Back
How to Study Endocrinology for NEET PG 2026: High-Yield Topics, Hormone Axes and Exam Strategy
Master endocrinology for NEET PG 2026 with our comprehensive guide covering thyroid disorders, diabetes mellitus, pituitary gland, adrenal conditions, hormone axes, and proven exam strategies.

How to Study Endocrinology for NEET PG 2026: High-Yield Topics, Hormone Axes and Exam Strategy
You are probably staring at a 500-page endocrinology textbook right now, wondering how to memorize every hormone, receptor, and feedback loop before NEET PG 2026. Here's the thing — endocrinology makes up 8-10% of NEET PG questions, and most students overcomplicate it. The key is understanding patterns, not memorizing every detail.
NEET PG typically includes 16-20 endocrinology questions out of 200 total. These questions follow predictable patterns: hormone axes, clinical scenarios, lab interpretations, and emergency management. The highest-yield topics are diabetes mellitus (30% of endo questions), thyroid disorders (25%), and pituitary-adrenal axis (20%). Master these three areas, and you've secured 75% of endocrinology marks.
Recent NEET PG patterns show increased emphasis on clinical vignettes over pure recall. Questions now integrate endocrinology with other specialties — a diabetic patient with cardiac complications, thyroid storm in pregnancy, or Cushings syndrome presenting as psychiatric symptoms. This shift means your study strategy needs to focus on pattern recognition and differential diagnosis, not isolated facts.
The secret to endocrinology mastery lies in understanding three fundamental concepts: feedback loops, temporal patterns, and compensatory mechanisms. Once you grasp these, the entire subject becomes predictable. Here's your complete roadmap to conquering endocrinology for NEET PG 2026.
Understanding Hormone Axes: The Foundation of Endocrinology
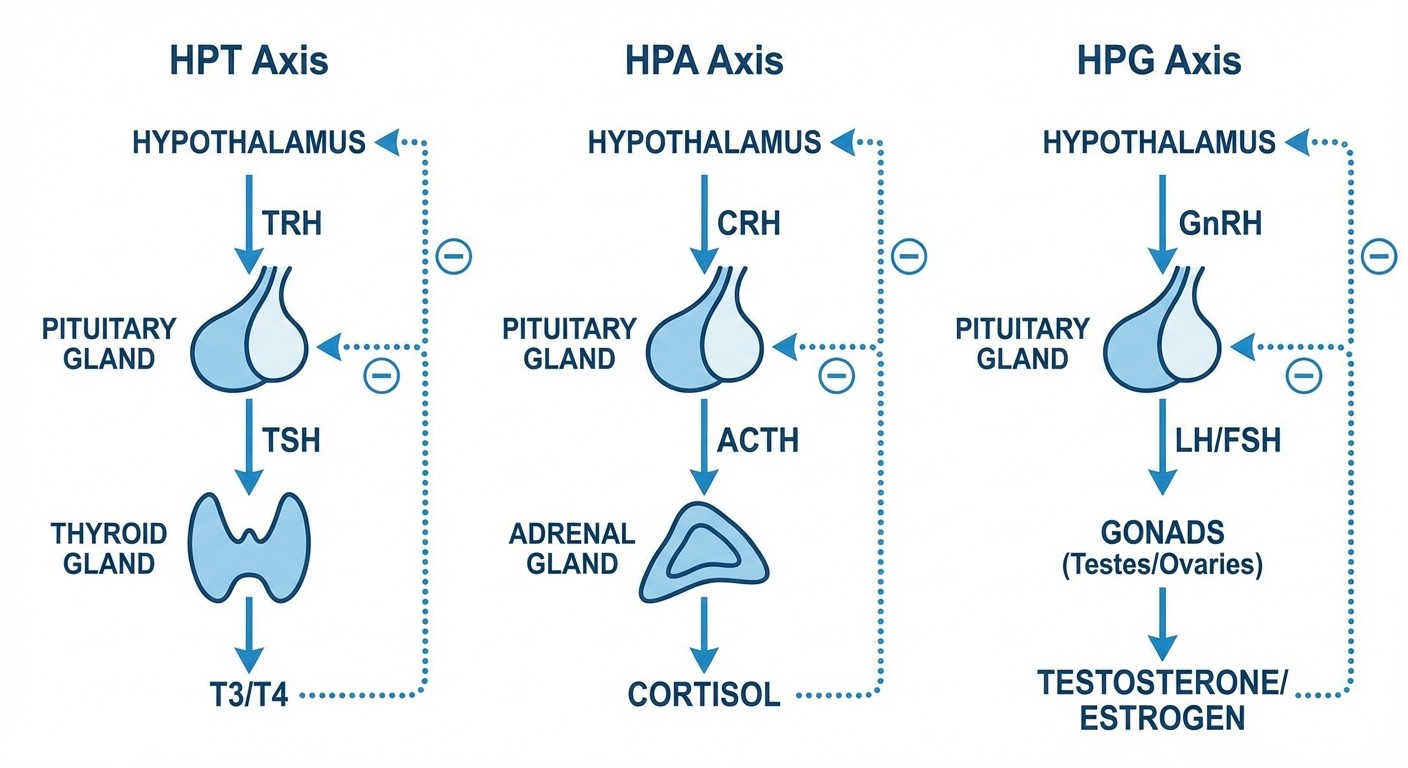
Every endocrine disorder stems from disruption in one of three major axes: hypothalamic-pituitary-thyroid (HPT), hypothalamic-pituitary-adrenal (HPA), or hypothalamic-pituitary-gonadal (HPG). Master these axes, and you'll solve 70% of endocrinology questions without memorizing individual facts.
The HPT Axis: Your Thyroid Roadmap
