INICET Musculoskeletal & Rheumatology Pharmacology Glossary 2026: NSAIDs, DMARDs, Anti-Gout Drugs and Biologics
Complete INICET rheumatology pharmacology guide covering NSAIDs, DMARDs, biologics, and anti-gout drugs. High-yield mechanisms, side effects, monitoring schedules, and MCQ mnemonics for exam success.
INICET Musculoskeletal & Rheumatology Pharmacology Glossary 2026: NSAIDs, DMARDs, Anti-Gout Drugs and Biologics
You are probably staring at another rheumatology pharmacology chapter wondering how to memorize 47 different drug mechanisms, 23 side effect profiles, and the contraindications for every DMARD without your brain melting. INICET loves testing the intricate details — methotrexate monitoring schedules, anti-TNF contraindications, and whether febuxostat or allopurinol causes more drug interactions.
This glossary cuts through the noise. Every drug class gets mechanism + high-yield side effects + MCQ traps that INICET actually tests. No fluff, no generic overviews. Just the exam-ready facts you need to distinguish between tocilizumab and tofacitinib when the clock is ticking.
The pattern is predictable: INICET asks about NSAIDs selectivity (COX-1 vs COX-2), DMARD toxicity monitoring (folate with methotrexate, ophthalmology with hydroxychloroquine), and biologics mechanisms (which targets TNF vs IL-6 vs JAK). Master these core concepts and the MCQs become pattern recognition instead of guesswork.
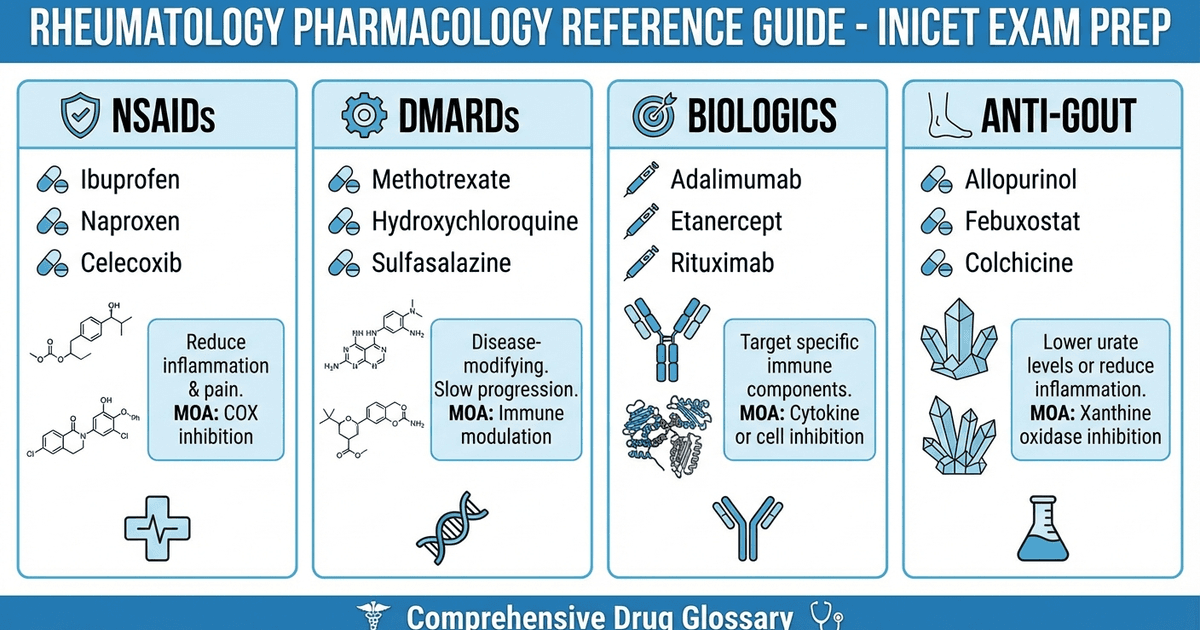
NSAIDs: COX Selectivity and Clinical Applications
Mechanism and Classification
NSAIDs work by inhibiting cyclooxygenase (COX) enzymes, blocking prostaglandin synthesis. INICET focuses heavily on COX-1 vs COX-2 selectivity and clinical implications.
