Back
7 High-Yield Cardiology Topics for NEET PG 2026 (With Must-Know ECG Patterns)
Master the 7 most tested cardiology topics in NEET PG 2026. Complete ECG patterns, clinical vignettes, and exam-focused insights for MI, AF, heart failure, and more.

7 High-Yield Cardiology Topics for NEET PG 2026 (With Must-Know ECG Patterns)
You are probably staring at another cardiology textbook right now, wondering which topics will actually show up in NEET PG 2026. Here is the reality: cardiology makes up 12-15% of your internal medicine questions, and 7 specific topics account for nearly 70% of those questions.
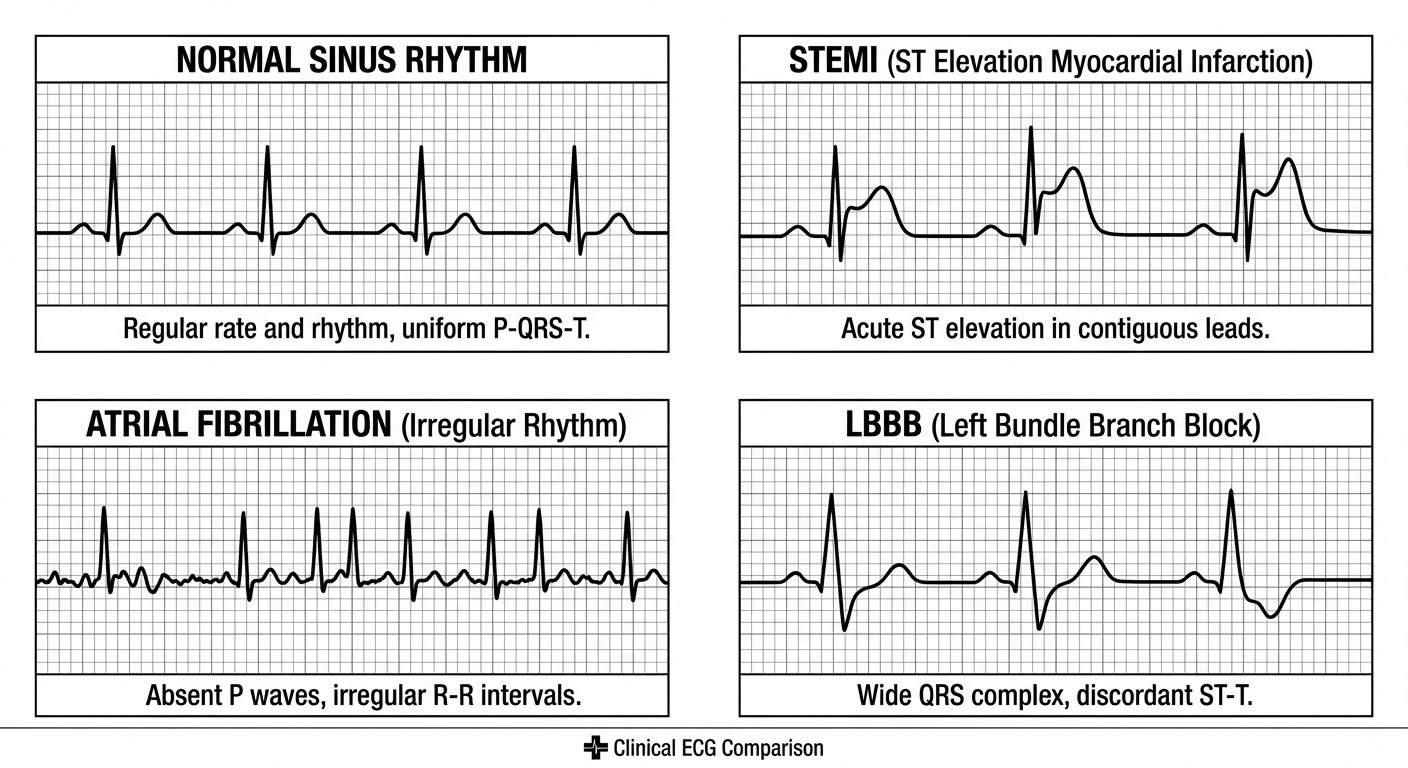
NEET PG doesnt test obscure syndromes. It tests pattern recognition — can you spot a STEMI on ECG, differentiate LBBB from RBBB, or recognize the irregular rhythm of atrial fibrillation? The examiners want to see if you can think like a clinician, not memorize like a textbook.
