Back
INICET CNS Pharmacology Glossary 2026: Antiepileptics, Antipsychotics & Antidepressants High-Yield Drug List
Master INICET CNS pharmacology with this comprehensive glossary covering antiepileptics, antipsychotics, and antidepressants. High-yield drug list, mechanisms, mnemonics, and exam patterns for 2026.

INICET CNS Pharmacology Glossary 2026: Antiepileptics, Antipsychotics & Antidepressants High-Yield Drug List
You are staring at your INICET preparation timeline. Three months left. Pharmacology feels overwhelming — 500+ drugs, countless mechanisms, drug interactions that make your head spin. But here's what INICET veterans know: CNS pharmacology isnt about memorizing every drug. It's about mastering the 30-40 high-yield drugs that show up repeatedly.
INICET loves CNS pharmacology. In the last 5 INICET exams, CNS drugs accounted for 18-22% of the total pharmacology questions — that's 8-10 MCQs guaranteed. The pattern is predictable: antiepileptics (3-4 questions), antipsychotics (2-3 questions), and antidepressants (2-3 questions). Master these three classes, and you've locked 7-10 easy marks.
This glossary covers exactly what INICET tests: mechanisms, classifications, key drugs, side effects, and the clinical pearls that separate toppers from the rest. No textbook fluff — just the drug facts that convert to marks.
Why CNS Pharmacology is a Must-Win in INICET
CNS pharmacology has the highest repeat rate in INICET. The same 30 drugs appear across multiple years, often with identical question stems. INICET 2023 repeated 4 CNS pharmacology MCQs from previous years — exact questions, different options.
Here's the weightage breakdown from INICET 2021-2025:
Antiepileptics: 3.2 questions per exam (16% of pharma)
Antipsychotics: 2.8 questions per exam (14% of pharma)
Antidepressants: 2.4 questions per exam (12% of pharma)
Total CNS: 8.4 questions per exam (42% of pharmacology section)
The pattern is mechanism-heavy. INICET rarely asks brand names or dosages. Instead, they test:
MOA-based drug classification
Side effect profiles
Drug interactions
Clinical scenarios requiring specific drugs
Students who drill these three classes report 90%+ accuracy in CNS pharmacology MCQs. The return on time invested is massive — 3 weeks of focused study can lock 8-10 marks for the next 5 years.
Antiepileptics: First-Line Drugs and INICET Favorites
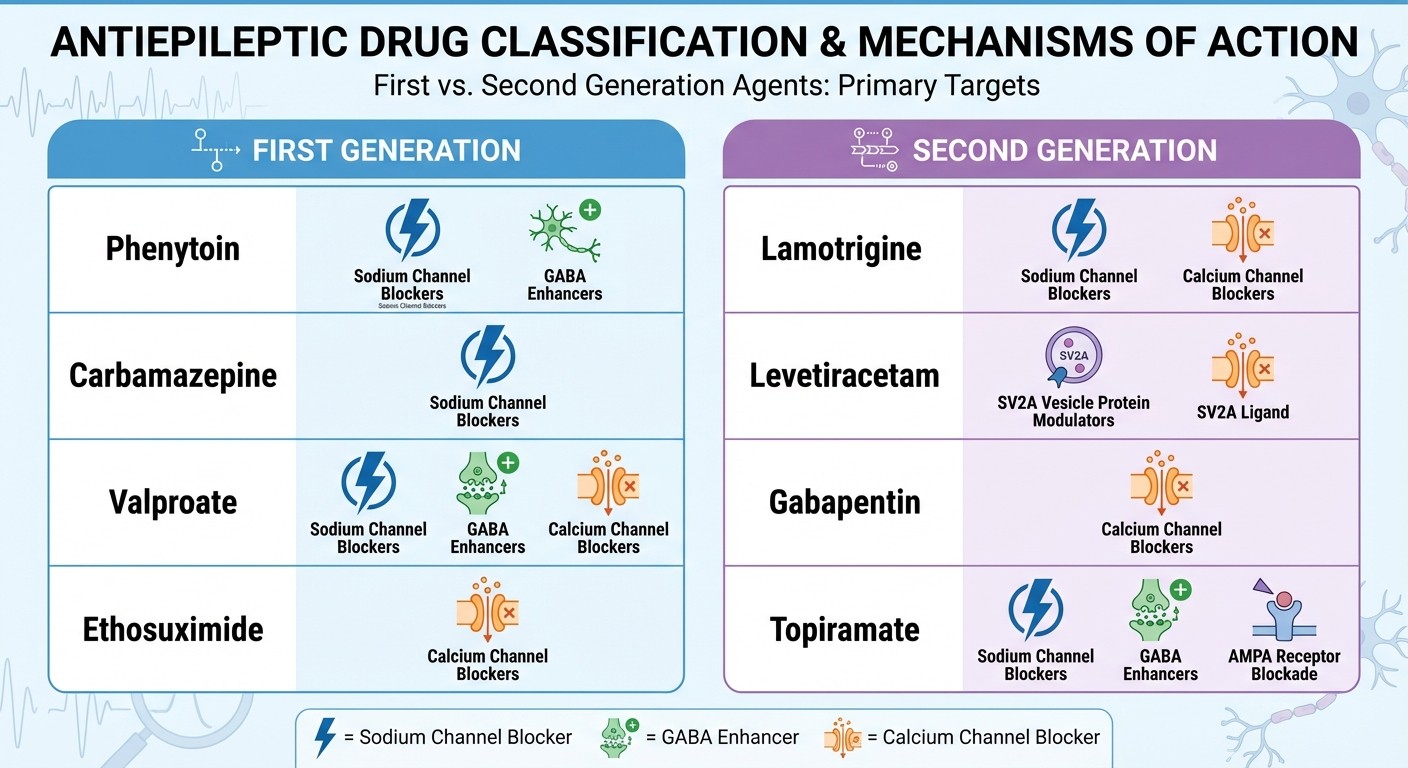
Drug Classification: Generation-Based Approach
First Generation (1950s-1980s):
Phenytoin (MOA: Na+ channel blocker)
Carbamazepine (MOA: Na+ channel blocker)
Sodium valproate (MOA: Multiple — Na+ channels, GABA enhancement, Ca2+ channels)
Ethosuximide (MOA: T-type Ca2+ channel blocker)
Second Generation (1990s-2000s):
Lamotrigine (MOA: Na+ channel blocker + Ca2+ channels)
Levetiracetam (MOA: SV2A protein modulation)
Gabapentin (MOA: Ca2+ channel α2δ subunit blocker)
Topiramate (MOA: Multiple — Na+ channels, GABA, carbonic anhydrase inhibition)
