms understanding of how focal lesions produce complex cognitive and behavioral syndromes through pathway disconnection.
🛣️ Neural Superhighways: The Brain's Information Networks
🎯 Vascular Territories: The Brain's Circulation Map
Anterior Circulation: Carotid Territory Dominance
The internal carotid system supplies 80% of cerebral blood flow through anterior and middle cerebral arteries:
-
Anterior Cerebral Artery (ACA) Territory
- Medial frontal and parietal cortex
- Anterior corpus callosum and cingulate gyrus
- Leg area of motor and sensory cortex
- Supplementary motor area and prefrontal cortex
-
Middle Cerebral Artery (MCA) Territory
- Lateral frontal, parietal, and temporal cortex
- Basal ganglia (lenticulostriate arteries)
- Internal capsule (anterior circulation portion)
- Language areas (dominant hemisphere)
MCA Stroke Syndromes: Pattern Recognition
MCA strokes produce the most common cerebrovascular syndromes:
| MCA Division | Territory | Clinical Syndrome | Frequency |
|---|---|---|---|
| Main Stem | Entire MCA territory | Complete MCA syndrome | 15% of MCA strokes |
| Superior Division | Frontal-parietal | Broca's aphasia, arm weakness | 35% of MCA strokes |
| Inferior Division | Temporal-parietal | Wernicke's aphasia, visual field cut | 25% of MCA strokes |
| Lenticulostriate | Basal ganglia | Pure motor hemiparesis | 20% of MCA strokes |
| Cortical Branches | Specific gyri | Focal deficits | 5% of MCA strokes |
Loading diagram…
Posterior Circulation: Vertebrobasilar Territory
The vertebrobasilar system supplies 20% of cerebral blood flow to posterior brain regions:
-
Posterior Cerebral Artery (PCA) Territory
- Occipital cortex and visual areas
- Medial temporal lobe and hippocampus
- Posterior corpus callosum and splenium
- Thalamus (posterior circulation portion)
-
Vertebrobasilar Territory
- Brainstem (medulla, pons, midbrain)
- Cerebellum (PICA, AICA, SCA)
- Posterior thalamus and subthalamus
- Posterior limb internal capsule (partial)
Watershed Zones: Vulnerable Borderlands
Watershed areas represent vascular borderlands susceptible to hypoperfusion:
-
Cortical Watersheds
- ACA-MCA border: Parasagittal frontal-parietal
- MCA-PCA border: Temporo-occipital junction
- Vulnerable during hypotension (systolic <90 mmHg)
-
Subcortical Watersheds
- Deep white matter between cortical and deep perforators
- Centrum semiovale and corona radiata
- Periventricular white matter in elderly
| Vascular Territory | Blood Flow | Clinical Deficits | Collateral Potential |
|---|---|---|---|
| ACA | 250 ml/min | Leg weakness, abulia | Good via AComA |
| MCA | 400 ml/min | Hemiplegia, aphasia | Limited leptomeningeal |
| PCA | 100 ml/min | Hemianopia, memory loss | Moderate via PComA |
| Vertebrobasilar | 200 ml/min | Brainstem signs, ataxia | Poor end-artery supply |
Venous Drainage: The Return Highway
Cerebral venous drainage follows predictable patterns with clinical implications:
-
Superficial Venous System
- Superior sagittal sinus: Drains superior cortex
- Inferior sagittal sinus: Drains medial cortex
- Transverse sinuses: Drain temporal-occipital regions
- Sigmoid sinuses: Connect to internal jugular veins
-
Deep Venous System
- Internal cerebral veins: Drain deep white matter
- Basal veins of Rosenthal: Drain basal forebrain
- Great vein of Galen: Collects deep drainage
- Straight sinus: Drains to confluence of sinuses
💡 Master This: Vascular territory knowledge enables rapid stroke localization - deficit pattern immediately suggests arterial involvement and guides acute intervention timing.
Understanding cerebrovascular anatomy transforms stroke evaluation from symptom description to precise anatomical localization and targeted therapeutic intervention.
