FMGE Physiology High Yield Topics 2026: Complete Subject Guide
Master FMGE physiology with this definitive 2026 guide covering high-yield topics, weightage breakdown, and exam-ready mechanisms. Score higher with targeted preparation.
FMGE Physiology High Yield Topics 2026: Complete Subject Guide
You are probably staring at the 2,000-page physiology textbook wondering where to even start. FMGE 2026 has 300 questions across all subjects, with physiology accounting for roughly 35-40 questions. That means you have 63 seconds per question and zero room for confusion about mechanisms.
Here's the reality: physiology questions in FMGE test specific numerical values, mechanism sequences, and conceptual applications. They dont ask you to regurgitate Guyton's entire chapter on renal function. They want you to know that normal GFR is 120-130 ml/min, recognize the JG apparatus mechanism in 15 seconds, and connect aldosterone action to clinical scenarios.
This guide breaks down the highest-yield physiology topics for FMGE 2026, ranked by frequency in past papers and weighted by exam importance. Every topic here has appeared in at least 3 of the last 5 FMGE cycles.
FMGE Physiology Weightage Breakdown 2026
System | Questions per Exam | Weightage (%) | Must-Know Topics |
|---|---|---|---|
Cardiovascular | 8-10 | 25% | Cardiac cycle, ECG, heart sounds |
Respiratory | 6-8 | 20% | Lung volumes, V/Q ratio, gas transport |
Renal | 5-7 | 18% | GFR, tubular function, acid-base |
Endocrine | 4-6 | 15% | Thyroid, insulin, adrenal hormones |
GI | 3-4 | 10% | Gastric secretion, GI hormones |
CNS | 2-3 | 7% | Cerebellar functions, sleep |
General/Blood | 2-3 | 5% | Membrane transport, coagulation |
High-Yield Cardiovascular Physiology
Cardiac Cycle and Hemodynamics
The cardiac cycle generates 8-10 questions per FMGE exam because it connects anatomy, physiology, and clinical correlations. Focus on these pressure changes and valve timings:
Systolic Phase Events:
Isovolumetric contraction: all valves closed, pressure rises from 8 mmHg to 80 mmHg
Ejection phase: aortic valve opens, stroke volume = 70ml ejected
Peak systolic pressure: 120 mmHg in healthy adults
Diastolic Phase Events:
Isovolumetric relaxation: pressure drops from 80 mmHg to 8 mmHg
Filling phase: mitral valve opens, ventricular filling 70% passive
End-diastolic volume: 120-130ml (preload determinant)
FMGE loves asking about Starling's law applications. The key insight: increased preload stretches myocardial fibers, increasing contractility up to a physiological limit. Beyond that, heart failure mechanics kick in.
Practice identifying heart sounds with their cardiac cycle correlations using Oncourse's cardiovascular system lessons and reinforce the timing relationships with targeted cardiovascular physiology questions.
ECG Interpretation Essentials
Every FMGE cycle tests ECG wave correlations:
P wave: atrial depolarization (0.08-0.1 sec duration)
QRS complex: ventricular depolarization (0.06-0.1 sec)
T wave: ventricular repolarization
PR interval: 0.12-0.2 sec (AV conduction time)
QT interval: 0.35-0.45 sec (total ventricular activity)
High-yield abnormalities: prolonged QT (>0.45 sec), shortened PR (<0.12 sec suggesting WPW), and QRS widening (>0.12 sec indicating bundle branch issues).
JVP Waveform Analysis
Jugular venous pressure waveforms appear in 2-3 questions per exam:
a wave: atrial contraction against closed tricuspid valve
c wave: tricuspid valve closure during isovolumetric contraction
v wave: atrial filling against closed tricuspid valve
x descent: atrial relaxation
y descent: tricuspid valve opening
Remember: elevated JVP suggests right heart failure, while giant v waves indicate tricuspid regurgitation.