High-Yield INICET Drugs
1. Sodium Valproate
MOA: Blocks Na+ channels, enhances GABA, blocks T-type Ca2+ channels
Spectrum: Broad — focal, generalized tonic-clonic, absence, myoclonic
INICET pearl: Only antiepileptic effective in ALL seizure types
Key side effects: Hepatotoxicity, teratogenicity (neural tube defects), hair loss, weight gain
INICET trap: Contraindicated in pregnancy (Category D), especially neural tube defects
2. Phenytoin
MOA: Voltage-gated Na+ channel blocker (state-dependent)
Uses: Focal seizures, generalized tonic-clonic, status epilepticus (IV)
Zero-order kinetics: Small dose increases → large plasma level jumps
Key side effects: Gingival hyperplasia, hirsutism, coarsening of facial features, megaloblastic anemia
INICET pattern: Questions on zero-order kinetics and dental side effects
Practice CNS pharmacology MCQs with targeted difficulty using Oncourse's adaptive question bank — filter by antiepileptics and drill only the drugs that appeared in the last 5 INICET exams. 3. Carbamazepine
MOA: Voltage-gated Na+ channel blocker
Uses: Focal seizures, trigeminal neuralgia, bipolar disorder
Autoinduction: Induces its own metabolism (CYP3A4)
Key side effects: Diplopia, ataxia, hyponatremia, aplastic anemia (rare)
INICET favorite: Hyponatremia mechanism (SIADH-like effect)
4. Lamotrigine
MOA: Na+ channel blocker + presynaptic Ca2+ channel blocker
Uses: Focal, generalized, Lennox-Gastaut syndrome
Key advantage: Minimal weight gain, good cognitive profile
INICET warning: Stevens-Johnson syndrome with rapid titration
5. Levetiracetam
MOA: Binds SV2A protein (synaptic vesicle protein)
Uses: Focal, myoclonic, generalized tonic-clonic
Advantages: No drug interactions, renal elimination
INICET pearl: Safe in liver disease, pregnancy Category C
6. Ethosuximide
MOA: T-type Ca2+ channel blocker in thalamus
Specific use: Absence seizures (first-line)
INICET pattern: Always tested with absence seizure scenarios
Side effects: GI upset, drowsiness, rare blood dyscrasias
INICET MCQ Patterns for Antiepileptics
1. MOA-based classification: "Which drug blocks T-type calcium channels?" (Answer: Ethosuximide)
2. Seizure type matching: "First-line drug for absence seizures in a 7-year-old" (Answer: Ethosuximide)
3. Side effect profiles: "Gingival hyperplasia is seen with..." (Answer: Phenytoin)
4. Drug interactions: "Which antiepileptic shows autoinduction?" (Answer: Carbamazepine)
5. Pregnancy categories: "Safest antiepileptic in pregnancy" (Answer: Lamotrigine or Levetiracetam)
High-yield mnemonic for Na+ channel blockers: "PHiLly CaLLs" — PHenytoin, Lamotrigine, Carbamazepine, Lacosamide, Lidocaine
Antipsychotics: Typical vs Atypical Mechanisms
Classification: Dopamine Receptor Basis
Typical Antipsychotics (First Generation)
MOA: D2 receptor antagonism (primarily)
Prototype: Haloperidol, Chlorpromazine, Fluphenazine
Efficacy: Positive symptoms > Negative symptoms
Major issue: Extrapyramidal side effects (EPS)
Atypical Antipsychotics (Second Generation)