🎯 Vascular Territories: The Brain's Circulation Map


🔧 Clinical Correlation Matrix: Lesion-Deficit Mapping
Frontal Lobe Syndromes: Executive Dysfunction Patterns
Frontal lobe lesions produce characteristic behavioral and cognitive changes:
-
Dorsolateral Prefrontal Syndrome
- Executive dysfunction: Planning, working memory deficits
- Perseveration: Inability to shift cognitive sets
- Apathy: Reduced motivation and initiative
- Wisconsin Card Sort Test: <50% categories completed
-
Orbitofrontal Syndrome
- Disinhibition: Inappropriate social behavior
- Emotional lability: Rapid mood changes
- Poor judgment: Risky decision-making
- Personality changes: 85% of patients show alterations
-
Medial Frontal Syndrome
- Akinetic mutism: Reduced speech and movement
- Abulia: Lack of will or motivation
- Urinary incontinence: Loss of bladder control
- Gait apraxia: Difficulty initiating walking
📌 Remember: DOA - Dorsolateral (executive), Orbitofrontal (disinhibition), Anterior cingulate (akinetic)
Parietal Lobe Syndromes: Integration Failures
Parietal lesions disrupt sensory integration and spatial processing:
| Syndrome | Location | Key Features | Frequency |
|---|---|---|---|
| Neglect | Right parietal | Ignores left space | 85% right hemisphere |
| Apraxia | Left parietal | Cannot perform learned movements | 70% left hemisphere |
| Acalculia | Angular gyrus | Cannot calculate | 90% left hemisphere |
| Agraphia | Supramarginal | Cannot write | 80% left hemisphere |
| Astereognosis | Postcentral | Cannot recognize objects by touch | Bilateral representation |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |||
| flowchart TD |
Start["🧠 Parietal Lesion
• Cortical injury• Brain pathology"]
Hemi{"↔️ Hemisphere
• Lateralization• Side of lesion"}
RightSide["📐 Spatial Deficits
• Non-dominant side• Visual processing"]
Neglect["🚫 Neglect Syndrome
• Hemispatial neglect• Left-side ignore"]
ConstAp["🧱 Const. Apraxia
• Drawing deficits• Spatial assembly"]
LeftSide["🔡 Lang/Calculat.
• Dominant side• Symbolic tasks"]
Gerstmann["🧮 Gerstmann Syn.
• Specific cluster• Left side focal"]
Ideomotor["🎭 Ideomotor Apr.
• Motor planning• Execution deficit"]
GerstDetails["📑 Triad Symptoms
• Acalculia/Agraphia• Finger Agnosia"]
Start --> Hemi Hemi -->|Right| RightSide Hemi -->|Left| LeftSide
RightSide --> Neglect RightSide --> ConstAp
LeftSide --> Gerstmann LeftSide --> Ideomotor
Gerstmann --> GerstDetails
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Hemi fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style RightSide fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style LeftSide fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Neglect fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style ConstAp fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Gerstmann fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Ideomotor fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style GerstDetails fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
### Temporal Lobe Syndromes: Memory and Language Disruption
Temporal lobe lesions affect memory, language, and emotional processing:
* **Hippocampal Lesions**
- **Anterograde amnesia**: Cannot form new memories
- **Retrograde amnesia**: **Temporal gradient** (recent > remote)
- **Preserved procedural memory**: Motor skills intact
- **Bilateral damage**: **Severe global amnesia** (HM case)
* **Dominant Temporal Lobe**
- **Wernicke's aphasia**: Fluent but meaningless speech
- **Anomic aphasia**: Word-finding difficulties
- **Alexia**: Reading comprehension deficits
- **Verbal memory impairment**: **Story recall <5th percentile**
* **Non-dominant Temporal Lobe**
- **Visuospatial memory deficits**: Cannot recall complex figures
- **Prosody impairment**: Flat emotional speech
- **Musical processing deficits**: Amusia
- **Face recognition problems**: Prosopagnosia (bilateral)
> ⭐ **Clinical Pearl**: Temporal lobe epilepsy causes **memory impairment in 60%** of patients, with **verbal memory deficits** from left-sided foci and **visuospatial deficits** from right-sided foci.