COX-1 (Constitutive)
Present in stomach, kidneys, platelets
Produces protective prostaglandins
Inhibition causes GI toxicity and bleeding
COX-2 (Inducible)
Upregulated during inflammation
Target for anti-inflammatory effect
Selective inhibition reduces GI side effects
High-Yield NSAIDs Classification
Drug | COX Selectivity | Half-life | Key Points |
|---|---|---|---|
Aspirin | Irreversible COX-1/COX-2 | 15-20 min | Only irreversible NSAID |
Ibuprofen | Non-selective | 2-4 hours | Safest NSAID profile |
Diclofenac | COX-2 preferential | 1-2 hours | High CV risk |
Celecoxib | COX-2 selective | 11 hours | Reduced GI toxicity |
Indomethacin | Non-selective | 4-5 hours | High CNS toxicity |
Aspirin Mnemonic: "ASPIRIN ACTS"
Antiplatelet (irreversible)
Salicylism at high doses
Prostaglandin inhibition
Irreversible COX binding
Reye syndrome (avoid in children)
Inflammation reduction
No reversibility
When preparing for pharmacology sections, Oncourse's adaptive MCQ bank serves INICET-level questions specifically on NSAID selectivity and can filter by drug class to focus your weak areas.
NSAID Side Effects and Contraindications
Gastrointestinal Effects
Gastritis, peptic ulcers, bleeding
Mechanism: COX-1 inhibition reduces protective prostaglandins
Risk factors: Age >60, H. pylori, steroids, anticoagulants
Renal Effects
Acute kidney injury, fluid retention
Mechanism: Reduced prostaglandin-mediated renal blood flow
Higher risk in elderly, dehydrated, or CHF patients
Cardiovascular Effects
Increased MI and stroke risk (except aspirin)
COX-2 selective drugs have higher CV risk
Mechanism: Altered prostacyclin/thromboxane balance
DMARDs: Disease-Modifying Anti-Rheumatic Drugs
Conventional Synthetic DMARDs (csDMARDs)
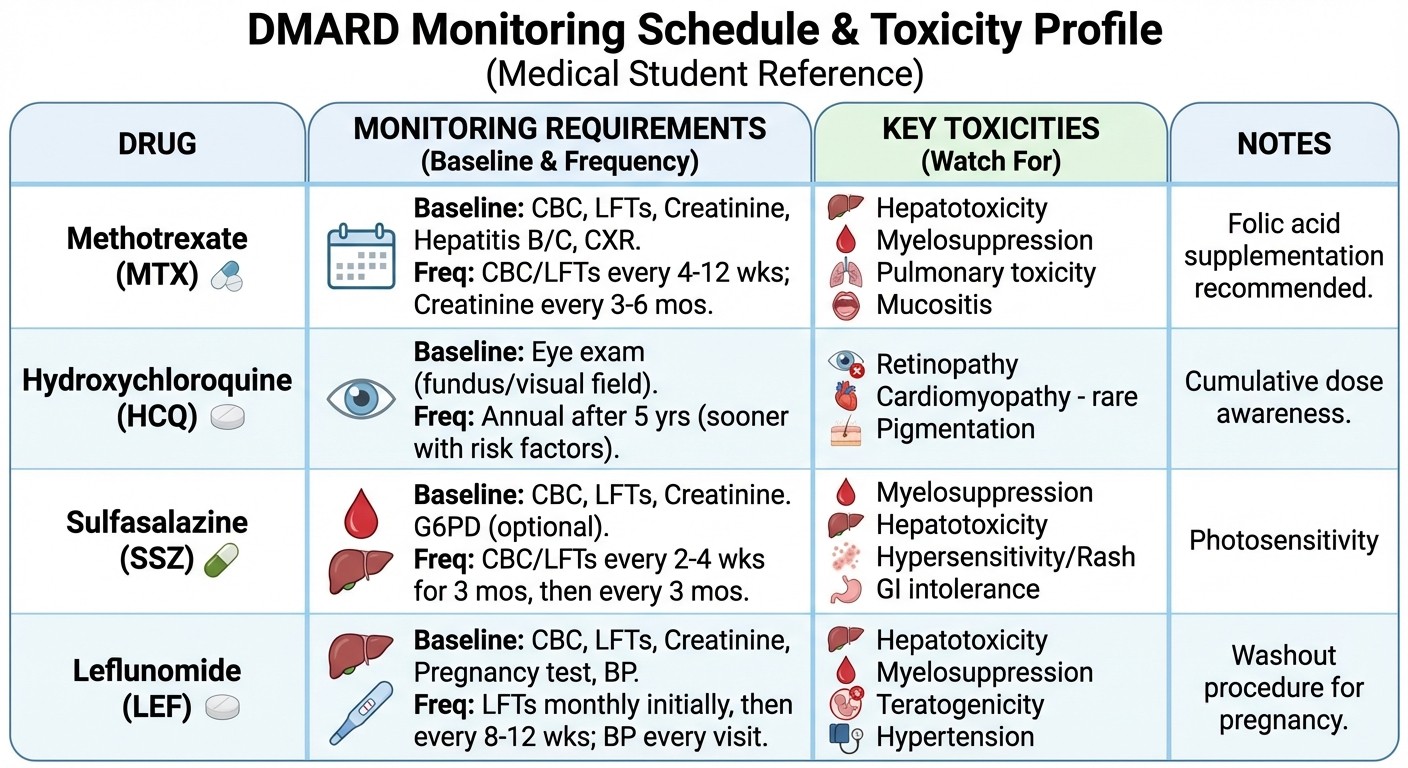
Methotrexate (MTX)
Mechanism: Dihydrofolate reductase inhibition
Dose: 7.5-25 mg weekly (oral/subcutaneous)
Monitoring: CBC, LFTs, creatinine every 4-8 weeks
Toxicity: Hepatotoxicity, pneumonitis, bone marrow suppression
Methotrexate Monitoring Mnemonic: "MTX CALLS BACK"
Monthly CBC initially
Twice yearly chest X-ray
X-tra folate supplementation
Creatinine every visit
ALT/AST every month
Liver biopsy if persistent elevation
Lung function if dyspnea
Stop if pancytopenia
Back to baseline before restarting