This guide breaks down the 7 most frequently tested cardiology topics in NEET PG, complete with the ECG patterns that show up year after year. Each topic includes the specific clinical vignette clues that help you nail the answer in under 60 seconds.
1. Acute Myocardial Infarction — STEMI vs NSTEMI ECG Changes
Why it is high-yield: MI questions appear in 85% of NEET PG papers. The examiners love testing ECG interpretation combined with management decisions — thrombolysis vs PCI, Sgarbossa criteria for LBBB, and troponin timing. Must-know ECG patterns:
STEMI: ST elevation >1mm in 2 contiguous leads (>2mm in V2-V3)
NSTEMI: ST depression, T-wave inversions, or normal ECG with elevated troponins
Sgarbossa criteria for LBBB: Concordant ST elevation >1mm (5 points), concordant ST depression >1mm in V1-V3 (3 points), discordant ST elevation >5mm (2 points). Score ≥3 = STEMI equivalent.
Clinical vignette clue: "55-year-old male with chest pain radiating to left arm for 2 hours, diaphoresis, ECG shows..." — if you see ST elevation, think STEMI and immediate reperfusion. Oncourse's adaptive question bank automatically identifies if you are missing MI subtype differentiation and drills targeted practice until you can spot these patterns instantly. High-yield fact: Posterior MI shows tall R waves and ST depression in V1-V2 (mirror image). Always check posterior leads V7-V9 if suspected.
2. Atrial Fibrillation — Irregularly Irregular Rhythm Recognition
Why it is high-yield: AF appears in 40% of NEET PG cardiology questions, often combined with stroke risk stratification (CHADS2 scoring) and anticoagulation decisions. Must-know ECG patterns:
Irregularly irregular rhythm with absent P waves
Fibrillatory waves (f-waves) instead of organized P waves
Variable RR intervals with no pattern
Rate: Often 100-180 bpm if uncontrolled
Clinical vignette clue: "Elderly patient with palpitations, irregular pulse, ECG shows absence of P waves and irregular RR intervals..." — the key is recognizing that irregularly irregular rhythm = AF until proven otherwise. CHADS2 scoring (memorize this):
CHF (1 point)
Hypertension (1 point)
Age >75 (1 point)
Diabetes (1 point)
Stroke/TIA history (2 points)
Score ≥2 = anticoagulation indicated
Rate control vs rhythm control: Rate control (beta-blockers, calcium channel blockers) is first-line unless patient is young (<65), symptomatic, or has new-onset AF.
3. Heart Failure — Left vs Right Ventricular Failure ECG Clues
Why it is high-yield: Heart failure questions combine ECG interpretation with clinical correlation — can you spot LVH criteria and match it to the clinical picture of dyspnea and orthopnea? Must-know ECG patterns:
LVF ECG: LVH criteria (see topic 5), LAD, poor R-wave progression
RVF ECG: RAD, tall R waves in V1-V2, deep S waves in V5-V6, P-pulmonale
Acute heart failure: May show new Q waves (if post-MI) or strain patterns
Clinical vignette clue: "Patient with dyspnea on exertion, bilateral ankle edema, JVP raised, ECG shows..." — match the ECG pattern to symptoms. LVF = pulmonary edema symptoms, RVF = systemic edema symptoms. High-yield clinical correlation:
LVF: Dyspnea, orthopnea, PND, pulmonary crackles
RVF: JVP elevation, hepatomegaly, ankle edema, ascites
When studying heart failure pathophysiology, Clinical Rounds presents these exact case vignettes in NEET PG format, helping you practice systematic ECG interpretation under timed conditions.
