Back
NEET PG Respiratory Pharmacology Glossary 2026 — Bronchodilators, Antitussives & High-Yield Drugs
Complete NEET PG respiratory pharmacology glossary covering bronchodilators, antitussives, and high-yield drugs. Beta-2 agonists, anticholinergics, corticosteroids, and exam-focused drug mechanisms.

NEET PG Respiratory Pharmacology Glossary 2026 — Bronchodilators, Antitussives & High-Yield Drugs
You're probably staring at a 20-page respiratory pharmacology chapter thinking "how am I supposed to remember all these drug names AND their mechanisms?" NEET PG loves testing respiratory drugs — 8-12 questions per year across pharmacology and medicine. The good news? Most questions test the same 25 high-yield drugs with predictable patterns.
This glossary breaks down every drug you need to know, organized by mechanism and clinical use. No fluff, just the exam-relevant facts that separate correct answers from attractive distractors.
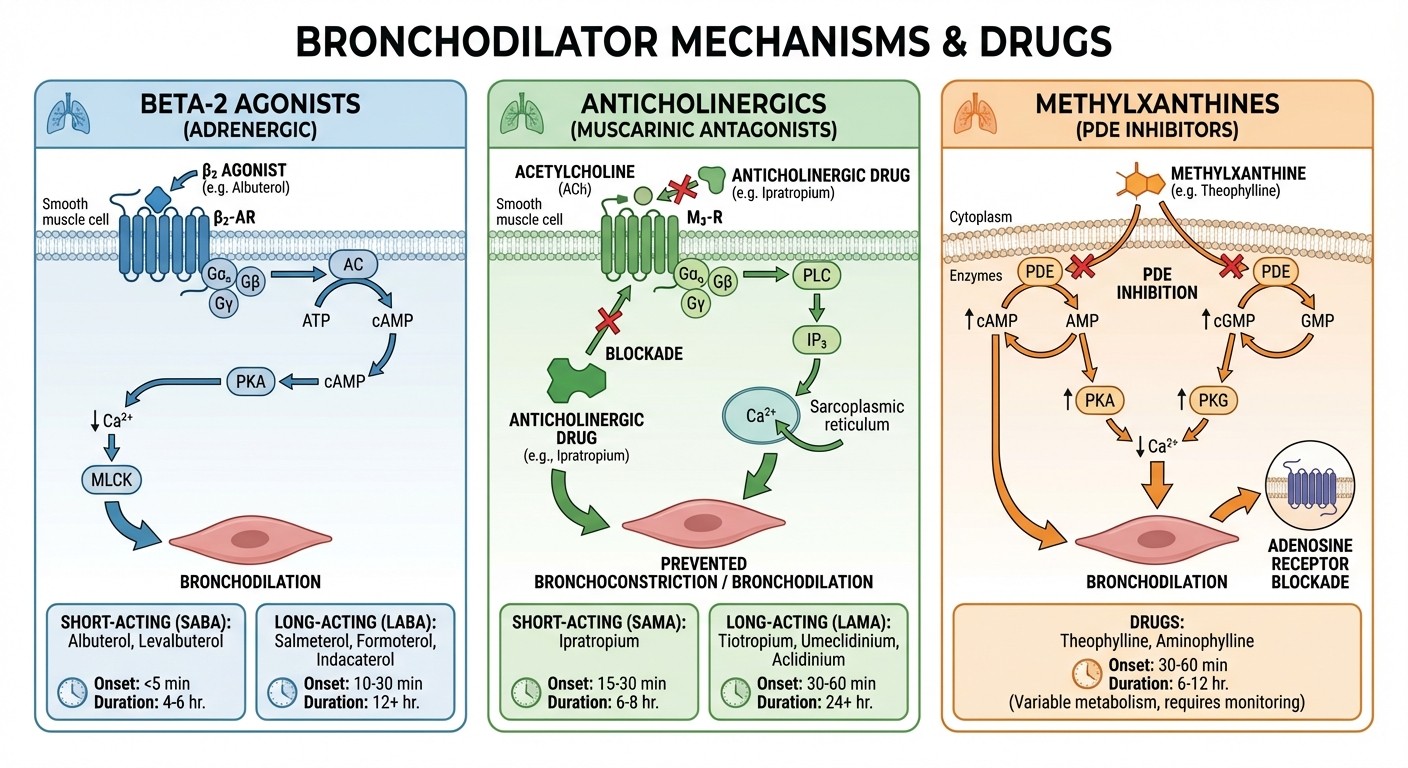
Beta-2 Adrenergic Agonists (Bronchodilators)
The most tested drug class in respiratory pharmacology. NEET PG loves asking about onset time, duration, and selectivity.