Alcohol counseling
Contraception counseling
Kidney function monitoring
The toxicity tables for DMARDs convert perfectly into spaced repetition flashcards on Oncourse — surfaces forgotten monitoring schedules at optimal intervals to cut review time significantly.
Hydroxychloroquine (HCQ)
Mechanism: Unclear — lysosomal pH alteration, TLR inhibition
Dose: 5 mg/kg/day (max 400 mg)
Monitoring: Annual ophthalmology exam
Toxicity: Retinal toxicity (irreversible), cardiomyopathy
Sulfasalazine (SSZ)
Mechanism: 5-ASA release in colon, unknown RA mechanism
Dose: 2-3 g daily in divided doses
Monitoring: CBC, LFTs
Toxicity: GI upset, rash, oligospermia (reversible)
Leflunomide
Mechanism: Dihydroorotate dehydrogenase inhibition
Active metabolite: A77 1726 (long half-life)
Monitoring: CBC, LFTs, blood pressure
Washout: Cholestyramine for toxicity/pregnancy
Targeted Synthetic DMARDs (tsDMARDs)
JAK Inhibitors
Mechanism: Janus kinase pathway inhibition
Examples: Tofacitinib (JAK1/JAK3), Baricitinib (JAK1/JAK2)
Monitoring: CBC, lipids, LFTs
Warnings: Infections, malignancy, thrombosis
Biologics: Targeted Immunotherapy
Anti-TNF Agents
Mechanism: TNF-α neutralization reduces inflammatory cascade
Drug | Type | Route | Half-life | Key Features |
|---|---|---|---|---|
Etanercept | TNF receptor fusion | SC | 3-5 days | Lower immunogenicity |
Infliximab | Chimeric mAb | IV | 8-10 days | Higher infusion reactions |
Adalimumab | Human mAb | SC | 14 days | Least immunogenic |
Golimumab | Human mAb | SC/IV | 14 days | Monthly dosing |
Certolizumab | PEGylated Fab | SC | 14 days | Safe in pregnancy |
Anti-TNF Contraindications Mnemonic: "TNF BLOCKS IMMUNITY"
Tuberculosis (active or latent)
Neurologic demyelinating disease
Fungal infections (systemic)
B-cell lymphoma risk
Live vaccines contraindicated
Opportunistic infections
CHF (moderate to severe)
Known hypersensitivity
Skin cancer (melanoma)
Immunodeficiency states
Malignancy (active)
Multiple sclerosis
Uncontrolled infections
Neutropenia
Infection screening required
TB screening mandatory
Yellow fever vaccine avoid
Oncourse's mock test analytics break down performance by rheumatology pharmacology topics, so students can see exactly where their anti-TNF knowledge stands vs INICET benchmarks.