High-Yield Respiratory Physiology
Lung Volumes and Capacities
FMGE tests specific numerical values. Memorize these exact numbers:
Parameter | Normal Value | Clinical Significance |
|---|---|---|
Tidal Volume (TV) | 500 ml | Resting breath volume |
Inspiratory Reserve (IRV) | 3000 ml | Deep inspiration capacity |
Expiratory Reserve (ERV) | 1100 ml | Forced expiration reserve |
Residual Volume (RV) | 1200 ml | Air remaining after max expiration |
Vital Capacity | 4600 ml | TV + IRV + ERV |
Total Lung Capacity | 5800 ml | All lung volumes combined |
FEV1 | 80% of FVC | Airway obstruction marker |
Clinical correlations tested: restrictive disease reduces all volumes proportionally, while obstructive disease increases RV and reduces FEV1/FVC ratio.
Ventilation-Perfusion (V/Q) Relationships
This topic generates 3-4 questions per exam. Master these zone concepts:
Zone 1 (Apical): V/Q = 3.3 (high ventilation, low perfusion)
Dead space physiology dominates
Minimal gas exchange efficiency
Zone 2 (Middle): V/Q = 1.0 (ideal matching)
Optimal gas exchange region
Most efficient oxygen uptake
Zone 3 (Basal): V/Q = 0.6 (low ventilation, high perfusion)
Shunt physiology develops
Reduced oxygen saturation
Understanding V/Q mismatches helps with interpreting ABG abnormalities and pulmonary pathology questions that frequently follow physiology topics in FMGE.
Oxygen and CO2 Transport Mechanisms
Oxygen Transport:
Dissolved O2: 3% (0.3 ml O2/100ml blood)
Hemoglobin-bound: 97% (19.7 ml O2/100ml blood)
P50 value: 27 mmHg (hemoglobin 50% saturated)
CO2 Transport:
Dissolved CO2: 7%
Carbaminohemoglobin: 23%
Bicarbonate: 70% (chloride shift in RBCs)
The carbonic anhydrase reaction (CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3-) appears in multiple question formats. When practicing respiratory mechanisms, Oncourse flashcards encode these transport sequences as step-by-step chains, helping you retain the multi-stage processes that FMGE loves to test in different ways.
High-Yield Renal Physiology
Glomerular Filtration Rate (GFR) and Filtration
GFR calculations appear in every FMGE exam:
Normal GFR: 120-130 ml/min (males), 90-120 ml/min (females) Filtration fraction: GFR/RPF = 20% (normal kidneys filter 20% of plasma flowing through) Starling forces affecting filtration:
Glomerular hydrostatic pressure: +60 mmHg (favors filtration)
Bowman's capsule pressure: -15 mmHg (opposes filtration)
Plasma oncotic pressure: -29 mmHg (opposes filtration)
Net filtration pressure: +16 mmHg
Auto-regulation mechanisms:
Tubuloglomerular feedback: macula densa cells detect high NaCl, release adenosine to constrict afferent arteriole
Myogenic response: afferent arteriole constricts with increased pressure
Tubular Reabsorption and Secretion
Focus on specific transport percentages and mechanisms:
Proximal Tubule (65% of filtrate reabsorbed):
Na+/K+-ATPase drives all reabsorption
Glucose: 100% reabsorbed (threshold = 180 mg/dl)
Amino acids: 100% reabsorbed
Bicarbonate: 80% reabsorbed via carbonic anhydrase
Loop of Henle:
Thin ascending limb: passive NaCl reabsorption
Thick ascending limb: Na+/K+/2Cl- cotransporter (furosemide target)
Creates medullary concentration gradient (300-1200 mOsm)
Distal Tubule and Collecting Duct:
Aldosterone increases ENaC channels for Na+ reabsorption
ADH increases aquaporin-2 for water reabsorption
Principal cells vs intercalated cells (acid-base regulation)
Hormonal Regulation: Aldosterone and ADH
Aldosterone mechanism:
1. Low Na+ or high K+ stimulates aldosterone release
2. Binds mineralocorticoid receptors in principal cells
3. Increases ENaC and Na+/K+-ATPase synthesis
4. Result: Na+ retention, K+ loss
ADH (Vasopressin) mechanism:
1. High plasma osmolality (>295 mOsm) or low blood volume triggers release
2. Binds V2 receptors on basolateral membrane
3. Activates cAMP → PKA → phosphorylates aquaporin-2
4. Result: water reabsorption increases, urine concentrates
FMGE often tests diabetes insipidus (ADH deficiency) vs SIADH (excess ADH) scenarios requiring you to predict urine osmolality changes.