MOA: D2 + 5-HT2A receptor antagonism (balanced)
Prototype: Clozapine, Risperidone, Olanzapine, Quetiapine, Aripiprazole
Efficacy: Positive + Negative symptoms
Advantage: Lower EPS risk, better tolerability
INICET High-Yield Antipsychotics
1. Haloperidol (Typical)
MOA: High-potency D2 receptor antagonist
Clinical use: Acute psychosis, Tourette syndrome, delirium
INICET focus: Highest EPS risk among antipsychotics
Side effects: Acute dystonia, parkinsonism, tardive dyskinesia, neuroleptic malignant syndrome
Pearl: IV form used in ICU for delirium
2. Clozapine (Atypical)
MOA: D1, D2, D4 + 5-HT2A, α1, M1, H1 receptor antagonism
Unique indication: Treatment-resistant schizophrenia
INICET danger: Agranulocytosis (1-2%) — requires weekly CBC monitoring
Other side effects: Seizures, metabolic syndrome, myocarditis
Pearl: Most effective antipsychotic but highest monitoring requirements
Each MCQ on Oncourse comes with detailed AI explanations covering MOA, classification, side effects, and clinical scenarios — students see why haloperidol causes EPS or why clozapine requires CBC monitoring, embedded in context. 3. Risperidone (Atypical)
MOA: D2 + 5-HT2A antagonism with high D2 affinity
Clinical use: Schizophrenia, bipolar mania, autism (behavioral)
INICET pattern: Higher EPS risk among atypicals (due to high D2 affinity)
Side effects: Hyperprolactinemia, weight gain, diabetes risk
4. Olanzapine (Atypical)
MOA: D2 + 5-HT2A + H1 + M1 antagonism
Clinical use: Schizophrenia, bipolar disorder
INICET focus: Highest weight gain and metabolic risk
Monitoring: Lipids, glucose, weight every 3 months
5. Aripiprazole (Atypical)
MOA: D2 partial agonist + 5-HT2A antagonist + 5-HT1A partial agonist
Unique feature: Dopamine system stabilizer (agonist at low dopamine, antagonist at high dopamine)
Advantages: Weight neutral, low EPS, low prolactin elevation
INICET pearl: Safest metabolic profile among antipsychotics
Side Effects Tested in INICET
Extrapyramidal Side Effects (EPS) — Typical > Atypical 1. Acute dystonia (hours): Muscle spasms, torticollis — treat with anticholinergics 2. Parkinsonism (days-weeks): Bradykinesia, rigidity, tremor 3. Akathisia (weeks): Motor restlessness, cannot sit still 4. Tardive dyskinesia (months-years): Irreversible orofacial movements Non-EPS Side Effects
Metabolic: Weight gain, diabetes, dyslipidemia (Olanzapine > Risperidone > Haloperidol)
Cardiac: QT prolongation (especially Haloperidol IV)
Endocrine: Hyperprolactinemia → galactorrhea, amenorrhea, erectile dysfunction
Hematologic: Agranulocytosis (Clozapine only)
INICET trap question pattern: "A patient on antipsychotics develops fever, muscle rigidity, elevated CK" — Answer: Neuroleptic malignant syndrome (discontinue drug, supportive care, dantrolene)
Antidepressants: MOA-Based Classification
Major Classes and Mechanisms
1. Tricyclic Antidepressants (TCAs)
MOA: Block serotonin and norepinephrine reuptake + anticholinergic effects