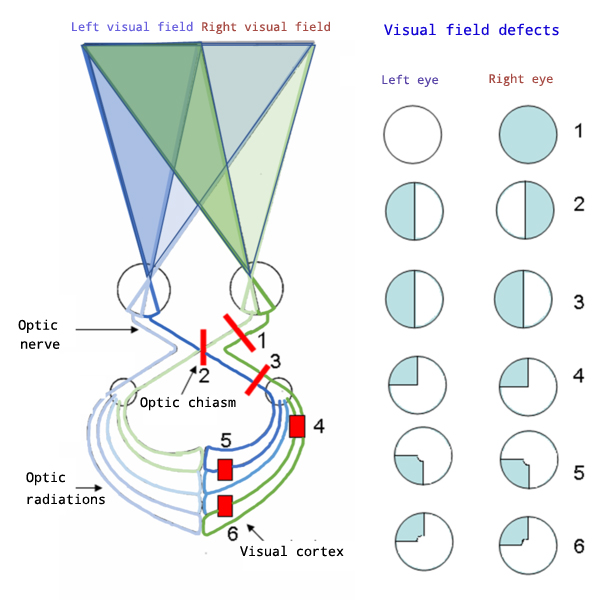
### Occipital Lobe Syndromes: Visual Processing Failures
Occipital lesions produce specific visual field defects and processing disorders:
* **Primary Visual Cortex (V1) Lesions**
- **Homonymous hemianopia**: **Macular sparing** in **90%**
- **Cortical blindness**: Bilateral V1 damage
- **Anton's syndrome**: Denial of blindness
- **Visual field defects**: **Congruent** and **complete**
* **Visual Association Area Lesions**
- **Achromatopsia**: Color vision loss (V4 area)
- **Akinetopsia**: Motion blindness (V5/MT area)
- **Visual agnosia**: Cannot recognize objects
- **Simultanagnosia**: Cannot see multiple objects
| Visual Deficit | Location | Characteristics | Recovery Rate |
|----------------|----------|-----------------|---------------|
| **Hemianopia** | V1 | **Congruent, macular sparing** | **30%** partial recovery |
| **Quadrantanopia** | Temporal/parietal radiations | **Incongruent** | **60%** improvement |
| **Scotoma** | Partial V1 | **Central or paracentral** | **70%** adaptation |
| **Cortical Blindness** | Bilateral V1 | **Complete vision loss** | **15%** recovery |> 💡 **Master This**: Visual field defect patterns immediately localize lesions - **congruent defects** indicate occipital cortex, **incongruent defects** suggest optic radiations.
### Disconnection Syndromes: When Pathways Break
White matter lesions produce disconnection syndromes by interrupting information flow:
* **Callosal Disconnection**
- **Left hand apraxia**: Cannot follow verbal commands
- **Alien hand syndrome**: Involuntary left hand movements
- **Interhemispheric transfer deficits**: **Split-brain phenomena**
* **Arcuate Fasciculus Lesions**
- **Conduction aphasia**: **Fluent speech, good comprehension, poor repetition**
- **Phonemic paraphasias**: Sound substitution errors
- **Preserved reading and writing**: **Unlike other aphasias**
* **Uncinate Fasciculus Damage**
- **Temporal lobe disconnection**: Memory and emotional deficits
- **Semantic processing impairment**: Word meaning difficulties
- **Personality changes**: **Frontal-temporal disconnection**
Understanding lesion-deficit correlations transforms neurological examination from symptom collection to precise anatomical diagnosis and targeted intervention planning.
🔧 Clinical Correlation Matrix: Lesion-Deficit Mapping

⚖️ Therapeutic Targeting: Precision Intervention Strategies
Surgical Intervention Strategies
Neurosurgical approaches utilize anatomical landmarks for precise therapeutic targeting:
-
Deep Brain Stimulation (DBS) Targets
- Subthalamic Nucleus: Parkinson's disease (70% improvement in motor scores)
- Globus Pallidus Interna: Dystonia (85% reduction in symptoms)
- Ventral Intermediate Thalamus: Essential tremor (90% tremor reduction)
- Anterior Limb Internal Capsule: Treatment-resistant depression
-
Epilepsy Surgery Principles
- Temporal Lobectomy: 65-80% seizure freedom in mesial temporal sclerosis
- Lesionectomy: 70-90% success for focal cortical dysplasia
- Corpus Callosotomy: 50-80% reduction in drop attacks
- Functional Hemispherectomy: 80-90% seizure control in hemispheric syndromes
Loading diagram…
Pharmacological Targeting Strategies
Drug interventions target specific neurotransmitter systems based on anatomical distribution:
| Target System | Anatomical Distribution | Therapeutic Applications | Efficacy Rates |
|---|---|---|---|
| Dopaminergic | Substantia nigra → striatum | Parkinson's disease | 70-80% motor improvement |
| Cholinergic | Basal forebrain → cortex | Alzheimer's disease | 30-40% cognitive stabilization |
| GABAergic | Widespread cortical | Epilepsy, anxiety | 60-70% seizure reduction |
| Glutamatergic | Cortical-subcortical | Stroke neuroprotection | 15-25% outcome improvement |
| Serotonergic | Raphe → limbic system | Depression | 60-70% response rates |
Rehabilitation Targeting Approaches
Rehabilitation strategies exploit neuroplasticity mechanisms through anatomically-informed interventions:
-
Constraint-Induced Movement Therapy
- Targets: Perilesional motor cortex reorganization
- Protocol: 90% restraint of unaffected limb for 6 hours daily