High-Yield Endocrine Physiology
Thyroid Hormone Regulation
The HPT (hypothalamic-pituitary-thyroid) axis generates consistent FMGE questions:
Hormone cascade:
TRH → TSH → T4/T3 → Negative feedback
T4 vs T3 characteristics:
T4: inactive form, 90% of thyroid secretion, longer half-life (7 days)
T3: active form, 10% direct secretion + peripheral conversion, shorter half-life (1.5 days)
5'-deiodinase converts T4 → T3 in target tissues
Physiological effects tested:
Metabolic: increases BMR, O2 consumption, heat production
Cardiovascular: increases heart rate, contractility, cardiac output
Growth: essential for normal CNS development (cretinism if deficient)
Clinical correlations: primary vs secondary hypothyroidism based on TSH levels (high vs low TSH respectively).
Insulin and Glucagon Mechanisms
Glucose homeostasis questions appear 2-3 times per FMGE exam:
Insulin actions:
Glucose uptake: increases GLUT4 translocation in muscle/adipose
Glycogen synthesis: activates glycogen synthase
Lipogenesis: acetyl-CoA → fatty acid synthesis
Protein synthesis: activates mTOR pathway
Glucagon actions:
Glycogenolysis: activates glycogen phosphorylase
Gluconeogenesis: activates PEPCK, G6Pase enzymes
Lipolysis: hormone-sensitive lipase activation
Ketogenesis: acetyl-CoA → ketone body production
Regulation patterns:
Fed state: insulin dominates, anabolic pathways active
Fasted state: glucagon dominates, catabolic pathways active
Exercise: both hormones coordinate glucose supply to muscles
Understanding these opposing actions helps answer complex scenarios about metabolic syndrome, diabetes management, and exercise physiology that frequently connect to insulin resistance concepts.
Adrenal Cortex and Medulla Function
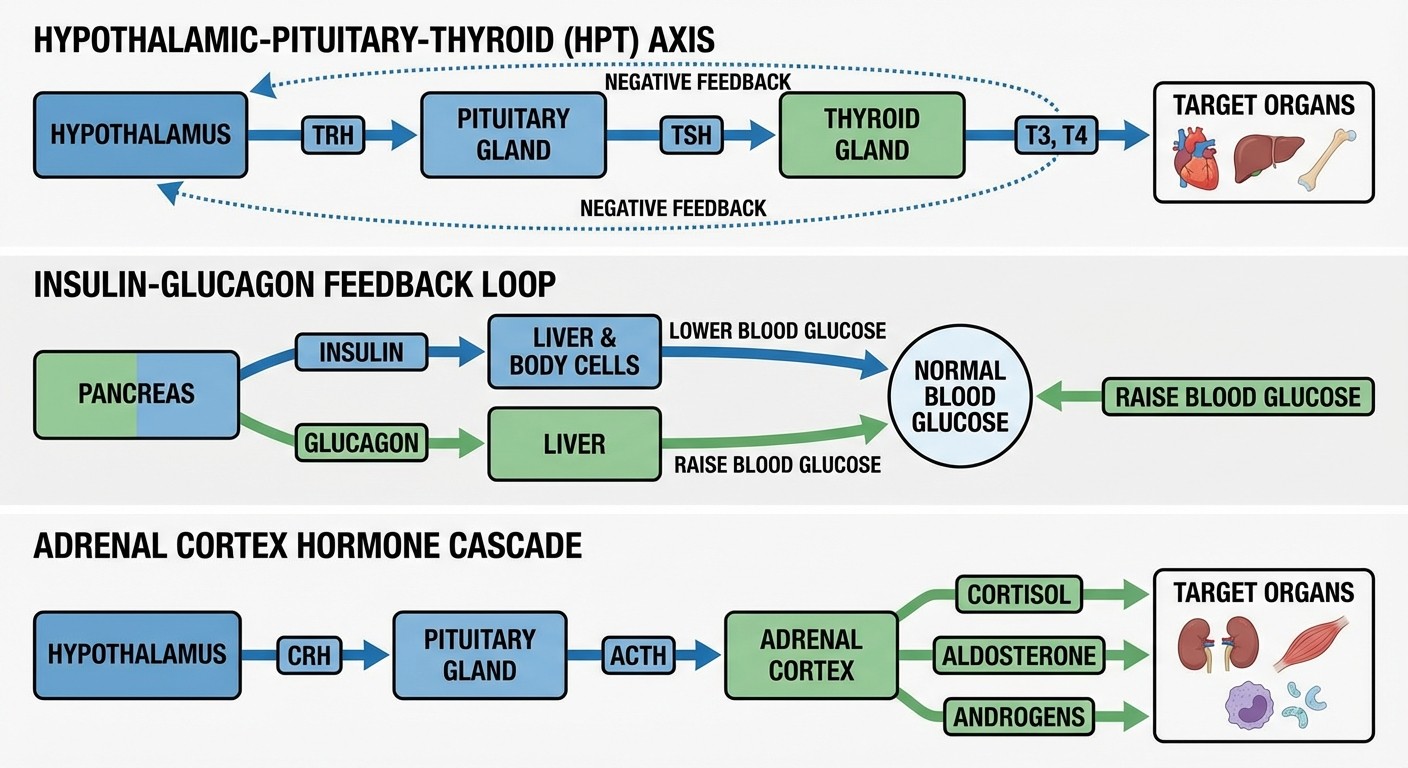
Adrenal Cortex (Steroid Hormones):
Zona glomerulosa: aldosterone (mineralocorticoid)
