Back
NEET PG Cardiovascular Pharmacology Glossary 2026: Antihypertensives, Antiarrhythmics, Anti-Anginals and Heart Failure Drugs
Complete high-yield reference for NEET PG 2026 cardiovascular pharmacology. Master 47 essential drugs across antihypertensives, antiarrhythmics, anti-anginals and heart failure drugs with mechanisms, side effects and MCQ mnemonics.

NEET PG Cardiovascular Pharmacology Glossary 2026: Antihypertensives, Antiarrhythmics, Anti-Anginals and Heart Failure Drugs
You are staring at 47 cardiovascular drugs. The NEET PG paper has 200 questions, and 8-10 of them will be pure CVS pharmacology — antihypertensives, antiarrhythmics, heart failure drugs, and anti-anginals. You need mechanisms, side effects, contraindications, and drug interactions memorized cold.
This isnt another textbook chapter. Its a high-yield reference glossary built specifically for NEET PG 2026 and INICET — every drug mechanism explained in 2-3 lines, every side effect pattern condensed into mnemonics, every MCQ trap highlighted upfront. Cardiology accounts for 15-18% of your NEET PG score. Get the pharmacology right, and you have scored 30-35 marks before touching pathology or medicine.
The four major CVS drug classes — antihypertensives (ACE inhibitors, ARBs, calcium channel blockers, beta-blockers, diuretics), antiarrhythmics (Vaughan Williams Class I-IV), anti-anginals (nitrates, ranolazine, ivabradine), and heart failure drugs (digoxin, sacubitril-valsartan, aldosterone antagonists) — represent your highest-yield pharmacology topics. Master these 47 drugs and their 200+ testable facts, and cardiovascular pharmacology becomes your strength, not your weakness.
Antihypertensive Drugs: The Big Five Categories
ACE Inhibitors (The "-pril" Family)
Core Mechanism: Block angiotensin-converting enzyme → ↓ angiotensin II → ↓ aldosterone → vasodilation + ↓ sodium retention. Key Drugs: Lisinopril, enalapril, captopril, ramipril, perindopril High-Yield Facts:
Captopril: First ACE inhibitor, shortest half-life (8 hours), contains sulfhydryl group
Lisinopril: Longest half-life (24 hours), doesnt require hepatic activation
Enalapril: Prodrug, requires conversion to enalaprilat
Side Effects Mnemonic - "ACE CHOP":
Angioedema (0.1-0.5%, higher in blacks)
Cough (dry, nonproductive, 10-15%)
Elevated potassium (hyperkalemia)
Creatinine rise (reversible azotemia)
Hypotension (first-dose effect)
Oliguria (in bilateral renal artery stenosis)
Pregnancy contraindicated (teratogenic)
MCQ Traps:
Angioedema is NOT dose-dependent and can occur years after starting therapy
ACE inhibitors are protective in diabetic nephropathy even without hypertension
Contraindicated in bilateral renal artery stenosis (causes acute kidney injury)
For deeper understanding of ACE inhibitor mechanisms and clinical applications, explore NEET PG cardiovascular pharmacology lessons.
Angiotensin Receptor Blockers (ARBs - The "-sartan" Family)
Core Mechanism: Block angiotensin II at AT1 receptors → same effects as ACE inhibitors but no bradykinin accumulation. Key Drugs: Losartan, valsartan, telmisartan, olmesartan, irbesartan High-Yield Facts:
Losartan: Active metabolite E-3174, also blocks uric acid reabsorption
Telmisartan: Longest half-life (24 hours), PPAR-γ agonist activity
Valsartan: Component of sacubitril-valsartan (Entresto)
Side Effects: Similar to ACE inhibitors BUT NO COUGH, NO ANGIOEDEMA Clinical Pearl: ARBs are first choice when ACE inhibitors cause cough (10% of patients). When drilling cardiovascular pharmacology MCQs, Oncourse's adaptive question bank automatically increases ARB mechanism questions if you miss them repeatedly, closing gaps faster than random revision.
Beta-Blockers: Selective vs Non-Selective
Core Mechanism: Block β-adrenergic receptors → ↓ heart rate + ↓ contractility + ↓ renin release.