The HPT axis follows a simple pattern: TRH → TSH → T4/T3. When this axis breaks, you get predictable lab patterns. Primary hypothyroidism shows high TSH with low T4, while secondary hypothyroidism shows low TSH with low T4. NEET PG loves testing this distinction through clinical vignettes.
Central hypothyroidism (pituitary cause) presents with fatigue but normal or low TSH — this catches many students off-guard. Remember the mnemonic "Central = TSH Can't rise" to differentiate from primary thyroid failure. When you encounter thyroid function tests in questions, always check TSH first, then T4, finally T3 if needed.
The adaptive question bank on Oncourse lets you drill thyroid function test interpretation with topic-filtered practice. Students can isolate weak areas like distinguishing subclinical hypothyroidism from sick euthyroid syndrome and practice until the patterns become automatic.
The HPA Axis: Stress Response Mastery
The HPA axis (CRH → ACTH → cortisol) governs stress response and glucose metabolism. Primary adrenal insufficiency (Addisons) shows high ACTH with low cortisol, while secondary adrenal insufficiency shows low ACTH with low cortisol. The dexamethasone suppression test distinguishes Cushings causes by suppression patterns.
Cushings syndrome patterns are high-yield: pituitary adenoma (Cushings disease) suppresses with high-dose dexamethasone, adrenal adenoma doesnt suppress at all, and ectopic ACTH syndrome partially suppresses. Practice these suppression patterns until you can predict the diagnosis from lab values alone.
The HPG Axis: Reproductive Hormones
The HPG axis (GnRH → LH/FSH → sex hormones) creates predictable patterns in reproductive disorders. Primary hypogonadism shows high LH/FSH with low testosterone/estrogen, while secondary hypogonadism shows low LH/FSH with low sex hormones. NEET PG frequently tests PCOS, which shows elevated LH:FSH ratio (>2:1) with high androgens.
High-Yield Endocrinology Topics for NEET PG 2026
Diabetes Mellitus: 30% of Endocrinology Questions
Diabetes questions focus on complications, emergency management, and drug mechanisms. Type 1 diabetes markers include GAD antibodies (most persistent), islet cell antibodies, and zinc transporter 8 antibodies. Type 2 diabetes diagnosis requires fasting glucose ≥126 mg/dL, random glucose ≥200 mg/dL, or HbA1c ≥6.5%.