Non-TNF Biologics
Tocilizumab (Anti-IL-6 Receptor)
Mechanism: IL-6 receptor antagonism
Route: IV or SC
Monitoring: Neutrophils, platelets, lipids, LFTs
Side effects: Infections, GI perforation, hepatotoxicity
Rituximab (Anti-CD20)
Mechanism: B-cell depletion
Use: RA, vasculitis, after TNF failure
Monitoring: Immunoglobulins, HBV reactivation
Premedication: Methylprednisolone, antihistamines
Abatacept (CTLA-4-Ig)
Mechanism: T-cell costimulation blockade
Route: IV or SC
Lower infection risk than TNF inhibitors
Avoid live vaccines
Anti-Gout Drugs: Acute and Chronic Management
Acute Gout Treatment
Colchicine
Mechanism: Microtubule polymerization inhibition
Dosing: 1.2 mg, then 0.6 mg 1 hour later
Maximum: 1.8 mg in 24 hours
Side effects: Diarrhea (dose-limiting), nausea
Colchicine Mechanism Mnemonic: "MICRO TUBES"
Microtubule disruption
Inflammation reduction
Chemotaxis inhibition
Rapid onset (1-2 hours)
Only for acute attacks initially
NSAIDs for Acute Gout
First-line: Indomethacin, naproxen, ibuprofen
Avoid aspirin (can precipitate attack at low doses)
Contraindications: Kidney disease, GI bleeding
Corticosteroids
Indications: NSAID/colchicine contraindicated
Options: Oral prednisolone, intra-articular injection
Taper over 7-14 days
Chronic Gout Prevention
Xanthine Oxidase Inhibitors Allopurinol
Mechanism: Xanthine oxidase inhibition
Starting dose: 100 mg daily, titrate up
Target: Uric acid <6 mg/dL
Major side effect: Stevens-Johnson syndrome (HLA-B*5801)
Drug interactions: Azathioprine, warfarin
Febuxostat
Mechanism: Selective xanthine oxidase inhibition
Advantages: Fewer drug interactions, safe in mild-moderate CKD
CV warning: Increased CV death vs allopurinol
Dose: 40-80 mg daily
Uricosuric Agents Probenecid
Mechanism: Blocks renal uric acid reabsorption
Requires normal kidney function (CrCl >50)
Drug interactions: Penicillins, NSAIDs
Contraindications: Kidney stones, high uric acid excretion
Uric Acid Lowering Comparison
Parameter | Allopurinol | Febuxostat | Probenecid |
|---|---|---|---|
Mechanism | XO inhibitor | XO inhibitor | Uricosuric |
CKD use | Dose adjust | Safe | Contraindicated |
Drug interactions | Many | Few | Moderate |
CV risk | Lower | Higher | Neutral |
Cost | Low | High | Moderate |
When reviewing complex drug interaction tables, students often miss key details. Practice with NSAIDs MCQs on Oncourse helps identify these commonly tested interaction patterns.