#### Non-Selective Beta-Blockers (β1 + β2)
Drugs: Propranolol, nadolol, timolol
Propranolol: Prototype, lipophilic, crosses BBB, has membrane-stabilizing activity
Nadolol: Hydrophilic, long half-life, no hepatic metabolism
#### Cardioselective Beta-Blockers (β1 > β2)
Drugs: Metoprolol, atenolol, bisoprolol, nebivolol
Atenolol: Hydrophilic, renal elimination
Metoprolol: Lipophilic, hepatic metabolism
Nebivolol: Additional NO-mediated vasodilation
#### Beta-Blockers with α-Blocking Activity
Drugs: Labetalol (α1 + β), carvedilol (α1 + β + antioxidant)
Side Effects Mnemonic - "BETA BLOCK":
Bronchospasm (avoid in asthma)
Erectile dysfunction
Tiredness/fatigue
AV conduction blocks
Bradycardia
Lipid profile worsening (↑ TG, ↓ HDL)
Overall mask hypoglycemia symptoms
Cold extremities
Kontraindicated in cocaine toxicity (unopposed α-stimulation)
MCQ Traps:
ISA (Intrinsic Sympathomimetic Activity): Pindolol, acebutolol — less bradycardia, less lipid changes
Beta-blockers without ISA preferred post-MI for mortality benefit
Calcium Channel Blockers: Three Distinct Classes
Core Mechanism: Block L-type calcium channels → vasodilation and/or ↓ cardiac contractility/conduction.
#### Dihydropyridines (The "-pine" Family)
Drugs: Nifedipine, amlodipine, felodipine, nicardipine
Mechanism: Selective vascular calcium channel blockade
Effects: Peripheral vasodilation, no cardiac depression
Amlodipine: Longest half-life (30-50 hours), least negative inotropic effect
#### Non-Dihydropyridines
Verapamil (Phenylalkylamine):
Negative inotrope + negative chronotrope + negative dromotrope
Constipation (most common side effect)
Strong CYP3A4 inhibitor
Diltiazem (Benzothiazepine):
Intermediate between verapamil and dihydropyridines
Less constipation than verapamil
Less peripheral edema than dihydropyridines
Side Effects by Class:
Dihydropyridines: Peripheral edema (not heart failure), flushing, reflex tachycardia
Verapamil: Constipation (most common), AV block, negative inotropy
Diltiazem: AV block, negative inotropy (less than verapamil)