Prototype drugs: Amitriptyline, Imipramine, Desipramine, Nortriptyline
Clinical uses: Major depression, neuropathic pain, migraine prophylaxis
INICET focus: Anticholinergic side effects and cardiotoxicity
2. Selective Serotonin Reuptake Inhibitors (SSRIs)
MOA: Selective 5-HT reuptake inhibition
Drugs: Fluoxetine, Sertraline, Paroxetine, Citalopram, Escitalopram
Advantages: Fewer side effects than TCAs, safer in overdose
INICET pattern: First-line for depression and anxiety disorders
Master antidepressant classifications with Oncourse's spaced repetition flashcards — organized by MOA and clinical use, with built-in recall testing. 3. Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
MOA: Dual inhibition of 5-HT and NE reuptake
Drugs: Venlafaxine, Duloxetine, Desvenlafaxine
Uses: Depression, generalized anxiety disorder, neuropathic pain
INICET advantage: Better efficacy than SSRIs in severe depression
4. Monoamine Oxidase Inhibitors (MAOIs)
MOA: Irreversible MAO-A and MAO-B enzyme inhibition
Drugs: Phenelzine, Tranylcypromine, Isocarboxazid
Uses: Atypical depression, treatment-resistant depression
INICET danger: Tyramine interactions → hypertensive crisis
High-Yield Antidepressants for INICET
1. Amitriptyline (TCA)
MOA: 5-HT > NE reuptake inhibition + anticholinergic + antihistaminic
Uses: Depression, neuropathic pain, migraine prophylaxis, IBS
Side effects: Dry mouth, constipation, urinary retention, sedation, weight gain
INICET trap: Cardiotoxicity in overdose (Na+ channel blockade)
2. Fluoxetine (SSRI)
MOA: Selective 5-HT reuptake inhibition
Unique features: Longest half-life (4-6 days), active metabolite (norfluoxetine)
Uses: Depression, OCD, bulimia, PMDD
INICET pearl: Least withdrawal symptoms due to long half-life
3. Sertraline (SSRI)
MOA: Selective 5-HT reuptake inhibition + mild dopamine reuptake inhibition
Advantages: Minimal drug interactions, safe in cardiac disease
Uses: Depression, panic disorder, PTSD, social anxiety
INICET preference: First-line SSRI in post-MI depression
4. Venlafaxine (SNRI)
MOA: 5-HT reuptake inhibition (low dose) + NE reuptake inhibition (high dose)
Uses: Depression, GAD, social anxiety disorder
Side effects: Hypertension (dose-dependent), discontinuation syndrome
INICET pattern: Effective in treatment-resistant depression
5. Duloxetine (SNRI)
MOA: Balanced 5-HT and NE reuptake inhibition
Uses: Depression, diabetic neuropathy, fibromyalgia, chronic pain
INICET advantage: FDA-approved for multiple pain conditions
Monitoring: Liver function (hepatotoxicity risk)
Clinical Uses by Disorder
Condition | First-Line Drug | INICET Pearl |
|---|---|---|
Major Depression | SSRI (Sertraline/Escitalopram) | Start low, titrate slowly |
Neuropathic Pain | TCA (Amitriptyline) or Duloxetine | Analgesic effect independent of antidepressant effect |
OCD | SSRI (Fluoxetine/Sertraline) | Higher doses needed vs depression |
Panic Disorder | SSRI (Sertraline/Paroxetine) | Avoid initial anxiety worsening |