Short-Acting Beta-2 Agonists (SABA)
Salbutamol (Albuterol)
MOA: Selective beta-2 receptor agonist → increased cAMP → bronchodilation
Onset: 5 minutes (inhaled), 15-30 minutes (oral)
Duration: 4-6 hours
Clinical use: Acute bronchospasm, status asthmaticus (first-line), exercise-induced asthma
Side effects: Tremor, tachycardia, hypokalemia
Exam point: Drug of choice for acute asthma attack
Terbutaline
MOA: Beta-2 selective agonist with mild beta-1 activity
Route: SC, inhaled, oral
Duration: 4-6 hours
Clinical use: Status asthmaticus when inhaled route not possible
Side effects: More cardiac effects than salbutamol
Exam point: Can be given subcutaneously in emergency
Long-Acting Beta-2 Agonists (LABA)
Salmeterol
MOA: Beta-2 agonist with lipophilic side chain → prolonged receptor binding
Onset: 20 minutes (slow)
Duration: 12 hours
Clinical use: Maintenance therapy (never alone), COPD
Side effects: Same as SABA but longer-lasting
Exam point: Black box warning — increased asthma-related deaths when used without corticosteroids
The Oncourse mnemonic engine generates memorable hooks like "SALBS: Short Acting = Salbutamol, Terbutaline; Long Acting = Salmeterol, Formoterol" — making drug classification instant recall rather than rote memorization. Formoterol
MOA: Beta-2 agonist with rapid onset and long duration
Onset: 5 minutes (fast like SABA)
Duration: 12 hours
Clinical use: Maintenance + rescue therapy, COPD
Side effects: Similar to other LABAs
Exam point: Only LABA suitable for rescue use due to rapid onset
Methylxanthines
High-yield for mechanism questions and drug interactions.
Theophylline
MOA: Non-selective phosphodiesterase inhibition → increased cAMP + adenosine receptor antagonism
Therapeutic range: 10-20 μg/mL (narrow therapeutic index)
Clinical use: Second-line for asthma, COPD maintenance
Side effects: CNS stimulation, cardiac arrhythmias, GI upset
Drug interactions: CYP1A2 substrate (smoking decreases levels, ciprofloxacin increases)
Exam point: Requires monitoring due to narrow therapeutic window
Aminophylline
MOA: Theophylline + ethylenediamine (better solubility)
Route: IV (for status asthmaticus)
Clinical use: Severe acute asthma when beta-agonists fail
Exam point: IV form of theophylline for emergency use
For tricky concepts like theophylline's drug interactions, Synapses flashcards use spaced repetition to surface these facts at optimal intervals before your exam — no more cramming the night before.
Anticholinergics (Muscarinic Antagonists)
NEET PG frequently tests the difference between short and long-acting anticholinergics.
Ipratropium
MOA: M3 muscarinic receptor antagonist → reduced acetylcholine-induced bronchoconstriction
Onset: 15-30 minutes
Duration: 4-6 hours
Clinical use: COPD (first-line), asthma (second-line)
Side effects: Dry mouth, minimal systemic absorption
Exam point: Preferred in COPD over beta-agonists
Tiotropium
MOA: Long-acting M3 antagonist with kinetic selectivity
Onset: 30 minutes
Duration: 24 hours
Clinical use: COPD maintenance (once daily)
Side effects: Dry mouth, constipation
Exam point: First-line maintenance therapy for COPD
Glycopyrrolate
MOA: Long-acting anticholinergic
Duration: 12-24 hours
Route: Inhaled, injection
Clinical use: COPD maintenance therapy
Exam point: Alternative to tiotropium
Inhaled Corticosteroids (ICS)
Essential for maintenance therapy questions and side effect profiles.