The "ABCD" mnemonic for heart failure drugs (ACE inhibitors, Beta-blockers, CCBs avoided, Diuretics) has visual mnemonics available in Oncourse flashcard decks — students can move from reading this glossary to active recall in one tap.
Diuretics in Hypertension
#### Thiazide and Thiazide-Like Diuretics
Drugs: Hydrochlorothiazide (HCTZ), chlorthalidone, indapamide
Mechanism: Block Na-Cl cotransporter in distal convoluted tubule
Chlorthalidone vs HCTZ:
Chlorthalidone: Longer half-life (24-72 hours), better cardiovascular outcomes in trials
HCTZ: Shorter half-life (6-12 hours), more commonly used
Side Effects - "THIAZIDE HIT":
Thrombocytopenia
Hyponatremia
Impotence
Alkalosis (metabolic)
Zinc deficiency (rare)
Increased glucose
Decreased potassium
Elevated uric acid
Hypercalcemia
Increased cholesterol
Tinnitus (high doses)
#### Loop Diuretics in HTN
Limited Role: Only in hypertension with fluid overload Drug: Furosemide Major Concern: Ototoxicity (especially with aminoglycosides)
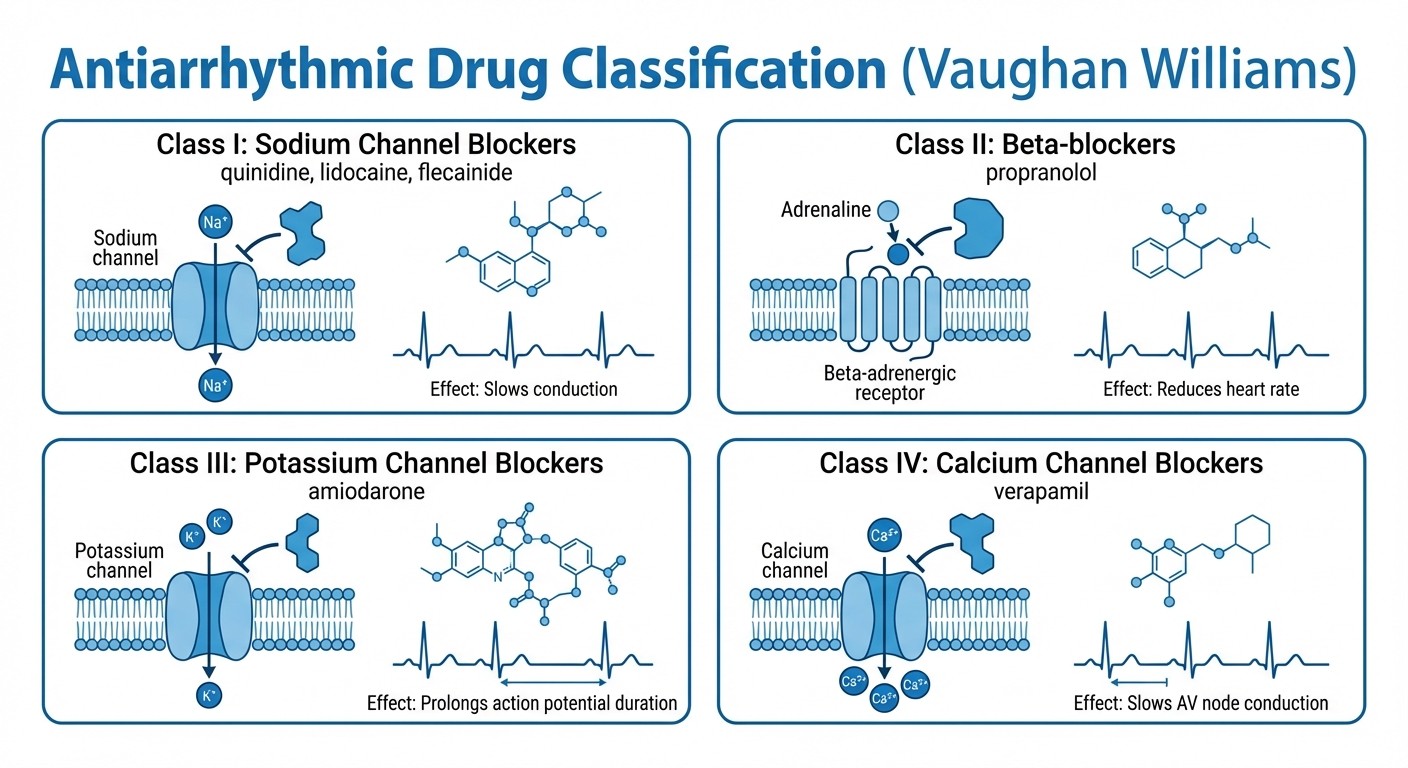
Antiarrhythmic Drugs: Vaughan Williams Classification
Class I: Sodium Channel Blockers
Core Mechanism: Block fast Na+ channels → ↓ phase 0 depolarization → ↓ conduction velocity.
#### Class IA: Intermediate Kinetics
Drugs: Quinidine, procainamide, disopyramide
Quinidine: Prototype, antimalarial activity, cinchonism
Procainamide: Lupus-like syndrome (slow acetylators), NAPA metabolite
Disopyramide: Strong negative inotrope, anticholinergic effects
Effects: ↓ conduction velocity, ↑ refractory period, ↓ contractility
#### Class IB: Fast Kinetics
Drugs: Lidocaine, mexiletine, phenytoin
Lidocaine: IV only, hepatic metabolism, CNS toxicity
Mexiletine: Oral lidocaine analog
Phenytoin: Antiepileptic with antiarrhythmic properties
Effects: Minimal effect on normal tissue, preferentially blocks ischemic/depolarized cells
#### Class IC: Slow Kinetics
Drugs: Flecainide, propafenone
Flecainide: Most potent Na+ channel blocker, avoid in structural heart disease
Propafenone: Weak β-blocking activity
CAST Study Warning: Class IC drugs increase mortality in post-MI patients with structural heart disease.