- Outcomes: Significant improvement in 80% of chronic stroke patients
- Mechanism: Forces use-dependent plasticity in damaged hemisphere
-
Aphasia Rehabilitation Protocols
- Melodic Intonation Therapy: Exploits right hemisphere musical processing
- Constraint-Induced Language Therapy: 3-4 hours daily intensive practice
- Transcranial Stimulation: Enhances left hemisphere recovery
- Success rates: 40-60% meaningful improvement in chronic aphasia
-
Cognitive Rehabilitation Strategies
- Working Memory Training: Targets dorsolateral prefrontal circuits
- Attention Process Training: Hierarchical difficulty progression
- Executive Function Training: Problem-solving and planning tasks
- Transfer effects: 30-50% improvement in untrained tasks
⭐ Clinical Pearl: Rehabilitation timing matters - intensive therapy within 3 months post-stroke yields 2-3x greater improvement than delayed intervention due to critical period plasticity.
Neuromodulation Techniques
Non-invasive brain stimulation targets specific cortical regions for therapeutic benefit:
-
Transcranial Magnetic Stimulation (TMS)
- High-frequency (>5 Hz): Increases cortical excitability
- Low-frequency (<1 Hz): Decreases cortical activity
- Depression treatment: Left DLPFC stimulation, 50-60% response
- Stroke recovery: Contralesional inhibition enhances recovery
-
Transcranial Direct Current Stimulation (tDCS)
- Anodal stimulation: Increases neuronal excitability
- Cathodal stimulation: Decreases cortical activity
- Aphasia treatment: Left hemisphere anodal stimulation
- Motor recovery: Ipsilesional facilitation + contralesional inhibition
| Technique | Target Precision | Treatment Duration | Success Rates | Side Effects |
|---|---|---|---|---|
| DBS | <1 mm accuracy | Continuous | 70-90% | 5-10% complications |
| TMS | 5-10 mm resolution | Daily sessions | 50-70% | <1% seizure risk |
| tDCS | 25-50 cm² area | 20-30 minutes | 30-50% | Minimal side effects |
| Focused Ultrasound | <1 mm precision | Single session | 80-95% | <5% complications |
Precision neuroterapeutics transforms treatment from empirical approaches to anatomically-guided interventions that maximize therapeutic benefit through targeted pathway modulation.
⚖️ Therapeutic Targeting: Precision Intervention Strategies

🔗 Integration Networks: The Connectome Architecture
Large-Scale Brain Networks: Functional Orchestration
Modern neuroimaging reveals 7 major functional networks that operate across anatomical boundaries:
-
Default Mode Network (DMN)
- Core hubs: Medial prefrontal cortex, posterior cingulate, angular gyrus
- Function: Self-referential thinking, autobiographical memory
- Deactivation: 60-80% reduction during focused tasks
- Clinical relevance: Altered in depression, Alzheimer's, schizophrenia
-
Executive Control Network (ECN)
- Key regions: Dorsolateral prefrontal cortex, posterior parietal cortex
- Function: Goal-directed attention, cognitive control
- Working memory: 7±2 items capacity limitation
- Disorders: Impaired in ADHD, autism, traumatic brain injury
-
Salience Network (SN)
- Primary nodes: Anterior insula, dorsal anterior cingulate
- Function: Switches between internal and external attention
- Response time: 150-300 ms for salience detection
- Pathology: Disrupted in anxiety, PTSD, addiction
Network Connectivity Patterns
Brain networks exhibit specific connectivity characteristics that enable functional specialization:
| Network | Within-Network Connectivity | Between-Network Connectivity | Clinical Implications |
|---|---|---|---|
| DMN | High positive correlation | Anti-correlated with task-positive | Hyperconnectivity in depression |
| ECN | Moderate positive correlation | Flexible task-dependent | Hypoconnectivity in ADHD |
| SN | Strong positive correlation | Mediates network switching | Altered switching in autism |
| Visual | Very high correlation | Minimal cross-network | Preserved in most disorders |
| Motor | High correlation | Connected to planning networks | Disrupted in movement disorders |
Developmental Network Maturation
Brain networks undergo systematic developmental changes that explain age-related cognitive capabilities:
-
Childhood (5-12 years)
- Local connectivity: Increases by 40%