Zona fasciculata: cortisol (glucocorticoid)
Zona reticularis: androgens (DHEA, androstenedione)
Cortisol physiology:
Circadian rhythm: peak at 8 AM, lowest at midnight
Stress response: increases gluconeogenesis, anti-inflammatory
Negative feedback: inhibits CRH and ACTH release
Adrenal Medulla (Catecholamines):
Epinephrine: 80% of medullary secretion
Norepinephrine: 20% of medullary secretion
Fight-or-flight response: increases heart rate, blood pressure, glucose
High-Yield GI Physiology
Gastric Acid Secretion Control
Gastric physiology generates 3-4 FMGE questions focusing on regulatory mechanisms:
Three phases of gastric secretion: 1. Cephalic phase (30%): sight/smell/taste → vagal stimulation → acetylcholine release 2. Gastric phase (60%): gastric distension + amino acids → gastrin release 3. Intestinal phase (10%): duodenal amino acids → intestinal gastrin Parietal cell acid secretion:
H+/K+-ATPase (proton pump) exchanges H+ for K+
Carbonic anhydrase: CO2 + H2O → H+ + HCO3-
Stimulation: acetylcholine (M3), gastrin (CCK-B), histamine (H2)
Inhibition: somatostatin, prostaglandins (PGE2)
GI Hormone Functions
Master these hormone actions for guaranteed FMGE points:
Gastrin:
Source: G cells in gastric antrum
Stimulus: amino acids, gastric distension
Actions: stimulates gastric acid, pepsinogen secretion
Secretin:
Source: S cells in duodenum
Stimulus: acidic chyme (pH < 4.5)
Actions: stimulates pancreatic bicarbonate, inhibits gastric acid
CCK (Cholecystokinin):
Source: I cells in duodenum/jejunum
Stimulus: fatty acids, amino acids
Actions: gallbladder contraction, pancreatic enzyme secretion
GIP (Glucose-dependent Insulinotropic Peptide):
Source: K cells in duodenum
Stimulus: glucose, fatty acids
Actions: stimulates insulin release, inhibits gastric emptying
Remember the mnemonic: "Secretin Stops Stomach acid, CCK Contracts gallbladder."
