Back
Which Bone Tumors Occur in Maffucci Syndrome? Explained Simply for Medical Students 2026
Complete guide to bone tumors in Maffucci syndrome: enchondromas, chondrosarcoma transformation, diagnosis & management. Essential for NEET-PG, USMLE prep.

Which Bone Tumors Occur in Maffucci Syndrome? Explained Simply for Medical Students 2026
Maffucci syndrome is a rare genetic disorder that significantly increases the risk of developing multiple bone tumors. Understanding the types of bone tumors associated with this condition is crucial for medical students preparing for NEET-PG, USMLE, and other medical examinations. This comprehensive guide breaks down everything you need to know about bone tumors in Maffucci syndrome.
What is Maffucci Syndrome?
Maffucci syndrome is a rare mesodermal disorder characterized by the presence of multiple enchondromas (benign cartilage tumors) and soft tissue hemangiomas. First described by Angelo Maffucci in 1881, this condition affects approximately 1 in 1 million people worldwide.
The syndrome is caused by somatic mutations in the IDH1 or IDH2 genes, which occur during early embryonic development. These mutations lead to the formation of multiple benign bone tumors, but more importantly, create a significant risk for malignant transformation.
Key Clinical Features of Maffucci Syndrome
Multiple enchondromas affecting long bones
Soft tissue hemangiomas
Asymmetric limb growth
Pathological fractures
High risk of malignant transformation (15-30%)
Primary Bone Tumors in Maffucci Syndrome
1. Enchondromas (Most Common)
Enchondromas are the hallmark bone tumors of Maffucci syndrome. These benign cartilage tumors develop within the medullary cavity of bones and are responsible for most of the clinical manifestations.
Characteristics of Enchondromas in Maffucci Syndrome:
Location: Primarily affect long bones (femur, tibia, humerus, radius, ulna)
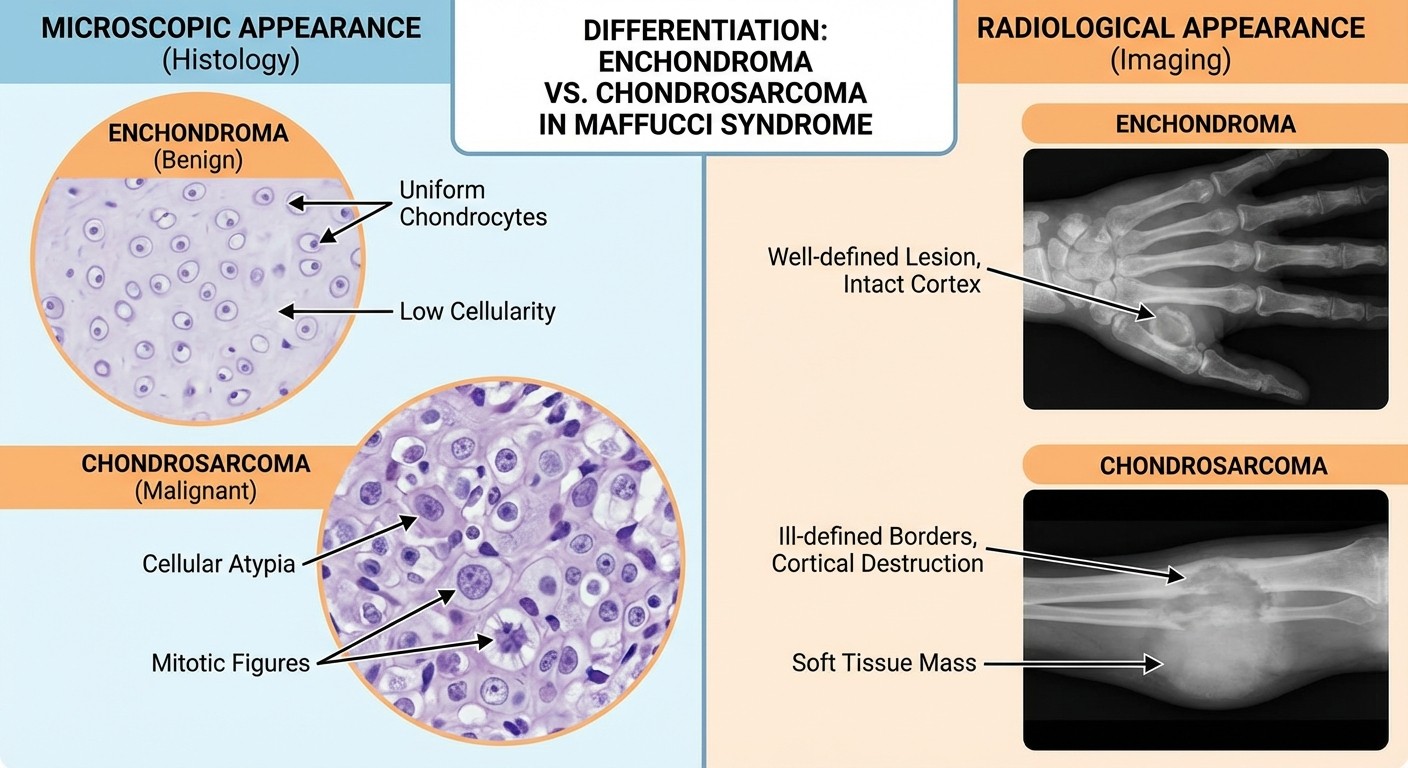
Radiological appearance: Well-defined lytic lesions with calcifications
Histology: Mature hyaline cartilage with lobular architecture
Growth pattern: Slow-growing, usually asymptomatic unless causing fractures
Clinical Significance:
Enchondromas in Maffucci syndrome differ from solitary enchondromas in their:
Higher number (multiple lesions)
Increased risk of malignant transformation
Association with soft tissue hemangiomas
Tendency to cause limb deformities
2. Chondrosarcomas (Malignant Transformation)
The most concerning aspect of Maffucci syndrome is the high risk of malignant transformation of enchondromas into chondrosarcomas. This occurs in 15-30% of patients, making regular monitoring essential.