- Long-range connections: Gradual strengthening
- Network segregation: Progressive specialization
- Cognitive impact: Improved attention, working memory
-
Adolescence (13-18 years)
- Default mode network: Adult-like organization emerges
- Executive control: Continued strengthening until age 25
- Risk-taking behavior: Immature prefrontal-limbic connections
- Myelination: White matter increases 30%
-
Aging (>65 years)
- Network connectivity: 10-15% decline per decade
- Compensatory mechanisms: Bilateral recruitment
- Default mode: Reduced deactivation
- Cognitive reserve: Education provides 20-30% protection
Loading diagram…
Network-Based Disorders
Many neurological and psychiatric conditions reflect network-level dysfunction rather than focal lesions:
-
Alzheimer's Disease
- Default mode network: Early and severe disruption
- Posterior cingulate: First region affected
- Network spread: Follows anatomical connectivity
- Cognitive decline: Correlates with network breakdown
-
Schizophrenia
- Salience network: Hyperactivity leads to aberrant salience
- Default mode: Reduced deactivation during tasks
- Executive control: Hypoconnectivity causes cognitive deficits
- Auditory hallucinations: Abnormal language network activity
-
Depression
- Default mode: Hyperconnectivity promotes rumination
- Executive control: Hypoconnectivity impairs cognitive control
- Limbic networks: Increased emotional reactivity
- Treatment response: Network normalization predicts recovery
⭐ Clinical Pearl: Network connectivity measures predict treatment response in 70-80% of depression cases, with default mode hyperconnectivity indicating need for intensive intervention.
Therapeutic Network Targeting
Network-based interventions target connectivity patterns rather than individual brain regions:
-
Neurofeedback Training
- Real-time network monitoring: fMRI or EEG feedback
- Default mode regulation: Reduces rumination in depression
- Attention network training: Improves ADHD symptoms
- Success rates: 50-70% improvement in targeted symptoms
-
Network-Guided TMS
- Connectivity-based targeting: Individual network mapping
- Default mode modulation: Subgenual cingulate stimulation
- Executive enhancement: Dorsolateral prefrontal stimulation
- Precision improvement: 30-40% better outcomes than standard targeting
| Intervention | Network Target | Mechanism | Clinical Outcomes |
|---|---|---|---|
| Meditation | Default mode regulation | Attention training | 40-60% anxiety reduction |
| Cognitive Training | Executive network | Working memory enhancement | 20-30% transfer effects |
| Psychotherapy | Emotion regulation networks | Top-down control | 60-80% depression response |
| Pharmacotherapy | Neurotransmitter networks | Chemical modulation | 50-70% symptom improvement |
Network-level understanding transforms neurological practice from symptom-based treatment to connectivity-guided precision interventions that target the root causes of brain dysfunction.
🔗 Integration Networks: The Connectome Architecture


🎯 Clinical Mastery Arsenal: Rapid Assessment Tools
Rapid Localization Framework
The 4-Level Localization System enables systematic anatomical correlation:
-
Level 1: Supratentorial vs Infratentorial
- Supratentorial signs: Hemiparesis, aphasia, visual field cuts
- Infratentorial signs: Cranial nerve deficits, ataxia, crossed signs
- Decision time: <30 seconds from presentation
- Accuracy: >95% for experienced clinicians
-
Level 2: Cortical vs Subcortical
- Cortical signs: Aphasia, neglect, apraxia, seizures
- Subcortical signs: Pure motor/sensory deficits, movement disorders
- Key discriminator: Higher cortical functions preserved in subcortical lesions
- Clinical pearl: Face-arm-leg equal weakness suggests subcortical
-
Level 3: Vascular Territory
- ACA: Leg > arm weakness, abulia, urinary incontinence
- MCA: Arm > leg weakness, aphasia, visual field cut
- PCA: Isolated visual deficits, memory loss, alexia
- Vertebrobasilar: Cranial nerves, ataxia, crossed signs
-
Level 4: Specific Anatomical Structure
- Precise localization: Individual gyri, nuclei, tracts
- Surgical planning: Millimeter accuracy required