Budesonide
MOA: Glucocorticoid receptor agonist → anti-inflammatory gene transcription
Bioavailability: Low systemic (high first-pass metabolism)
Clinical use: Asthma maintenance, COPD with frequent exacerbations
Side effects: Local — thrush, hoarseness; Systemic — growth retardation (children)
Exam point: Preferred in pregnancy and children
Fluticasone
MOA: High-potency corticosteroid with minimal systemic activity
Formulations: Propionate (twice daily), furoate (once daily)
Clinical use: Asthma maintenance, often combined with LABA
Side effects: Similar to budesonide but higher potency
Exam point: Available in combination with salmeterol
Beclomethasone
MOA: Corticosteroid prodrug activated in lungs
Clinical use: Asthma maintenance therapy
Side effects: Higher systemic absorption than newer agents
Exam point: Older agent, less commonly used now
Anti-Inflammatory Agents
Mast Cell Stabilizers Sodium Cromoglycate
MOA: Mast cell membrane stabilization → prevents histamine release
Clinical use: Prophylaxis (not acute treatment), exercise-induced asthma
Route: Inhaled only
Side effects: Minimal (cough, throat irritation)
Exam point: Prophylactic only — no use in acute attack
Nedocromil
MOA: Similar to cromoglycate but more potent
Clinical use: Asthma prophylaxis, allergic conjunctivitis
Side effects: Bitter taste, headache
Exam point: Second-generation mast cell stabilizer
Leukotriene Modifiers
High-yield for asthma pathophysiology and drug classification.
Montelukast
MOA: Leukotriene D4 (LTD4) receptor antagonist
Clinical use: Asthma maintenance, allergic rhinitis, exercise-induced asthma
Route: Oral (convenient for children)
Side effects: Behavioral changes, suicidal ideation (rare)
Exam point: Alternative to ICS in mild asthma
Zafirlukast
MOA: LTD4 receptor antagonist
Clinical use: Similar to montelukast
Drug interactions: CYP2C9 substrate
Side effects: Hepatotoxicity (rare)
Exam point: Requires liver function monitoring
Zileuton
MOA: 5-lipoxygenase inhibitor → blocks leukotriene synthesis
Clinical use: Asthma with aspirin sensitivity
Side effects: Hepatotoxicity, drug interactions (CYP1A2 inhibitor)
Exam point: Only leukotriene synthesis inhibitor (others are receptor antagonists)
When practicing MCQs about leukotriene pathways, the AI explanation chat breaks down why zileuton blocks synthesis while montelukast blocks receptors — turning confusion into clarity at the question level.
Antitussives
Frequently tested for mechanism and central vs peripheral action.
Codeine
MOA: Opioid μ-receptor agonist in medulla cough center
Clinical use: Dry cough suppression
Side effects: Sedation, constipation, respiratory depression
Contraindications: Children <12 years, CYP2D6 poor metabolizers
Exam point: Central antitussive with addiction potential
Dextromethorphan
MOA: NMDA receptor antagonist + sigma receptor → cough suppression
Clinical use: Non-prescription dry cough relief
Side effects: Minimal at therapeutic doses, abuse potential at high doses
Exam point: Non-opioid central antitussive
Noscapine (Pholcodine)
MOA: Central cough suppression without respiratory depression
Clinical use: Dry cough in patients where opioids contraindicated
Side effects: Minimal sedation, no addiction
Exam point: Non-opioid antitussive with better safety profile
Expectorants and Mucolytics
Important for differentiating mechanism of action.