Warning Signs of Malignant Transformation:
Clinical Feature | Benign Enchondroma | Malignant Chondrosarcoma |
|---|---|---|
Pain | Usually painless | Progressive, increasing pain |
Growth | Stable or slow growth | Rapid enlargement |
Cortical involvement | Intact cortex | Cortical destruction |
Soft tissue extension | Absent | May be present |
Age of transformation | - | Usually after age 40 |
Types of Chondrosarcoma in Maffucci Syndrome:
Grade I (Low-grade): Most common, slow-growing
Grade II (Intermediate): Moderate cellular atypia
Grade III (High-grade): Rare, aggressive behavior
Less Common Bone Tumors
3. Osteosarcomas
While rare, osteosarcomas can occasionally develop in patients with Maffucci syndrome. These malignant bone tumors typically arise in areas previously affected by enchondromas.
Characteristics:
More aggressive than chondrosarcomas
Higher metastatic potential
Require immediate aggressive treatment
Associated with worse prognosis
4. Fibrosarcomas
Fibrosarcomas represent another rare malignant transformation possibility in Maffucci syndrome patients. These tumors arise from fibrous connective tissue within or adjacent to bone lesions.
Diagnostic Approach to Bone Tumors in Maffucci Syndrome
Clinical Assessment
History Taking:
Family history (though most cases are sporadic)
Age of onset of symptoms
Pattern of tumor growth
Associated symptoms (pain, fractures, functional limitations)
Physical Examination:
Limb length discrepancy
Palpable masses
Range of motion assessment
Neurological examination if nerve compression suspected
Imaging Studies
Plain Radiographs:
First-line imaging modality
Shows characteristic "ring and arc" calcifications
Helps identify cortical integrity
Monitors for changes suggestive of malignant transformation
MRI (Magnetic Resonance Imaging):
Best for assessing soft tissue extension
Evaluates cortical destruction
Helps differentiate benign from malignant lesions
Essential for surgical planning
CT Scan:
Excellent for detecting calcifications
Assesses cortical involvement
Useful for biopsy guidance
Monitors treatment response
Laboratory Tests
While no specific laboratory tests diagnose Maffucci syndrome, certain markers may be helpful:
Alkaline phosphatase: May be elevated in malignant transformation
LDH (Lactate dehydrogenase): Can be increased in aggressive tumors
Genetic testing: IDH1/IDH2 mutation analysis (research purposes)
Malignant Transformation Risk Factors
Understanding the factors that increase malignant transformation risk is crucial for patient management:
High-Risk Features
1. Age: Risk increases significantly after age 40
2. Tumor location: Axial skeleton lesions have higher risk
3. Tumor size: Large enchondromas (>5 cm) are more concerning
4. Pain: New or increasing pain in a previously asymptomatic lesion
5. Growth: Any evidence of lesion enlargement in adults
Monitoring Protocol
Regular Follow-up Schedule:
Ages 0-18: Annual clinical and radiological assessment
Ages 18-40: Every 2 years if stable
Ages 40+: Annual monitoring due to increased malignancy risk
Any concerning changes: Immediate evaluation
Treatment Approaches
Management of Benign Enchondromas
Conservative Management:
Regular monitoring with imaging
Activity modification if fracture risk is high
Physical therapy for functional limitations
Pain management for symptomatic lesions
Surgical Intervention Indications:
Pathological fractures
Significant limb deformity
Functional impairment
Suspected malignant transformation
Large lesions threatening cortical integrity
Surgical Options:
Curettage and bone grafting
Prophylactic fixation for impending fractures
Limb reconstruction procedures
Corrective osteotomies for deformities
Management of Malignant Transformation
Chondrosarcoma Treatment:
Wide surgical resection with clear margins
Limb salvage procedures when feasible
Amputation for extensive or recurrent disease
Chemotherapy has limited effectiveness
Radiation therapy for inoperable cases
Multidisciplinary Approach:
Orthopedic oncologist
Medical oncologist
Radiation oncologist
Reconstructive surgeon
Pathologist
Genetic counselor
Prognosis and Long-term Outlook
Factors Affecting Prognosis
Benign Disease:
Generally good functional outcome with appropriate management
Quality of life may be affected by limb deformities
Risk of pathological fractures throughout life
Ongoing surveillance required
Malignant Transformation:
Grade I chondrosarcoma: 5-year survival >90%
Grade II chondrosarcoma: 5-year survival 70-80%
Grade III chondrosarcoma: 5-year survival <50%
