Back
INICET 2026 Surgery & Orthopedics High-Yield Topics: Must-Know Procedures, Fracture Classifications and Exam Strategy
Master INICET 2026 surgery and orthopedics with high-yield procedures, fracture classifications (Garden, Neer, AO/OTA), trauma management, and proven exam strategies from 5 years of paper analysis.

INICET 2026 Surgery & Orthopedics High-Yield Topics: Must-Know Procedures, Fracture Classifications and Exam Strategy
You are staring at 200 questions. Three hours. One chance to crack INICET 2026.
Surgery and orthopedics together make up nearly 25% of your paper. That's 50 questions where knowing the Garden classification cold or recognizing a Neer Type IV fracture in 30 seconds can make the difference between AIIMS and disappointment.
Here's what 5 years of INICET papers reveal: they dont test textbook definitions anymore. They drop you into clinical vignettes where a 65-year-old falls, shows you an X-ray, and ask for immediate management. No time for second-guessing fracture patterns or surgical approaches.
This guide breaks down exactly what works for INICET surgery prep. High-yield procedures that show up every year. Fracture classifications that can save you 2-3 marks per paper. And exam-day strategy that turns your prep into actual points.
Understanding INICET 2026 Surgery Pattern
INICET has shifted hard toward clinical decision-making. Gone are the days of "Name the classification" questions. Now you get:
Scenario-based vignettes: 70% of surgery questions come wrapped in patient presentations
Image-heavy questions: X-rays, CT scans, and clinical photos dominate
Management-focused options: "What's your next step?" not "What's the definition?"
Integrated knowledge: Surgery questions pull from anatomy, pathology, and pharmacology
The average INICET surgery question takes 63 seconds to solve. Speed matters as much as accuracy.
Question Distribution (2021-2025 Analysis):
Trauma & Emergency Surgery: 35%
GI Surgery: 25%
Orthopedic Procedures: 20%
Head & Neck Surgery: 12%
Miscellaneous: 8%
Your strategy should mirror these weightages.
High-Yield Surgery Topics That Repeat Every Year
Trauma Surgery Essentials
ATLS Principles (Shows up in 4-5 questions annually)
Primary survey: ABCDE approach with cervical spine protection
Shock classification and fluid resuscitation targets
Damage control surgery indications
Peritoneal lavage vs CT in unstable patients
Polytrauma Management
Definitive vs damage control approaches
Timing of orthopedic fixation in polytrauma
Fat embolism syndrome recognition
Compartment syndrome in multiple injuries
Oncourse's adaptive question bank identifies weak zones in trauma protocols, building your speed on emergency surgery scenarios where seconds count. The platform tracks which ATLS principles you consistently miss and delivers targeted practice until recognition becomes automatic. Abdominal Trauma
FAST exam interpretation
Grading of solid organ injuries (liver, spleen, kidney)
Non-operative management criteria for blunt trauma
Indications for exploratory laparotomy
General Surgery Must-Knows
Appendicitis (2-3 questions per paper)
Modified Alvarado Score components
CT findings in complicated appendicitis
Laparoscopic vs open approach decision factors
Post-appendectomy complications
Hernia Repair
Inguinal hernia: Lichtenstein vs TEP/TAPP techniques
Mesh selection and positioning
Complications: chronic pain, recurrence rates
Emergency presentations: strangulation management
Thyroid Surgery
Indications for total vs subtotal thyroidectomy
Recurrent laryngeal nerve anatomy and protection
Post-thyroidectomy hypocalcemia management
Completion thyroidectomy timing
Gallbladder Disease
Laparoscopic cholecystectomy: critical view of Calot
Conversion to open surgery criteria
Post-cholecystectomy syndrome
ERCP timing in choledocholithiasis
Breast Surgery
Breast Cancer Staging
TNM classification updates
Sentinel lymph node biopsy indications
Neoadjuvant therapy criteria
Breast conservation vs mastectomy
Benign Breast Disease
Fibroadenoma management by age
BIRADS classification and follow-up
Phyllodes tumor characteristics
Practice with Oncourse's spaced repetition flashcards helps cement breast cancer staging and BIRADS classifications. The system delivers cards like "T2N1M0 breast cancer staging" and "Sentinel node biopsy contraindications" at optimal intervals, turning forgettable lists into long-term recall.
Orthopedics High-Yield Classifications
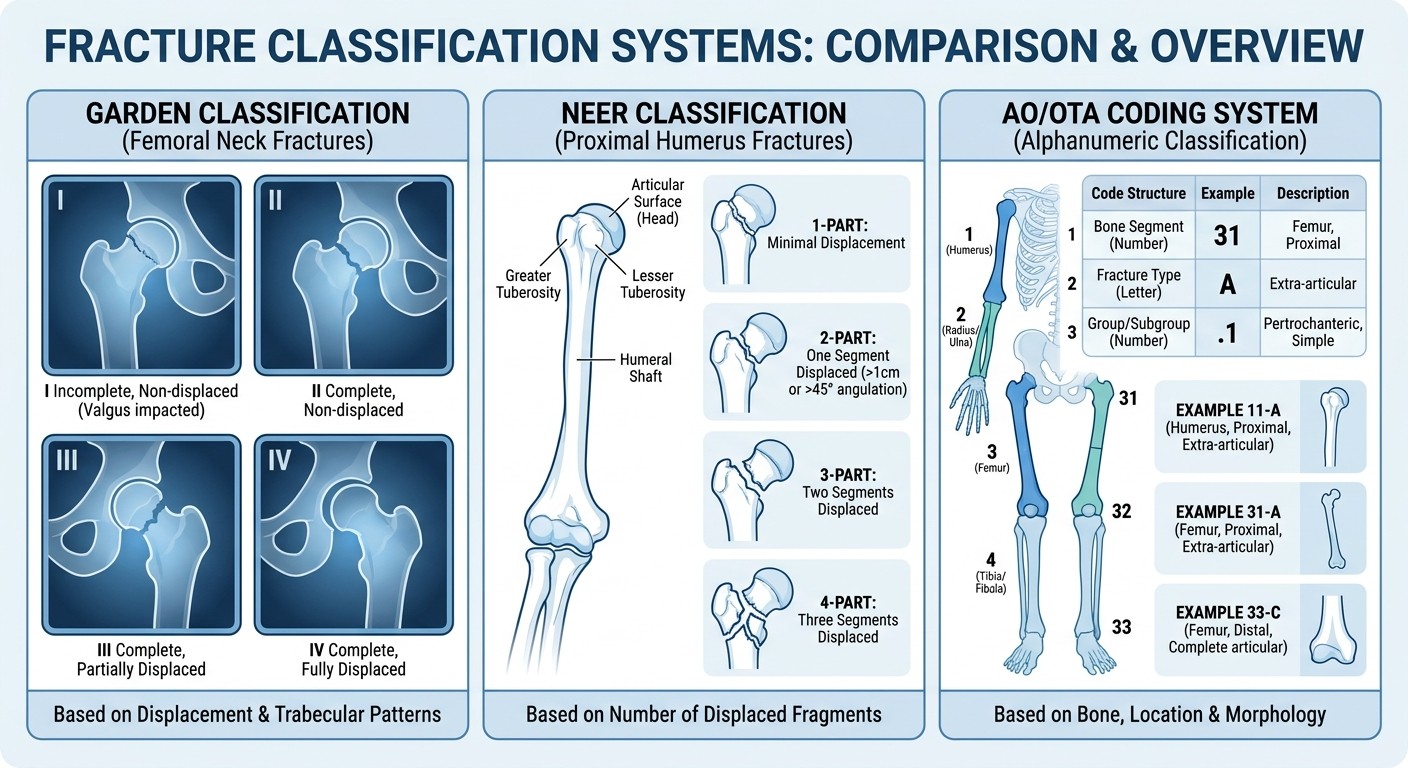
Garden Classification (Femoral Neck Fractures)
This shows up in 2-3 INICET questions annually. Master the staging:
Garden I: Incomplete, valgus-impacted fracture
Stable fracture pattern
Internal fixation preferred in younger patients
Good prognosis with proper reduction
Garden II: Complete, non-displaced fracture
Complete fracture line but no displacement
Generally stable, amenable to fixation
Risk of displacement if inadequately fixed
Garden III: Complete, partially displaced
Femoral head tilts into varus position
Unstable fracture pattern
Higher risk of avascular necrosis
Garden IV: Complete, fully displaced
Complete loss of femoral head alignment
Highest risk of complications
Often requires arthroplasty in elderly
Clinical Decision Points:
Garden I-II: Consider internal fixation if patient <65 years
Garden III-IV: Arthroplasty preferred in elderly (>70 years)
Young patients with Garden III-IV: Attempt reduction and fixation
Neer Classification (Proximal Humerus)
Focus on displacement criteria: >1cm displacement or >45° angulation defines a "part."
1-Part Fractures: No displaced segments
Conservative management with sling
Early mobilization at 1-2 weeks
Good functional outcomes expected
2-Part Fractures: One displaced segment
Surgical neck, greater tuberosity, or lesser tuberosity
Consider ORIF vs conservative based on patient factors
Age and activity level guide decision
3-Part Fractures: Two displaced segments
Usually involves surgical neck + tuberosity
ORIF preferred in younger patients
Higher complication rates
4-Part Fractures: Three displaced segments
High risk of avascular necrosis
Consider arthroplasty in elderly
Complex reconstruction in young patients
AO/OTA Classification System
Universal Coding Structure:
First digit: Bone (1=humerus, 2=radius/ulna, 3=femur, 4=tibia/fibula)
Second digit: Segment (1=proximal, 2=diaphysis, 3=distal)
Third digit: Type and group (A=simple, B=wedge, C=complex)
High-Yield AO Codes for INICET:
11-A: Simple proximal humerus fractures
11-B: Wedge proximal humerus fractures
11-C: Complex proximal humerus fractures
31-A: Simple proximal femur fractures
32-A: Simple femoral shaft fractures
Common Orthopedic Procedures and Indications
Hip Fractures Management
Intracapsular Fractures (Femoral Neck)
Garden I-II: Internal fixation with cannulated screws
Garden III-IV in elderly: Hemiarthroplasty or total hip replacement
Young patients: Attempt reduction and fixation regardless of displacement
Extracapsular Fractures
Stable intertrochanteric: Dynamic hip screw (DHS)
Unstable intertrochanteric: Intramedullary nail
Subtrochanteric: Reconstruction nail or cephalomedullary nail
Shoulder Injuries
Rotator Cuff Tears
Acute traumatic tears: Early surgical repair
Chronic degenerative tears: Conservative vs surgical based on function
Massive irreparable tears: Consider reverse shoulder arthroplasty
Shoulder Dislocations
Anterior dislocation: Most common, associated with Hill-Sachs lesion
Posterior dislocation: Associated with seizures, electrical injury
First-time vs recurrent dislocation management differs
Spine Trauma
Cervical Spine
C1-C2 injuries: Atlas fractures, odontoid fractures classification
Subaxial cervical spine: Allen-Ferguson classification
Neurologic assessment and clearing protocols
Thoracolumbar Spine
Denis three-column concept
Load-sharing classification for instrumentation
Neurologic injury patterns and prognosis
Essential Surgical Procedures
Laparoscopic Fundamentals
Port Placement Principles
Primary port: Umbilical vs Palmer's point in adhesions
Secondary ports: Triangulation and ergonomics
Safe entry techniques: Veress needle vs direct trocar
Key Laparoscopic Procedures
Laparoscopic cholecystectomy: Critical view achievement
Laparoscopic appendectomy: Mesoappendix division techniques
Laparoscopic hernia repair: TEP vs TAPP approach
Oncourse's performance analytics tracks your accuracy on laparoscopic decision points over time, flagging specific areas where you consistently lose marks on port placement or complication recognition. This evidence-based feedback keeps your INICET prep targeted rather than generic.
Emergency Procedures
Cricothyroidotomy
Indications: "Cant intubate, cant ventilate" scenarios
Anatomic landmarks and technique
Complications and conversion to tracheostomy
Chest Tube Insertion
Triangle of safety identification
Technique and sizing considerations
Management of persistent air leak
Fasciotomy
Compartment syndrome recognition
4-compartment leg fasciotomy technique
Wound management and closure timing
Common Outpatient Procedures
Skin and Soft Tissue
Excision margins for skin cancers
Local flap designs and limitations
Wound closure techniques and timing
Minor Hand Surgery
Trigger finger release
Carpal tunnel decompression
Ganglion cyst treatment options
Imaging Interpretation for Surgery
Trauma Imaging
FAST Exam
Four standard views and findings
Extended FAST for pneumothorax
Limitations and follow-up imaging
CT in Trauma
Contrast timing for different organ systems
Grading systems for solid organ injury
When to repeat imaging
Orthopedic Imaging
X-ray Interpretation
Standard views for common fractures
Radiographic signs of instability
Post-operative hardware assessment
Advanced Imaging
CT for intra-articular fractures
MRI indications in trauma
Bone scan applications
Perioperative Care Essentials
Preoperative Assessment
Risk Stratification
ASA classification and implications
Cardiac risk assessment (RCRI score)
Pulmonary function considerations
Optimization Strategies
Diabetes management in surgery
Anticoagulation bridging protocols
Nutrition assessment and support
Strengthen your understanding with our comprehensive surgery preparation lessons and test your knowledge with targeted surgery MCQs.
Postoperative Management
Pain Management
Multimodal analgesia principles
Opioid-sparing techniques
Regional anesthesia applications
Complication Recognition
Early warning signs of major complications
Systematic approach to post-op deterioration
When to return to OR
Surgical Site Infections
Prevention Strategies
Antibiotic prophylaxis timing and selection
Skin preparation techniques
Operating room environment factors
Treatment Principles
Classification of surgical site infections
Culture and antibiotic selection
Surgical management decisions
INICET Exam Strategy for Surgery
Time Management
Question Allocation:
Simple recall: 30 seconds max
Clinical vignettes: 90-120 seconds
Image-based questions: 60-90 seconds
Complex scenarios: 2-3 minutes maximum
Triage Strategy:
1. Scan all surgery questions first
2. Tackle high-confidence questions immediately
3. Mark difficult questions for review
4. Use remaining time for marked questions
Pattern Recognition
High-Yield Question Stems:
"Most appropriate next step": Usually asks for immediate management
"Most likely diagnosis": Focus on key clinical features
"Best treatment option": Consider patient factors and evidence
Image Question Approach:
1. Identify anatomical structures first
2. Look for obvious abnormalities
3. Correlate with clinical information
4. Apply classification systems when relevant
Common Trap Answers
Surgery Questions Often Include:
Overly aggressive management options
Outdated treatment approaches
Incomplete workup choices
Procedure-specific complications as distractors
Red Flags to Avoid:
Choosing surgery without adequate workup
Missing conservative management options
Ignoring patient comorbidities
Selecting procedures outside standard indications
High-Yield Facts and Mnemonics
Surgery Mnemonics
AMPLE History (Trauma)
Allergies
Medications
Past medical history
Last meal
Events leading to injury
5 Ps of Compartment Syndrome
Pain (out of proportion)
Pallor
Paresthesias
Pulselessness
Paralysis
VINDICATE (Differential Diagnosis)
Vascular
Infectious
Neoplastic
Drugs/Degenerative
Inflammatory/Idiopathic
Congenital
Autoimmune
Trauma/Toxic
Endocrine
Quick Reference Values
Shock Classification:
Class I: <15% blood loss
Class II: 15-30% blood loss
Class III: 30-40% blood loss
Class IV: >40% blood loss
Burn Assessment:
Rule of 9s for adults
First 24 hours: 4ml/kg/% burn (Parkland formula)
Escharotomy indications: circumferential burns
Practice Questions and Mock Tests
Question Sources
High-Yield Practice Materials:
INICET previous year papers (2019-2025)
AIIMS entrance question banks
Specialty-specific MCQ collections
Image-based question sets
Mock Test Strategy:
Weekly full-length mocks in final 2 months
Subject-wise tests for targeted improvement
Timed sectional tests for speed building
Analysis of incorrect answers mandatory
Performance Tracking
Metrics to Monitor:
Overall accuracy percentage
Time per question trends
Subject-wise performance
Improvement over time
Weak Area Identification:
Questions consistently getting wrong
Topics taking too long to solve
Image interpretation difficulties
Clinical decision-making gaps
Review and Revision
Daily Review Schedule:
Morning: High-yield facts review (30 minutes)
Post-practice: Wrong question analysis (45 minutes)
Evening: Classification and procedure review (30 minutes)
Weekly Targets:
Complete 200-250 surgery questions
Review 2-3 major topics thoroughly
Analyze trends in mock test performance
Update revision notes with new concepts
Build your foundation with our orthopedic trauma lessons and reinforce concepts with fracture management questions. Our surgery flashcards help you memorize key classifications and procedures efficiently.
Frequently Asked Questions
How many surgery questions appear in INICET?
INICET 2026 typically includes 45-50 surgery and orthopedics questions out of 200 total questions. Surgery accounts for roughly 30-35 questions, while orthopedics contributes 15-20 questions. This represents about 25% of your total paper.
Which fracture classification is most important for INICET?
Garden classification for femoral neck fractures appears most frequently, followed by Neer classification for proximal humerus fractures. AO/OTA classification knowledge helps with general fracture terminology. Focus your memorization time on Garden stages and their management implications.
Should I memorize all surgical procedures step-by-step?
No. INICET tests clinical decision-making, not operative technique details. Focus on indications, contraindications, and immediate post-operative management rather than step-by-step procedural details. Know when to operate, not how to operate.
How much orthopedics should I study for INICET surgery?
Orthopedics questions in INICET focus heavily on trauma and fracture management. Spend 40% of your orthopedics time on trauma, 30% on common fractures and their classifications, and 30% on joint disorders and infections. Skip low-yield topics like sports medicine details.
What's the best way to approach image-based surgery questions?
Follow a systematic approach: identify the imaging modality, locate anatomical landmarks, identify obvious abnormalities, correlate with clinical information provided, and apply relevant classification systems. Practice with actual INICET images rather than textbook illustrations.
How do I improve my speed on surgery questions?
Pattern recognition is key. Practice identifying question stems that signal specific answer approaches. "Most appropriate next step" usually asks for immediate management. "Most likely diagnosis" focuses on key clinical features. Build mental templates for common scenarios through repeated practice.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for INICET success. Download free on Android and iOS.