Glucocorticoids in Rheumatology
Mechanism and Potency
Anti-inflammatory Mechanism
Inhibit phospholipase A2 via lipocortin
Reduce prostaglandin and leukotriene synthesis
Suppress inflammatory cell migration
Relative Potencies (Anti-inflammatory)
Hydrocortisone: 1
Prednisolone: 4
Methylprednisolone: 5
Dexamethasone: 25
Clinical Applications
Pulse Therapy
Methylprednisolone 1 g IV daily × 3 days
Indications: Lupus nephritis, vasculitis, severe RA flares
Follow with oral taper
Bridge Therapy
Low-dose prednisolone (≤7.5 mg daily) while starting DMARDs
Provides symptom relief during DMARD onset lag
Minimize duration due to toxicity
Intra-articular Injection
Triamcinolone acetonide most common
Provides local anti-inflammatory effect
Avoid in infected joints
Common INICET MCQ Traps
High-Yield Trap Scenarios
Trap 1: MTX Toxicity Prevention
Question stem: "Patient on MTX develops mouth ulcers"
Trap: Increase MTX dose
Correct: Add folate supplementation
Trap 2: Anti-TNF Screening
Question stem: "Before starting etanercept..."
Trap: Only check CBC
Correct: TB screening (chest X-ray, IGRA, clinical assessment)
Trap 3: Gout Drug Timing
Question stem: "Patient starts allopurinol, develops acute attack"
Trap: Stop allopurinol immediately
Correct: Continue allopurinol, treat acute attack separately
Trap 4: COX-2 Selectivity
Question stem: "Safest NSAID for peptic ulcer patient"
Trap: Any non-selective NSAID
Correct: Celecoxib (but still monitor for CV risk)
Review comprehensive analgesics and anti-inflammatory drug flashcards to reinforce these commonly tested concepts through spaced repetition.
Frequently Asked Questions
What are the key differences between MTX and hydroxychloroquine monitoring?
MTX requires monthly CBC, LFTs, and creatinine due to hepatic and bone marrow toxicity. Hydroxychloroquine needs annual ophthalmology exams for retinal toxicity screening — the retinal damage is irreversible, making early detection critical.
Which anti-TNF agent is safest during pregnancy?
Certolizumab is preferred during pregnancy because it's PEGylated and doesnt cross the placenta. Etanercept and adalimumab cross minimally in first trimester but should be stopped before third trimester.
Why cant you use aspirin for acute gout attacks?
Low-dose aspirin can precipitate gout attacks by reducing uric acid excretion through the kidneys. High-dose aspirin (>3g daily) is uricosuric but impractical due to toxicity. Use indomethacin, naproxen, or colchicine instead.
What's the mechanism behind rituximab delayed infections?
Rituximab depletes CD20-positive B cells, reducing antibody production for 6-12 months. This creates prolonged immunosuppression beyond the drug's half-life, requiring infection vigilance long after treatment.
How do you distinguish between febuxostat and allopurinol drug interactions?
Allopurinol inhibits xanthine oxidase and aldehyde oxidase, affecting azathioprine, mercaptopurine, and warfarin metabolism. Febuxostat selectively inhibits xanthine oxidase only, causing fewer drug interactions — key advantage for poly-pharmacy patients.
Which DMARD requires cholestyramine washout?
Leflunomide's active metabolite (A77 1726) has a very long half-life. Cholestyramine binds the metabolite in the gut, accelerating elimination during toxicity or before pregnancy. This washout protocol is unique to leflunomide.
For deeper understanding of these drug mechanisms and interactions, explore our comprehensive pharmacology lessons covering each drug class in detail.
---
Master these core concepts and INICET rheumatology pharmacology becomes pattern recognition. Every drug class follows predictable testing patterns — mechanism, monitoring, contraindications, and drug interactions. Focus on the high-yield details that distinguish similar drugs.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for INICET. Download free on Android and iOS.