Osteosarcoma: Variable, depends on stage and response to treatment
Complications to Monitor
1. Pathological fractures: Most common complication
2. Limb length discrepancy: Can cause functional impairment
3. Joint deformities: May require reconstructive surgery
4. Nerve compression: From large tumors
5. Malignant transformation: Requires immediate intervention
Study Tips for Medical Students
High-Yield Facts for Exams
Maffucci syndrome = Enchondromas + Hemangiomas
15-30% malignant transformation risk
IDH1/IDH2 mutations are the underlying cause
Chondrosarcoma is the most common malignant transformation
Regular monitoring is essential, especially after age 40
Common Exam Questions
1. What is the most common bone tumor in Maffucci syndrome?
Answer: Enchondroma
2. What percentage of patients develop malignant transformation?
Answer: 15-30%
3. Which genes are mutated in Maffucci syndrome?
Answer: IDH1 and IDH2
4. What is the most common type of malignant transformation?
Answer: Chondrosarcoma
5. At what age does malignant transformation risk significantly increase?
Answer: After age 40
Memory Aids
"MAFFUCCI" Mnemonic:
Multiple enchondromas
Asymmetric growth
Fractures (pathological)
Fibrous dysplasia (differential)
Uncommon syndrome
Chondrosarcoma risk
Calcifications on imaging
IDH mutations
Differential Diagnosis
Multiple Enchondromatosis (Ollier Disease)
Key differences from Maffucci syndrome:
No soft tissue hemangiomas in Ollier disease
Lower malignant transformation risk (5-25%)
Similar bone involvement pattern
Same genetic mutations (IDH1/IDH2)
Other Conditions to Consider
1. Hereditary Multiple Exostoses: External bone growths
2. McCune-Albright Syndrome: Fibrous dysplasia + café-au-lait spots
3. Neurofibromatosis Type 1: Neurofibromas + bone dysplasia
4. Metastatic Disease: In adults with multiple bone lesions
Clinical Case Study
Case Presentation:
A 35-year-old female presents with a 6-month history of increasing pain in her right femur. She has a known history of Maffucci syndrome with multiple enchondromas and cutaneous hemangiomas. Previous imaging showed stable enchondromas for the past 10 years.
Concerning Features:
New onset pain in a previously asymptomatic lesion
Patient approaching the high-risk age group for malignant transformation
Need for urgent re-evaluation
Management Approach:
1. Immediate MRI of the affected area
2. Comparison with previous imaging studies
3. Consider biopsy if imaging suggests malignant changes
4. Multidisciplinary team consultation
This case illustrates the importance of vigilant monitoring and prompt evaluation of any changes in patients with Maffucci syndrome.
Study Resources and Practice
For comprehensive understanding of bone tumors and genetic syndromes, medical students should utilize multiple learning modalities:
Essential Study Materials
Practice your knowledge with bone tumor questions to reinforce key concepts about Maffucci syndrome and related conditions.
Deepen your understanding through detailed bone and soft tissue pathology lessons that cover the histological and molecular aspects of these tumors.
Use bone tumor flashcards for quick revision and memorization of key facts about Maffucci syndrome and associated malignancies.
For orthopedic perspectives on bone tumors, explore orthopedics bone tumor lessons that focus on surgical management approaches.
Conclusion
Maffucci syndrome represents a complex genetic disorder with significant implications for bone tumor development. The primary bone tumors associated with this condition are enchondromas, which carry a substantial risk of malignant transformation to chondrosarcoma. Understanding the clinical features, diagnostic approaches, and management strategies is essential for medical students and healthcare providers.
Key takeaways include the importance of regular monitoring, recognition of warning signs for malignant transformation, and the need for a multidisciplinary approach to patient care. The 15-30% risk of malignant transformation makes Maffucci syndrome a high-stakes diagnosis requiring lifelong surveillance and prompt intervention when indicated.
For medical students preparing for examinations, focus on the association between IDH mutations, the clinical triad of multiple enchondromas and hemangiomas, and the critical age threshold of 40 years for increased malignancy risk. Regular practice with case-based questions and imaging interpretation will strengthen your understanding of this important rare disease syndrome.