DKA management follows a strict protocol: fluids first (normal saline), then insulin (0.1 units/kg/hour), then potassium replacement when levels drop below 5.5 mEq/L. The anion gap closes before glucose normalizes — dont stop insulin early. HHS presents with severe dehydration (glucose >600 mg/dL) but minimal ketosis.
Diabetic complications follow predictable timelines: retinopathy appears after 5-10 years, nephropathy after 10-15 years, and neuropathy varies widely. Screening recommendations are high-yield: annual dilated eye exams starting 5 years after Type 1 diagnosis, immediate screening for Type 2 diabetes. The flashcard decks on Oncourse cover these screening timelines with spaced repetition, surfacing forgotten protocols at optimal intervals during your 4-6 week revision period.
Thyroid Disorders: Clinical Pattern Recognition
Thyroid disorders present with classic patterns that NEET PG tests repeatedly. Hyperthyroidism causes weight loss, palpitations, and heat intolerance, while hypothyroidism causes weight gain, fatigue, and cold intolerance. The key is recognizing subtle presentations like subclinical thyroid disease or sick euthyroid syndrome.
Graves disease shows diffuse goiter, exophthalmos, and pretibial myxedema. The TSI (thyroid-stimulating immunoglobulins) remain elevated even after treatment, explaining why patients can relapse. Toxic multinodular goiter typically affects older patients and lacks the eye signs of Graves disease.
Thyroid storm requires immediate recognition: temperature >101°F, tachycardia >140 bpm, altered mental status, and precipitating factor (infection, surgery, iodine exposure). Treatment follows PTU → propranolol → prednisolone → potassium iodide sequence. Remember: PTU blocks new hormone synthesis AND peripheral conversion, making it superior to methimazole in thyroid storm.
Pituitary Disorders: Mass Effects and Hormone Deficiency
Pituitary adenomas cause problems through mass effects (visual field defects, headaches) or hormone excess/deficiency. The visual field defect pattern is diagnostic: bitemporal hemianopia suggests chiasmal compression from pituitary mass. Prolactinomas are the most common functioning adenomas, causing amenorrhea-galactorrhea in women and erectile dysfunction in men.
Acromegaly results from excess growth hormone, usually from pituitary adenoma. Clinical features develop slowly: enlarged hands and feet, coarse facial features, macroglossia, and sleep apnea. IGF-1 levels correlate better with disease activity than random GH levels. The glucose tolerance test remains the gold standard for diagnosis — GH should suppress below 1 ng/mL after glucose load.
Diabetes insipidus presents with polyuria (>3L/day) and polydipsia. Central DI responds to desmopressin, while nephrogenic DI doesnt. The water deprivation test distinguishes these: urine osmolality rises with desmopressin in central DI but remains low in nephrogenic DI.
Adrenal Disorders: Recognize the Syndromes
Primary adrenal insufficiency (Addisons disease) presents with fatigue, weight loss, hyperpigmentation, and salt craving. The hyperpigmentation occurs because high ACTH cross-reacts with melanocyte-stimulating hormone receptors. Lab findings show hyponatremia, hyperkalemia, and low cortisol with high ACTH.
Secondary adrenal insufficiency (pituitary cause) lacks the mineralocorticoid deficiency, so you won't see hyperkalemia or hyperpigmentation. These patients can maintain blood pressure but cant handle stress. The cosyntropin stimulation test confirms the diagnosis when cortisol fails to rise above 20 μg/dL after ACTH injection.
Cushings syndrome clinical features include central obesity, purple striae, easy bruising, and psychiatric changes. The overnight dexamethasone suppression test serves as initial screening — cortisol should suppress below 1.8 μg/dL in normal individuals. When studying these suppression patterns, Oncourse's performance analytics show which hormone axis you're struggling with, then provides a curated study path to address those specific gaps.
Conns syndrome (primary hyperaldosteronism) causes hypertension with hypokalemia. The aldosterone:renin ratio above 20 suggests the diagnosis. Remember that beta-blockers and ACE inhibitors interfere with renin measurements, so patients need medication adjustments before testing.