4. Valvular Heart Disease — Murmur Patterns and ECG Findings
Why it is high-yield: Valvular disease questions test your ability to correlate murmur characteristics with ECG changes and hemodynamic consequences. Must-know patterns by valve: Mitral Stenosis (MS):
Murmur: Low-pitched, rumbling, diastolic at apex
ECG: LAE (P-mitrale), RAE, AF common
Clinical: Dyspnea, hemoptysis, malar flush
Mitral Regurgitation (MR):
Murmur: High-pitched, blowing, systolic at apex → axilla
ECG: LAE, LVH (chronic), AF
Clinical: Fatigue, dyspnea, displaced apex
Aortic Stenosis (AS):
Murmur: Harsh, crescendo-decrescendo systolic, second ICS right sternal border
ECG: LVH, LAE, may have LBBB
Clinical: Triad — dyspnea, angina, syncope
Aortic Regurgitation (AR):
Murmur: High-pitched, blowing, early diastolic at left sternal border
ECG: LVH, wide pulse pressure signs
Clinical: Wide pulse pressure, water hammer pulse
High-yield tip: Systolic murmurs = AS or MR. Diastolic murmurs = AR or MS. Location tells you which valve.
5. Hypertensive Heart Disease — LVH Criteria Recognition
Why it is high-yield: LVH criteria questions are guaranteed in NEET PG. Memorize the voltage criteria — they appear in straightforward ECG interpretation questions. Must-know LVH criteria: Sokolow-Lyon criteria:
S in V1 + R in V5 or V6 ≥35mm
Most commonly tested in NEET PG
Cornell voltage criteria:
Men: S in V3 + R in aVL ≥28mm
Women: S in V3 + R in aVL ≥20mm
Additional LVH signs:
LAE (P-wave >120ms in lead II)
Strain pattern (ST depression, T-wave inversion in V5-V6)
Prolonged QRS duration (>120ms)
Clinical vignette clue: "Hypertensive patient, ECG shows increased voltage in lateral leads..." — calculate Sokolow-Lyon first, then look for strain patterns.
Using Synapses spaced-repetition, you can lock in these exact voltage numbers with daily 10-minute cardiology review sessions — the memory technique ensures you wont blank on criteria during the exam.
6. Conduction Defects — Bundle Branch Blocks and AV Blocks
Why it is high-yield: Conduction defects combine ECG pattern recognition with understanding of cardiac conduction system anatomy. NEET PG loves testing LBBB vs RBBB morphology and AV block progression. Bundle Branch Block patterns: LBBB (QRS >120ms):
V1: Broad, deep QS or rS
V6: Broad, notched R wave (RsR')
Memory: "WiLLiaM" — W in V1, M in V6
RBBB (QRS >120ms):
V1: rsR' pattern (rabbit ears)
V6: Wide S wave
Memory: "MaRRoW" — M in V1, W in V6
AV Block progression: 1st degree: PR interval >200ms, all P waves conducted 2nd degree Mobitz I (Wenckebach): Progressive PR prolongation until dropped QRS 2nd degree Mobitz II: Fixed PR interval with sudden dropped QRS 3rd degree (complete): Complete AV dissociation, independent P waves and QRS Clinical correlation: LBBB may indicate underlying cardiac disease. New LBBB in chest pain = consider STEMI equivalent.