- Functional mapping: Intraoperative confirmation
📌 Remember: SLIC - Supratentorial/infratentorial, Level (cortical/subcortical), Ischemic territory, Circuit/structure
Essential Clinical Correlations
| Clinical Sign | Anatomical Location | Vascular Territory | Urgency Level |
|---|---|---|---|
| Broca's Aphasia | Left frontal operculum | MCA superior division | High |
| Wernicke's Aphasia | Left superior temporal | MCA inferior division | High |
| Homonymous Hemianopia | Occipital cortex/optic radiations | PCA territory | Moderate |
| Pure Motor Hemiparesis | Internal capsule/corona radiata | Lenticulostriate arteries | High |
| Horner's Syndrome | Sympathetic pathway | Various levels | Variable |
| Internuclear Ophthalmoplegia | Medial longitudinal fasciculus | Paramedian brainstem | Moderate |
FAST-PLUS Assessment expands traditional stroke recognition:
- F - Face: Facial droop (cranial nerve VII, supranuclear)
- A - Arms: Arm drift (corticospinal tract, internal capsule)
- S - Speech: Aphasia/dysarthria (language areas, brainstem)
- T - Time: Onset timing (treatment window determination)
- P - Posterior: Ataxia, vertigo, visual loss (vertebrobasilar)
- L - Large vessel: Severe deficits (proximal occlusion)
- U - Unusual: Young age, unusual presentation
- S - Severity: NIHSS score (treatment eligibility)
Loading diagram…
Cognitive Assessment Rapid Screen
Montreal Cognitive Assessment (MoCA) Anatomical Correlations:
- Visuospatial/Executive (Clock, cube): Right parietal, frontal
- Naming (Animals): Left temporal, angular gyrus
- Attention (Digits, vigilance): Frontal-parietal networks
- Language (Repetition, fluency): Left hemisphere language areas
- Abstraction (Similarities): Dorsolateral prefrontal cortex
- Memory (Delayed recall): Hippocampus, medial temporal
- Orientation (Time, place): Posterior parietal, temporal
⭐ Clinical Pearl: MoCA scores <26 indicate cognitive impairment in 90% of cases, with domain-specific deficits localizing to corresponding anatomical regions.
Emergency Neuroanatomical Priorities
Life-Threatening Anatomical Emergencies requiring immediate intervention:
-
Brainstem Compression
- Signs: Altered consciousness, abnormal breathing, pupillary changes
- Anatomy: Reticular activating system, respiratory centers
- Action: Immediate neurosurgical consultation
- Time window: Minutes to hours
-
Increased Intracranial Pressure
- Signs: Headache, vomiting, papilledema, Cushing's triad
- Anatomy: Monro-Kellie doctrine (brain + blood + CSF)
- Action: Osmotic therapy, surgical decompression
- Critical threshold: >20 mmHg sustained
-
Spinal Cord Compression
- Signs: Bilateral weakness, sensory level, bladder dysfunction
- Anatomy: Corticospinal tracts, dorsal columns
- Action: High-dose steroids, emergency decompression
- Time window: <24 hours for optimal recovery
Bedside Localization Tools
Quick Reference Anatomical Correlations:
-
Cranial Nerve Quick Check
- CN II: Visual fields, pupils
- CN III, IV, VI: Eye movements, ptosis
- CN V: Facial sensation, jaw muscles
- CN VII: Facial movement, taste
- CN VIII: Hearing, balance
- CN IX, X: Swallowing, voice
- CN XI: Shoulder shrug, head turn
- CN XII: Tongue movement
-
Motor System Hierarchy
- Upper motor neuron: Spasticity, hyperreflexia, Babinski
- Lower motor neuron: Flaccidity, atrophy, fasciculations
- Extrapyramidal: Rigidity, tremor, bradykinesia
- Cerebellar: Ataxia, dysmetria, intention tremor
💡 Master This: Systematic neuroanatomical assessment transforms complex presentations into precise localizations - master these tools for rapid clinical decision-making in acute neurological emergencies.
These rapid assessment tools enable immediate anatomical correlation at the bedside, transforming neurological examination from descriptive observation to precise diagnostic localization.
🎯 Clinical Mastery Arsenal: Rapid Assessment Tools
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more












Have doubts about this lesson?
Ask Rezzy, your AI Study Partner, to explain anything you didn't understand
Everything you need for NEET-PG prep
Get full Oncourse access with lessons, practice questions, flashcards and AI study tools.
Scan to download app