GI Motility Patterns
Esophageal motility:
Primary peristalsis: initiated by swallowing
Secondary peristalsis: response to esophageal distension
Lower esophageal sphincter: tonic contraction prevents reflux
Gastric motility:
Antral grinding: 3 contractions per minute
Migrating motor complex: clears undigested material during fasting
Gastric emptying: liquids empty faster than solids
Small intestinal motility:
Segmentation: mixes chyme with digestive juices
Peristalsis: propels contents aborally
Ileocecal valve: prevents backflow from colon
Understanding motility disorders helps connect physiology to clinical presentations that often follow in FMGE question stems.
High-Yield CNS Physiology
Cerebellar Function and Motor Control
Cerebellar physiology appears in 2-3 questions per FMGE exam:
Functional divisions:
Vestibulocerebellum: balance and eye movements
Spinocerebellum: posture and locomotion
Cerebrocerebellum: motor planning and coordination
Clinical correlations:
Cerebellar lesions: intention tremor, dysmetria, ataxic gait
No paralysis (unlike cerebral motor cortex lesions)
Ipsilateral deficits due to double crossing of pathways
Sleep Physiology and EEG Patterns
Sleep stages and characteristics: NREM Stage 1: 5% of sleep
Light sleep, theta waves (4-8 Hz)
Easily awakened
NREM Stage 2: 45% of sleep
Sleep spindles (12-14 Hz) and K complexes
Moderately deep sleep
NREM Stage 3: 25% of sleep
Slow wave sleep, delta waves (<4 Hz)
Deep sleep, growth hormone release
REM Sleep: 25% of sleep
Rapid eye movements, vivid dreams
Muscle atonia, irregular breathing
Increased after sleep deprivation
Sleep cycle timing:
Total cycle: 90-110 minutes
REM increases toward morning
Slow wave sleep predominates early night
FMGE tests sleep deprivation effects and age-related changes in sleep architecture.
High-Yield Blood and General Physiology
Hemostasis and Coagulation Cascade
Blood physiology generates 2-3 questions focusing on clotting mechanisms:
Primary hemostasis:
1. Vascular spasm: immediate vasoconstriction
2. Platelet plug formation: vWF bridges platelets to collagen
3. Platelet aggregation: ADP and thromboxane A2 amplify response
Secondary hemostasis (coagulation cascade):
Extrinsic pathway: tissue factor + factor VII
Intrinsic pathway: contact activation (factors XII, XI, IX, VIII)
Common pathway: factor X → prothrombin → thrombin → fibrin
Key factors and tests:
PT tests extrinsic pathway (factors VII, X, V, II)
aPTT tests intrinsic pathway (factors XII, XI, IX, VIII)
Factor VIII deficiency: hemophilia A (X-linked)
Factor IX deficiency: hemophilia B (X-linked)
Cell Membrane Transport
General physiology concepts appear in 2-3 questions:
Passive transport:
Simple diffusion: O2, CO2, steroid hormones
Facilitated diffusion: glucose via GLUT transporters
Osmosis: water movement across semipermeable membranes
Active transport:
Primary active: Na+/K+-ATPase, H+/K+-ATPase, Ca2+-ATPase
Secondary active: Na+/glucose cotransporter, Na+/H+ exchanger
Membrane potential:
Resting potential: -70 mV (mainly due to K+ equilibrium)
Action potential: Na+ influx → depolarization → K+ efflux → repolarization
Refractory periods: absolute (Na+ channels inactivated) vs relative
These transport mechanisms connect to every system tested in FMGE, making them extremely high-yield for understanding complex physiological processes.