PTSD | SSRI (Sertraline/Paroxetine) | FDA-approved specifically |
Fibromyalgia | Duloxetine or Pregabalin | SNRIs preferred over SSRIs |
INICET Overdose Patterns
TCA Overdose (Highly Tested)
Mechanism: Na+ channel blockade → cardiac conduction defects
Presentation: Confusion, seizures, wide QRS, hypotension, anticholinergic signs
Treatment: IV sodium bicarbonate (alkalinization), supportive care
INICET pearl: Sodium bicarbonate improves both CNS and cardiac toxicity
SSRI Overdose
Presentation: Generally safer, serotonin syndrome possible with drug interactions
Management: Supportive care, discontinue drug, cyproheptadine if serotonin syndrome
If Oncourse identifies antidepressants as a weak area through performance data, the adaptive study system schedules extra MCQ sessions and targeted revision on that specific drug class.
High-Yield Mnemonics for INICET
Antiepileptics
Sodium Channel Blockers: "PHiL CaLLs"
PHenytoin, isocarboxazid (actually Lamotrigine), Carbamazepine, Lacosamide, Lidocaine
Phenytoin Side Effects: "CHIPS"
Coarsening of facial features, Hirsutism, Insomnia, Peripheral neuropathy, Skin rash
Broad Spectrum AEDs: "VaL LeT"
Valproate, Lamotrigine, Levetiracetam, Topiramate
Antipsychotics
Typical Antipsychotics: "HaLT CHF"
Haloperidol, Loxapine, Trifluoperazine, CHlorpromazine, Fluphenazine
High-Potency Typicals (High EPS): "HaLT"
Haloperidol, Loxapine, Trifluoperazine
Low EPS Atypicals: "QuARO"
Quetiapine, ARipiprazole, Olanzapine
Clozapine Monitoring: "WBC"
Weekly, Blood count, Clozapine (agranulocytosis risk)
Antidepressants
Tricyclics: "AMID NoT"
Amitriptyline, Mipramine, Imipramine, Desipramine, Nortriptyline, Trimipramine
SSRIs: "FLuPa CiEs"
Fluoxetine, Luvox (fluvoxamine), Paroxetine, Citalopram, Escitalopram, Sertraline
TCA Overdose Treatment: "BIKES"
Bicarbonate (sodium), Intubation, Kardiac monitoring, Elimination enhancement, Supportive care
Common INICET Traps and High-Yield Facts
Antiepileptic Traps
1. Valproate in pregnancy: Highest teratogenic risk (neural tube defects) — avoid in women of childbearing age
2. Phenytoin kinetics: Zero-order elimination means small dose increases cause large plasma level jumps
3. Carbamazepine autoinduction: Drug levels decrease over first few weeks as it induces its own metabolism
4. Lamotrigine + Valproate: Valproate inhibits lamotrigine metabolism → increased toxicity risk
5. Ethosuximide specificity: Only effective for absence seizures — useless in other seizure types
Antipsychotic Traps
1. Clozapine monitoring: Weekly CBC for first 6 months, then biweekly for 6 months, then monthly
2. Haloperidol in elderly: High risk of EPS and falls — avoid in dementia-related psychosis
3. QT prolongation: All antipsychotics can prolong QT, but IV haloperidol has highest risk
4. Tardive dyskinesia: Usually irreversible, higher risk with typicals and long duration
5. Neuroleptic malignant syndrome: Discontinue all dopaminergic drugs immediately, supportive care
Antidepressant Traps
1. SSRI discontinuation: Paroxetine has worst withdrawal syndrome due to short half-life and anticholinergic activity
2. MAOIs + Tyramine: Aged cheese, wine, cured meats cause hypertensive crisis
3. TCA overdose: Tricyclic antidepressant toxicity needs sodium bicarbonate, not just supportive care
4. Serotonin syndrome: Hyperthermia + muscle rigidity + altered mental status with serotonergic drug combinations
5. Fluoxetine washout: Need 5-week washout before starting MAOI due to long half-life
INICET-Specific Drug Facts
Most Repeated Questions (2021-2025)
1. "Drug of choice for absence seizures" — Ethosuximide (appeared 4 times)
2. "Antipsychotic requiring CBC monitoring" — Clozapine (appeared 4 times)
3. "TCA overdose treatment" — Sodium bicarbonate (appeared 3 times)
4. "Broad spectrum antiepileptic" — Valproate (appeared 3 times)
5. "SSRI with longest half-life" — Fluoxetine (appeared 3 times)
New Pattern Questions (2024-2025)
Mechanism-based drug selection ("Which antidepressant blocks both 5-HT and NE reuptake?")
Drug interaction scenarios ("Patient on phenytoin started on oral contraceptives...")
Side effect management ("Patient on haloperidol develops muscle rigidity and fever...")
Pediatric vs adult indications ("First-line antiepileptic in pediatric absence seizures...")
Frequently Asked Questions
Which antiepileptic is safest in pregnancy?
Lamotrigine and levetiracetam are considered safest (Category C). Avoid valproate (Category D) due to neural tube defects. Folic acid supplementation is essential with all antiepileptics in pregnancy.
How do you differentiate typical from atypical antipsychotics?
Typicals primarily block D2 receptors and cause more EPS. Atypicals block both D2 and 5-HT2A receptors with lower EPS risk. Clozapine is the prototype atypical but requires monitoring for agranulocytosis.
What's the difference between serotonin syndrome and neuroleptic malignant syndrome?
Serotonin syndrome: hyperthermia + hyperreflexia + clonus + altered mental status (from excess serotonin). NMS: hyperthermia + lead pipe rigidity + altered mental status (from dopamine blockade). Both need immediate drug discontinuation.
Which TCA is best for neuropathic pain?
Amitriptyline is first-line for neuropathic pain due to balanced 5-HT/NE reuptake inhibition. Start low (10-25mg) and titrate slowly. The analgesic effect is independent of antidepressant effect.
How long should you continue antidepressants?
First episode: 6-9 months after remission. Recurrent episodes: 2+ years. Some patients need lifelong therapy. INICET tests duration concepts for different psychiatric conditions.
What's the mechanism of lamotrigine?
Lamotrigine blocks voltage-gated sodium channels (use-dependent) and presynaptic calcium channels. It's effective in focal, generalized, and Lennox-Gastaut syndrome seizures with minimal cognitive side effects.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for INICET. Download free on Android and iOS.