Ambroxol
MOA: Increases surfactant production + mucociliary clearance
Clinical use: Productive cough, COPD with thick secretions
Route: Oral, injection
Side effects: GI upset, rash
Exam point: Metabolite of bromhexine
Bromhexine
MOA: Mucus depolymerization + increased serous secretion
Clinical use: Thick, tenacious sputum
Metabolism: Converted to ambroxol (active metabolite)
Exam point: Prodrug for ambroxol
Acetylcysteine
MOA: Breaks disulfide bonds in mucus → reduced viscosity
Clinical use: Cystic fibrosis, COPD, paracetamol poisoning antidote
Route: Inhaled, oral, IV
Side effects: Bronchospasm (with inhalation), nausea
Exam point: Dual use as mucolytic and antidote
Guaifenesin
MOA: Increases respiratory tract secretions → easier expectoration
Clinical use: Dry to productive cough conversion
Side effects: Nausea, vomiting at high doses
Exam point: Most common OTC expectorant
Anti-Asthma Biologics
Emerging area with increasing exam importance.
Omalizumab
MOA: Anti-IgE monoclonal antibody
Clinical use: Severe allergic asthma with elevated IgE
Route: Subcutaneous injection
Side effects: Injection site reactions, anaphylaxis risk
Exam point: First biologic for asthma
Mepolizumab
MOA: Anti-IL-5 monoclonal antibody → eosinophil reduction
Clinical use: Severe eosinophilic asthma
Route: Subcutaneous injection
Exam point: Targets eosinophil-driven inflammation
High-Yield Exam Patterns
Status Asthmaticus Management
1. First-line: High-dose salbutamol (nebulized) + systemic corticosteroids 2. Second-line: Ipratropium + salbutamol combination 3. Third-line: IV aminophylline or magnesium sulfate 4. Last resort: IV salbutamol or mechanical ventilation
COPD vs Asthma First-Line Therapy
COPD: Tiotropium (LAMA) or combined LAMA/LABA
Asthma: ICS (budesonide/fluticasone) ± LABA for maintenance
Beta-Blocker Poisoning Bronchospasm
Drug of choice: Ipratropium (anticholinergic)
Avoid: Beta-agonists (competitive inhibition by beta-blockers)
Cough Reflex Center
Location: Medulla oblongata
Central antitussives: Codeine, dextromethorphan, noscapine
Mechanism: μ-opioid receptor agonism (codeine) vs NMDA antagonism (dextromethorphan)
Drug Interaction Quick Reference
Drug | Major Interactions | Clinical Significance |
|---|---|---|
Theophylline | Ciprofloxacin ↑ levels, Smoking ↓ levels | Narrow therapeutic index |
Beta-agonists | Beta-blockers (antagonism) | Complete functional antagonism |
Zileuton | Warfarin, theophylline | CYP1A2 inhibition |
LABAs | Never use alone in asthma | FDA black box warning |
For complex interactions like these, targeted flashcards ensure you recall the mechanism behind each interaction — not just memorizing lists.
Frequently Asked Questions
Which bronchodilator has the fastest onset of action?
Salbutamol and formoterol both have 5-minute onset when inhaled. Salmeterol takes 20 minutes despite being long-acting.
What's the difference between theophylline and aminophylline?
Aminophylline is theophylline + ethylenediamine for better water solubility. It's used IV in emergencies. Theophylline is oral maintenance therapy.
Why cant LABAs be used alone in asthma?
LABAs can mask worsening inflammation while bronchodilating, leading to delayed recognition of severe exacerbations. Always combine with ICS.
Which antitussive is safest in children?
Dextromethorphan for children >4 years. Codeine is contraindicated under 12 years due to variable metabolism and respiratory depression risk.
What's first-line for exercise-induced asthma?
Short-acting beta-2 agonist (salbutamol) 15 minutes before exercise. Alternative: montelukast daily or cromoglycate before activity.
How do you remember anticholinergic duration?
"I-T rule": Ipratropium = short (4-6 hours), Tiotropium = long (24 hours). Both start with different letters for different durations.
Master respiratory pharmacology with the complete NEET PG pharmacology question bank and comprehensive lessons covering every high-yield drug. The systematic flashcard approach ensures nothing slips through the cracks during your final revision.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.