FMGE Physiology Study Strategy 2026
Topic Prioritization Matrix
Based on past 5 years of FMGE question analysis:
Tier 1 (Must Master - 70% of questions):
Cardiac cycle and ECG interpretation
Lung volumes and V/Q relationships
GFR and renal regulation mechanisms
Thyroid and insulin hormone actions
Gastric acid secretion control
Tier 2 (Important - 20% of questions):
JVP waveforms and heart sounds
Gas transport mechanisms
Aldosterone and ADH functions
GI hormone actions
Sleep physiology
Tier 3 (Lower Yield - 10% of questions):
Cerebellar function details
Blood group genetics
Specialized transport mechanisms
Focus 70% of study time on Tier 1 topics, ensuring you can answer these confidently under exam pressure.
Active Recall Techniques
Traditional physiology study involves reading lengthy explanations and hoping to remember mechanism details. FMGE success requires active recall of specific values, sequences, and correlations.
Effective study approach: 1. Mechanism mapping: Draw pathway diagrams from memory, then verify accuracy 2. Numerical drilling: Practice recalling exact values (GFR = 120 ml/min, not "around 100-150") 3. Clinical correlation: Connect each mechanism to potential FMGE question scenarios
When tackling abstract mechanisms like the JG apparatus or aldosterone regulation, break them into discrete steps and quiz yourself on each component. This builds the rapid recall needed for FMGE's time pressure.
Question-Based Learning Pattern
Pure theory study misses the clinical application style that FMGE emphasizes. After mastering basic mechanisms, shift to question-based reinforcement.
Recommended sequence:
1. Study mechanism from textbook/notes (30 minutes max per topic)
2. Practice topic-specific MCQs immediately (identify knowledge gaps)
3. Review incorrect answers and strengthen weak concepts
4. Repeat practice questions until consistent accuracy
Oncourse's FMGE question bank organizes past paper questions by subtopic, letting you drill cardiovascular physiology separate from respiratory, then combine them in mixed practice sessions. After completing physiology practice sets, check your performance analytics to see exactly which systems need reinforcement before moving to the next subject.
This targeted approach prevents the common mistake of spending equal time on all physiology topics when cardiovascular and respiratory dominate the actual exam.
Frequently Asked Questions
How many physiology questions appear in FMGE 2026?
FMGE typically includes 35-40 physiology questions out of 300 total questions, representing about 12-13% of the exam. Cardiovascular and respiratory systems account for nearly half of these physiology questions.
Which physiology topics are most frequently repeated in FMGE?
Cardiac cycle mechanisms, lung volume calculations, GFR regulation, and thyroid hormone actions appear in every FMGE cycle. ECG interpretation and gastric acid secretion control also show high repeatability across past exams.
Should I memorize all normal physiological values for FMGE?
Yes, FMGE frequently tests specific numerical values like normal GFR (120-130 ml/min), blood pressure (120/80 mmHg), and cardiac output (5 L/min). Create a separate list of all normal values mentioned in this guide for quick review.
How detailed should my understanding of physiology mechanisms be?
Focus on mechanism sequences and rate-limiting steps rather than molecular details. FMGE tests your ability to predict physiological outcomes and clinical correlations, not biochemical pathway minutiae.
Can I score well in physiology without extensive clinical correlation?
While basic mechanisms are essential, FMGE physiology questions increasingly incorporate clinical scenarios. Understanding how physiological abnormalities present clinically significantly improves your answer accuracy and confidence.
What's the best way to retain complex physiological processes?
Use active recall techniques like drawing mechanism diagrams from memory and explaining processes aloud. Spaced repetition of high-yield facts and regular practice testing strengthen long-term retention more effectively than passive reading.
---
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for FMGE. Download free on Android and iOS.