Calcium and Bone Metabolism: PTH Relationships
Primary hyperparathyroidism shows high calcium, low phosphorus, and high PTH. Secondary hyperparathyroidism (usually from vitamin D deficiency or CKD) shows low calcium, high phosphorus, and high PTH. Tertiary hyperparathyroidism occurs in CKD patients when parathyroid glands become autonomous, showing high calcium with persistently high PTH.
Vitamin D deficiency is increasingly common and often missed. Symptoms include bone pain, muscle weakness, and increased fracture risk. 25-hydroxyvitamin D levels below 20 ng/mL indicate deficiency. Treatment requires both vitamin D replacement and adequate calcium intake.
Creating Your Study Schedule: 8-Week Endocrinology Plan
Weeks 1-2: Foundation Building
Start with hormone axes and feedback loops. Spend 2 hours daily on basic concepts: hypothalamic-pituitary relationships, negative feedback mechanisms, and hormone classifications. Use active recall — draw hormone pathways from memory, then check your accuracy. This foundation prevents confusion later when studying individual disorders.
Focus on understanding rather than memorization. For example, instead of memorizing that "T4 half-life is 7 days," understand that this long half-life explains why thyroid replacement therapy takes 6-8 weeks to reach steady state. This conceptual approach helps you answer application questions, not just recall questions.
Weeks 3-4: High-Yield Topics Deep Dive
Dedicate week 3 to diabetes and thyroid disorders, week 4 to pituitary and adrenal conditions. Study 3-4 hours daily, alternating between reading and practice questions. For each condition, master the triad: pathophysiology, clinical presentation, and diagnostic approach.
Create comparison charts for similar conditions. For instance, compare primary vs secondary vs tertiary hyperparathyroidism in a table format. This visual organization helps during exam recall when you need to quickly differentiate conditions based on lab values.
Weeks 5-6: Integration and Clinical Scenarios
Practice interpreting lab values and clinical vignettes. NEET PG questions rarely test isolated facts — they present scenarios requiring diagnosis and management decisions. Spend time on mixed endocrine cases: diabetic patients with thyroid disease, pregnant women with Graves disease, or elderly patients with multiple hormone deficiencies.
Use the Oncourse question bank during this phase to practice topic-filtered questions. When you miss questions about Cushings vs Conns syndrome, the platform tracks this weakness and includes similar questions in future sessions until mastery is achieved.
Weeks 7-8: Revision and Weak Areas
Focus exclusively on your weak topics identified through practice tests. Use spaced repetition for hormone values, normal ranges, and drug doses. Create mnemonics for complex protocols like DKA management or thyroid storm treatment.
Review high-yield facts daily: diabetes screening guidelines, thyroid cancer staging, emergency management protocols. These factual details often determine correct answers in borderline questions.
Exam Strategy: Approaching Endocrinology Questions
Pattern Recognition Over Memorization
NEET PG endocrinology questions follow predictable patterns. Learn to recognize question types instantly: "A 45-year-old woman with weight gain and purple striae" signals Cushings syndrome. "A young man with visual field defects and galactorrhea" suggests prolactinoma with mass effects.
Practice the two-step approach: identify the syndrome first, then determine the specific cause. For thyrotoxicosis, first recognize hyperthyroidism from clinical features, then use additional clues (eye signs, goiter characteristics, age) to distinguish Graves disease from toxic multinodular goiter.
Lab Value Interpretation
Master the common lab patterns before exam day. Create quick reference cards for:
TSH/T4 combinations in thyroid disorders
Cortisol/ACTH patterns in adrenal conditions
Calcium/PTH relationships in parathyroid disease
Glucose/insulin dynamics in diabetes
When you see lab values in questions, resist the urge to calculate ratios or conversions. Focus on the pattern: is TSH high or low relative to T4? Is ACTH suppressed or elevated relative to cortisol? This pattern recognition approach saves time and reduces calculation errors.
Emergency Management Protocols
Endocrine emergencies require rapid recognition and systematic management. For DKA, remember the sequence: assess severity (pH, mental status), start fluids (normal saline initially), begin insulin after confirming potassium >3.3 mEq/L, monitor for complications (cerebral edema in children, hypokalemia in adults).