Class II: Beta-Blockers
Mechanism: Block β1 receptors → ↓ SA node firing, ↓ AV conduction, ↓ contractility Key Drugs: Propranolol, metoprolol, esmolol Esmolol: Ultra-short acting (half-life 9 minutes), IV only, metabolized by RBC esterases
Class III: Potassium Channel Blockers
Core Mechanism: Block K+ channels → ↑ action potential duration → ↑ refractory period. Amiodarone:
Unique Properties: Contains iodine (37% by weight), affects all four Vaughan Williams classes
Tissue Accumulation: Half-life 20-100 days, takes months to reach steady state
Side Effects: Pulmonary fibrosis (most serious), thyroid dysfunction, hepatotoxicity, corneal deposits, blue-gray skin
Dronedarone:
"Safer Amiodarone": No iodine, shorter half-life
Major Limitation: Contraindicated in permanent AF and heart failure
Sotalol:
Dual Action: β-blocker + Class III activity
Torsades Risk: Dose-related, worse in hypokalemia
Ibutilide & Dofetilide:
Use: Acute AF/flutter conversion
Risk: High torsades potential, requires inpatient monitoring
Class IV: Calcium Channel Blockers
Drugs: Verapamil, diltiazem Mechanism: Block L-type Ca2+ channels → ↓ SA node automaticity, ↓ AV conduction Use: Supraventricular arrhythmias (NOT ventricular) Drug-Drug Interaction Pearl: Verapamil + digoxin = doubled digoxin levels.
CVS pharmacology is flagged as a high-priority topic cluster in Oncourse's High-Yield Topic Tracker — it shows exactly how many CVS pharma questions you have attempted, your accuracy trend, and recommends your next study path (e.g., antiarrhythmics → ECG interpretation → related clinical scenarios).
Anti-Anginal Agents
Nitrates: NO Donors
Core Mechanism: Release nitric oxide → cGMP ↑ → smooth muscle relaxation → venous > arterial dilation. Nitroglycerin (GTN):
Routes: Sublingual, IV, transdermal patches, oral sustained-release
Onset: Sublingual 1-3 minutes, patch 30-60 minutes
Duration: Sublingual 10-30 minutes, patch 8-12 hours
Isosorbide Dinitrate (ISDN):
Bioavailability: 25% (extensive first-pass metabolism)
Duration: 4-6 hours
Active Metabolites: Isosorbide-2-mononitrate, isosorbide-5-mononitrate
Isosorbide Mononitrate (ISMN):
Advantage: 100% bioavailability (no first-pass metabolism)
Duration: 6-8 hours
Dosing: Asymmetric (8 AM, 2 PM) to prevent tolerance
Side Effects:
Headache: Most common, related to cerebral vasodilation
Hypotension: Especially orthostatic
Reflex Tachycardia: Compensatory response
Methemoglobinemia: Rare, with high doses
Tolerance: Develops within 24-48 hours of continuous exposure Prevention: Nitrate-free interval (10-12 hours daily)
Ranolazine: Late Sodium Channel Blocker
Mechanism: Selective inhibition of late INa → ↓ intracellular Na+ → ↓ Ca2+ overload → ↓ diastolic tension. Clinical Use: Chronic stable angina when first-line therapy inadequate Unique Feature: Anti-anginal without affecting heart rate or blood pressure Major Drug Interaction: CYP3A4 substrate, levels doubled by ketoconazole QT Prolongation: Dose-related, but rarely causes torsades
Ivabradine: If Channel Blocker
Mechanism: Selective If channel blockade in SA node → ↓ heart rate WITHOUT affecting contractility. Clinical Uses:
Chronic stable angina (when β-blockers contraindicated)
Heart failure with reduced ejection fraction (EF ≤35%) + sinus rhythm + HR ≥70 bpm
Side Effects: Luminous phenomena (phosphenes) — 15% of patients report visual brightness Contraindications: Atrial fibrillation (no effect on irregularly irregular rhythm)
Heart Failure Drugs
ACE Inhibitors and ARBs in Heart Failure
Mortality Benefit: Both classes reduce mortality in heart failure with reduced ejection fraction (HFrEF). Target Doses:
Lisinopril: 20-40 mg daily
Enalapril: 10-20 mg twice daily
Losartan: 50-150 mg daily
Beta-Blockers in Heart Failure
Evidence-Based Choices: Only three β-blockers have proven mortality benefit in HFrEF:
Metoprolol Succinate: Extended-release only
Carvedilol: α + β blocker
Bisoprolol: Highly β1-selective
Contraindications in Acute HF: Never start β-blockers during acute decompensated heart failure.
Aldosterone Receptor Antagonists
Spironolactone:
Mortality Benefit: RALES trial, severe heart failure
Side Effects: Gynecomastia (dose-related), hyperkalemia
Monitoring: Potassium and creatinine at 1 week, 1 month, 3 months
Eplerenone:
Advantages: No gynecomastia, more selective for mineralocorticoid receptor
Cost: Significantly more expensive than spironolactone
Evidence: EMPHASIS-HF trial, mild-moderate heart failure
Digoxin: The Cardiac Glycoside
Mechanism:
Positive Inotrope: Na+/K+-ATPase inhibition → ↑ intracellular Ca2+
Negative Chronotrope: Enhanced vagal tone → ↓ SA node firing + ↓ AV conduction
Pharmacokinetics:
Half-Life: 36 hours (normal kidney function)
Elimination: 85% renal, 15% hepatic
Loading Dose: 8-12 mcg/kg (lean body weight)
Therapeutic Range: 0.5-2.0 ng/mL (some prefer 0.5-1.0 ng/mL for heart failure) Digoxin Toxicity Signs:
Early: Nausea, vomiting, anorexia, visual disturbances (yellow halos)
Cardiac: Any arrhythmia except rapid AF, bidirectional VT (pathognomonic)
Treatment: Digoxin-specific antibodies (Digibind), correct electrolytes
Drug Interactions:
↑ Digoxin Levels: Amiodarone, verapamil, quinidine, erythromycin
↓ Digoxin Levels: Cholestyramine, sucralfate, antacids
Sacubitril-Valsartan (ARNI)
Mechanism:
Sacubitril: Neprilysin inhibitor → ↑ natriuretic peptides (ANP, BNP)
Valsartan: ARB component
Evidence: PARADIGM-HF trial showed 20% reduction in cardiovascular death vs enalapril Washout Period: Stop ACE inhibitors 36 hours before starting (angioedema risk) Contraindications: History of angioedema with ACE inhibitors/ARBs
Newer Heart Failure Therapies
SGLT2 Inhibitors in Heart Failure:
Mechanism: Sodium-glucose cotransporter 2 inhibition
Benefits: Reduce heart failure hospitalizations even in non-diabetics
Key Drugs: Dapagliflozin, empagliflozin
Side Effects: Genital fungal infections, DKA risk
Ivabradine in Heart Failure:
Indication: HFrEF with EF ≤35%, sinus rhythm, HR ≥70 bpm despite optimal β-blocker
Benefit: Reduces heart failure hospitalizations
Contraindications: Atrial fibrillation, severe hepatic impairment
Quick Reference Drug Tables
ACE Inhibitor | Half-Life | Key Feature |
|---|---|---|
Captopril | 2 hours | Sulfhydryl group, shortest acting |
Enalapril | 11 hours | Prodrug |
Lisinopril | 12 hours | No hepatic activation needed |
Ramipril | 13-17 hours | Strong tissue ACE binding |
Antiarrhythmic Class | Mechanism | Prototype Drug | Major Toxicity |
|---|---|---|---|
IA | ↓ Na+, ↑ APD | Quinidine | Torsades de pointes |
IB | ↓ Na+, ↓ APD | Lidocaine | CNS toxicity |
IC | ↓ Na+ (slow) | Flecainide | Proarrhythmia |
II | β-blockade | Propranolol | Bradycardia, bronchospasm |
III | ↓ K+ efflux | Amiodarone | Pulmonary fibrosis |
IV | ↓ Ca2+ | Verapamil | AV block |
High-Yield MCQ Patterns and Traps
Antihypertensive MCQ Traps
1. "Best initial therapy for diabetic with hypertension" → ACE inhibitor (renal protection) 2. "Hypertension with asthma" → Avoid β-blockers (even cardioselective) 3. "Bilateral renal artery stenosis" → Avoid ACE inhibitors and ARBs 4. "African American with hypertension" → Thiazides or CCBs (ACE inhibitors less effective)
Antiarrhythmic MCQ Traps
1. "Post-MI patient with VT" → Avoid Class IC drugs (CAST study) 2. "Amiodarone + warfarin" → Monitor INR closely (amiodarone inhibits warfarin metabolism) 3. "WPW with AF" → Avoid digoxin, verapamil, diltiazem (can facilitate conduction down accessory pathway) 4. "Torsades de pointes treatment" → IV magnesium + correct electrolytes
Heart Failure MCQ Traps
1. "Acute decompensated heart failure" → Never start β-blockers 2. "Digoxin toxicity with normal levels" → Check potassium (hypokalemia increases toxicity) 3. "Best mortality benefit in heart failure" → ACE inhibitors (not digoxin) 4. "Spironolactone monitoring" → Potassium and creatinine (hyperkalemia risk)
Contraindications Quick Reference
Absolute Contraindications
ACE Inhibitors/ARBs:
Bilateral renal artery stenosis
Pregnancy
History of angioedema
Beta-Blockers:
Severe asthma/COPD
2nd/3rd degree AV block (without pacemaker)
Cardiogenic shock
Calcium Channel Blockers:
Verapamil/Diltiazem: Severe heart failure, 2nd/3rd degree AV block
Dihydropyridines: Severe aortic stenosis
Digoxin:
2nd/3rd degree AV block
Ventricular tachycardia/fibrillation
Hypertrophic cardiomyopathy with outflow obstruction
Pharmacology mastery comes from pattern recognition. Use Synapses visual mnemonics to lock in drug mechanisms — the "ABCD" heart failure drugs, the "ACE CHOP" side effects, and Vaughan Williams classifications become automatic recall, not forced memorization.
Drug Interactions: High-Yield for NEET PG
CYP450 Interactions
Strong CYP3A4 Inhibitors: Amiodarone, verapamil, diltiazem
Effect: Increase levels of: simvastatin, digoxin, warfarin
P-glycoprotein Interactions:
Inhibitors: Amiodarone, verapamil, quinidine
Substrate: Digoxin
Result: Increased digoxin toxicity risk
Clinically Significant Combinations
1. Amiodarone + Warfarin → ↑ INR (inhibits warfarin metabolism) 2. Verapamil + Digoxin → ↑ digoxin levels (P-gp inhibition) 3. ACE Inhibitor + K+-sparing Diuretic → Hyperkalemia risk 4. β-blocker + Verapamil/Diltiazem → Severe bradycardia/AV block
Electrolyte-Drug Interactions
Hypokalemia → ↑ digoxin toxicity, ↑ QT prolongation with Class III drugs
Hypomagnesemia → ↑ torsades risk with any QT-prolonging drug
Hypercalcemia → ↑ digoxin toxicity
Frequently Asked Questions
Which antihypertensive is best for diabetic nephropathy?
ACE inhibitors or ARBs provide renal protection independent of blood pressure lowering. They reduce proteinuria and slow progression to end-stage renal disease. Start with ACE inhibitor; switch to ARB if cough develops.
Why is amiodarone contraindicated in pregnancy?
Amiodarone contains 37% iodine by weight, which can cause fetal thyroid dysfunction, growth retardation, and developmental abnormalities. The drug accumulates in fetal tissues and has a very long elimination half-life.
When should you avoid beta-blockers in heart failure?
Never start β-blockers during acute decompensated heart failure. Only initiate when patient is stable and euvolemic. Start low (e.g., carvedilol 3.125 mg twice daily) and titrate slowly over weeks to months.
What makes Class IC antiarrhythmics dangerous post-MI?
The CAST study showed increased mortality with flecainide and encainide in post-MI patients. These drugs have slow dissociation kinetics from sodium channels, creating proarrhythmic effects especially in ischemic myocardium.
How do you differentiate digoxin toxicity from heart failure symptoms?
Digoxin toxicity presents with GI symptoms (nausea, vomiting, anorexia) and visual disturbances (yellow/green halos) before cardiac manifestations. Heart failure typically causes dyspnea and edema without GI or visual symptoms.
Why is there a washout period before starting sacubitril-valsartan?
Both ACE inhibitors and neprilysin inhibition can increase bradykinin levels. Concurrent use significantly increases angioedema risk. The 36-hour washout allows ACE inhibitor levels to decline before starting the combination therapy.
Master Your CVS Pharmacology
You now have 47 cardiovascular drugs mapped with mechanisms, side effects, contraindications, and MCQ traps. The NEET PG 2026 cardiovascular pharmacology questions are testing pattern recognition — can you spot the hypokalemic patient with digoxin toxicity, the asthmatic who needs CCBs instead of β-blockers, or the post-MI patient who shouldnt get Class IC drugs?
Focus your next 2-3 study sessions on drug interactions and contraindications. These account for 40% of cardiovascular pharmacology MCQs but are often overlooked during mechanism memorization.
Practice with targeted MCQs to drill these patterns. Convert your reading knowledge into exam performance through active recall and spaced repetition. The difference between knowing enalapril is an ACE inhibitor and recognizing why it shouldnt be given to a patient with bilateral renal artery stenosis is what separates average scores from top percentile ranks.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.