7. Pericarditis and Myocarditis — Inflammatory ECG Changes
Why it is high-yield: Inflammatory heart disease questions test your ability to differentiate pericarditis from MI based on ECG patterns and clinical presentation. Pericarditis ECG stages:
Stage 1: Widespread saddle-shaped ST elevation, PR depression
Stage 2: Normalization of ST/PR
Stage 3: T-wave inversions
Stage 4: Resolution
Key differentiating features:
Pericarditis: Saddle-shaped ST elevation, PR depression, no reciprocal changes
MI: Localized ST elevation with reciprocal ST depression
Myocarditis: Similar to pericarditis but may have conduction defects
Clinical vignette clue: "Young patient with chest pain, friction rub, ECG shows diffuse ST elevation without reciprocal changes..." — widespread saddle-shaped ST elevation = pericarditis. High-yield clinical pearls:
Pericarditis pain: Sharp, positional, worse lying flat
Myocarditis: May present with heart failure symptoms
Both can cause troponin elevation (unlike isolated pericarditis)
Quick Reference: ECG Pattern Recognition Table
Condition | Key ECG Finding | Clinical Clue |
|---|---|---|
STEMI | ST elevation >1mm in 2 contiguous leads | Acute chest pain + ECG changes |
NSTEMI | ST depression or normal ECG + troponins | Chest pain + negative ECG |
Atrial Fibrillation | Irregularly irregular, absent P waves | Palpitations, irregular pulse |
LVH | Sokolow-Lyon ≥35mm | Hypertension history |
LBBB | W in V1, M in V6, QRS >120ms | May indicate cardiac disease |
RBBB | M in V1, W in V6, QRS >120ms | Often benign finding |
Pericarditis | Saddle-shaped ST elevation, PR depression | Sharp, positional chest pain |
Study Strategy for NEET PG 2026 Cardiology
Focus your cardiology preparation on pattern recognition rather than pathophysiology memorization. Practice ECG interpretation daily — 10 strips per day builds pattern recognition faster than reading theory.
The adaptive question system identifies exactly which cardiology subtopics need reinforcement, automatically generating practice sets focused on your weak areas. When you miss arrhythmia questions repeatedly, it unlocks focused ECG interpretation pathways until you achieve mastery.
Master the clinical correlation: every ECG finding must match a clinical picture. NEET PG questions rarely give you isolated ECG strips — they embed them in clinical vignettes that guide your differential diagnosis.
Frequently Asked Questions
What is the most frequently tested cardiology topic in NEET PG?
Acute myocardial infarction (MI) appears in 85% of NEET PG papers, particularly STEMI vs NSTEMI differentiation and ECG interpretation. Focus on ST elevation criteria and Sgarbossa criteria for LBBB.
How do I remember LVH voltage criteria for the exam?
Use the Sokolow-Lyon criteria: S in V1 + R in V5/V6 ≥35mm. Create a mental image — "35 is the magic number for LVH." Practice calculating this on 50+ practice ECGs to build automatic recognition.
Which ECG findings indicate immediate intervention in NEET PG scenarios?
STEMI with ST elevation >1mm (thrombolysis/PCI), complete heart block with hemodynamic compromise (pacing), and new LBBB in acute chest pain (treat as STEMI equivalent). These require emergency management.
How can I differentiate pericarditis from MI on ECG?
Pericarditis shows widespread saddle-shaped ST elevation with PR depression and no reciprocal changes. MI shows localized ST elevation with reciprocal ST depression in opposite leads. Pericarditis affects all leads except aVR.
What is the best way to practice ECG interpretation for NEET PG?
Practice with timed ECG strips in exam format. Start with 30 seconds per strip, then reduce to 15 seconds. Focus on systematic interpretation: rate, rhythm, axis, intervals, morphology. Build pattern recognition through repetition.
How important is memorizing exact voltage criteria for NEET PG?
Critical. NEET PG directly tests LVH criteria (Sokolow-Lyon ≥35mm), prolonged QT (>440ms), and bundle branch block criteria (QRS >120ms). These numbers appear in straightforward calculation questions.
Master Cardiology for NEET PG 2026
These 7 topics form the foundation of NEET PG cardiology questions. Master the ECG patterns, clinical correlations, and high-yield facts — they will give you the confidence to tackle any cardiology question in under 60 seconds.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.