For thyroid storm, the mnemonic "PTU Plus Propranolol Plus Prednisolone Plus Potassium iodide" covers the four-drug approach. Start PTU first (blocks synthesis and conversion), add propranolol for symptom control, give prednisolone for stress coverage, then potassium iodide to block hormone release.
Common Mistakes to Avoid
Overthinking Simple Questions
Students often miss straightforward questions by overanalyzing. If a question describes classic diabetic ketoacidosis — young patient, polyuria, fruity breath odor, high glucose, positive ketones — the answer is DKA management. Dont search for rare complications or alternative diagnoses.
Similarly, when you see bitemporal hemianopia with galactorrhea, think prolactinoma causing chiasmal compression. The zebra diagnoses (craniopharyngioma, meningioma) are mentioned to distract you, but NEET PG typically tests common conditions with classic presentations.
Confusing Primary vs Secondary Disorders
The primary vs secondary distinction trips up many students. Remember: primary means the problem is in the target gland itself, secondary means the problem is in the pituitary control system. Primary hypothyroidism has a sick thyroid gland (high TSH trying to stimulate it), while secondary hypothyroidism has a sick pituitary (low TSH unable to stimulate a normal thyroid).
Use the feedback loop logic: if the gland is sick, the controlling hormone rises trying to compensate (primary disorder). If the controller is sick, both the controlling hormone and target hormone fall together (secondary disorder).
Ignoring Clinical Context
Lab values mean nothing without clinical context. A slightly elevated TSH in an elderly patient with no symptoms might represent normal aging, while the same TSH in a young woman with fatigue suggests early hypothyroidism. Always correlate lab findings with clinical presentation.
Similarly, mild hyperglycemia during acute illness (stress hyperglycemia) doesnt equal diabetes mellitus. Look for supporting evidence: previous elevated values, classic symptoms, or diabetes complications before making the diagnosis.
Frequently Asked Questions
How many endocrinology questions appear in NEET PG 2026?
NEET PG 2026 typically includes 16-20 endocrinology questions out of 200 total questions, representing 8-10% of the exam. The distribution favors diabetes mellitus (30% of endo questions), thyroid disorders (25%), pituitary disorders (20%), adrenal disorders (15%), and calcium metabolism (10%).
Which endocrinology topics are highest yield for NEET PG?
Focus on diabetes mellitus complications and management, thyroid function test interpretation, pituitary adenoma presentations, Cushings vs Addisons syndrome differentiation, and endocrine emergency protocols. These five areas account for 75% of endocrinology questions in recent NEET PG exams.
How should I approach hormone axis questions?
Always start by identifying which axis is involved (HPT, HPA, or HPG), then determine if the problem is primary (target gland) or secondary (pituitary). Use the feedback loop principle: primary disorders show high controlling hormone with low target hormone, while secondary disorders show both hormones low together.
What are the most commonly tested lab value patterns?
Master these patterns: primary hypothyroidism (high TSH, low T4), secondary hypothyroidism (low TSH, low T4), primary hyperparathyroidism (high calcium, high PTH), secondary hyperparathyroidism (low calcium, high PTH), Cushings syndrome (high cortisol, low ACTH if adrenal cause), and Addisons disease (low cortisol, high ACTH).
How much time should I spend on endocrinology daily?
During dedicated preparation, allocate 2-3 hours daily to endocrinology for 8 weeks. Spend 60% of time on high-yield topics (diabetes, thyroid, pituitary), 30% on practice questions, and 10% on revision of weak areas identified through testing.
Should I memorize normal hormone values?
Yes, but focus on clinically relevant ranges: TSH (0.4-4.0 mIU/L), fasting glucose (<100 mg/dL normal, 100-125 mg/dL prediabetes, ≥126 mg/dL diabetes), HbA1c (<5.7% normal, 5.7-6.4% prediabetes, ≥6.5% diabetes), and calcium (8.5-10.5 mg/dL). These ranges appear frequently in NEET PG questions.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS