Back
FMGE ENT High Yield Topics 2026 — Complete Preparation Guide for Foreign Medical Graduates
Master FMGE ENT with this comprehensive guide covering high-yield topics like BPPV, cholesteatoma, tympanoplasty, and audiogram interpretation. Includes MCQ patterns and strategies for 2026.

FMGE ENT High Yield Topics 2026 — Complete Preparation Guide for Foreign Medical Graduates
You are probably staring at the FMGE syllabus wondering where to start with ENT. The truth? ENT questions in FMGE follow predictable patterns. 80% of ENT marks come from just 8-10 core topics that repeat year after year.
FMGE allocates roughly 8-12 questions to ENT out of 300 total. That translates to 2.7-4% weightage — small but crucial for your overall score. Each ENT question you nail adds 0.33% to your total. Miss them, and you are handing points to competitors who studied smarter.
The NBE loves testing clinical scenarios over theoretical knowledge. They want to see if you can diagnose BPPV from a case description, not recite the anatomy of semicircular canals. This guide breaks down exactly what they test, how they test it, and the high-yield facts that separate correct answers from attractive distractors.
Core ENT Topics That Dominate FMGE
1. Audiology and Hearing Loss
This cluster appears in 3-4 questions every year. The pattern? Clinical scenarios with audiogram interpretation, tuning fork tests, and hearing aid candidacy.
Key Sub-topics:
SNHL vs CSOM differentiation
Audiogram reading (bone conduction vs air conduction gaps)
Rinne and Weber test combinations
Sudden sensorineural hearing loss management
Noise-induced hearing loss criteria
High-Yield One-Liners:
SNHL shows bone conduction = air conduction on audiogram
CSOM shows air-bone gap >30 dB with normal bone conduction
Rinne negative + Weber lateralizing = conductive hearing loss
Sudden SNHL needs steroids within 72 hours for best outcomes
Industrial noise >85 dB for 8+ hours daily = compensable hearing loss
The smartest approach here is understanding the logic, not memorizing combinations. Oncourse AI Smart Flashcards include pre-loaded FMGE ENT decks that drill audiogram interpretation patterns until the logic becomes automatic — they surface cards based on your weak zones and create targeted revision paths for exactly these audiometry concepts.
2. Vertigo and Balance Disorders
FMGE loves vertigo because it tests both diagnosis and emergency management. Expect 2-3 questions on this cluster annually.
BPPV (Most Tested):
Posterior canal BPPV = most common (85% cases)
Dix-Hallpike positive = rotatory nystagmus with fatigue
Epley maneuver = first-line treatment
Typical duration: seconds to minutes per episode
Meniere Disease vs BPPV:
Meniere = hearing loss + tinnitus + vertigo + ear fullness (4 symptoms)
BPPV = positional vertigo only, no hearing loss
Meniere episodes last hours, BPPV episodes last seconds
Acute Vestibular Neuritis:
Sudden onset severe vertigo lasting days
No hearing loss (vs labyrinthitis which has hearing loss)
Head impulse test positive
Steroids help if started within 72 hours
Practice with FMGE ENT-specific question sets helps nail these distinctions — Oncourse AI Topic Tests include detailed explanations aligned to NBE patterns and help identify exactly which vertigo sub-topics need more revision before your exam.
3. Epistaxis Management
This appears as emergency management scenarios. Know the stepwise approach and when to escalate.
Immediate Management Protocol:
1. Anterior pressure + head forward position (not tilted back)
2. Topical decongestant (oxymetazoline) + cotton pledget
3. If bleeding continues: anterior nasal packing
4. If still bleeding: posterior packing or sphenopalatine artery ligation
Common Causes by Age:
Children: Digital trauma, foreign bodies, allergic rhinitis
Adults: Hypertension, anticoagulants, hereditary hemorrhagic telangiectasia
Elderly: Anticoagulation, atherosclerosis, nasal dryness
Red Flags for Referral:
Bilateral epistaxis (think systemic bleeding disorder)
Recurrent unilateral epistaxis (rule out malignancy)
Epistaxis with facial numbness (think nasopharyngeal carcinoma)
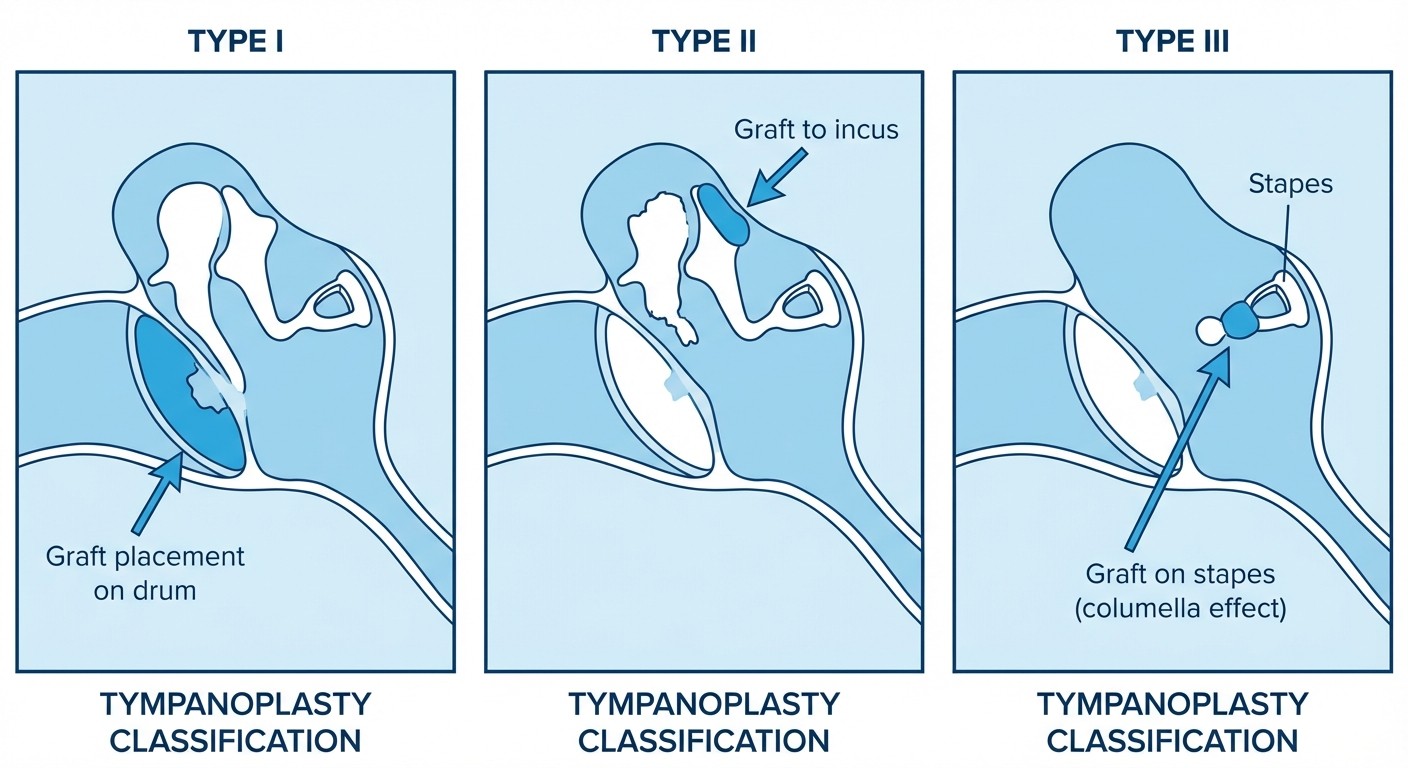
4. Tympanoplasty Classification
FMGE tests this through case scenarios describing tympanic membrane perforation patterns and asking about surgical approach.
Wullstein Classification:
Type I: Myringoplasty (intact ossicular chain)
Type II: Malleus handle missing (graft to incus/stapes)
Type III: Only stapes intact (graft to stapes head = columella effect)
Type IV: Stapes footplate only (fenestration procedure)
Type V: Fixed stapes footplate (fenestra nova)
Clinical Correlations:
Central perforation + intact margins = Type I candidate
Marginal perforation + ossicular erosion = evaluate for Type II/III
Cholesteatoma cases = often need Type III reconstruction
The key trick? FMGE rarely asks about Type IV/V directly. Focus on Types I-III which cover 90% of real clinical scenarios. When you see a case with "central perforation, intact ossicles," think Type I myringoplasty.
5. Nasal Polyps and Rhinosinusitis
This cluster tests both medical and surgical management decisions. Common in FMGE because it bridges ENT with allergy/immunology concepts.
Nasal Polyp Types:
Antrochoanal polyp (unilateral, originates from maxillary sinus)
Ethmoidal polyps (bilateral, associated with asthma/aspirin sensitivity)
Sphenochoanal polyp (rare, originates from sphenoid sinus)
Key Clinical Associations:
Aspirin-exacerbated respiratory disease (AERD) = nasal polyps + asthma + aspirin sensitivity
Cystic fibrosis patients = high risk for nasal polyps
Allergic fungal sinusitis = thick eosinophilic mucin + polyps
Management Steps:
1. Medical: Topical steroids (first-line for bilateral polyps)
2. Surgical: FESS (functional endoscopic sinus surgery) for failed medical therapy
3. Post-op: Long-term topical steroids prevent recurrence
FMGE Trap: Unilateral nasal polyp in adult = rule out malignancy first. Dont jump to steroid treatment without histopathology.
6. Cholesteatoma
This tests surgical decision-making and complication recognition. FMGE loves cholesteatoma because it can present as emergency scenarios.
Clinical Presentation Pattern:
Foul-smelling otorrhea (pathognomonic)
Conductive hearing loss
Retraction pocket or marginal perforation
White flaky debris in ear canal
Complications (High-Yield for FMGE):
Facial nerve palsy (most common neurologic complication)
Labyrinthitis (sensorineural hearing loss + vertigo)
Meningitis (intracranial spread through tegmen)
Brain abscess (temporal lobe, cerebellar)
Surgical Principles:
Canal wall up vs canal wall down mastoidectomy
Complete cholesteatoma removal = priority over hearing preservation
Second-look surgery often needed to confirm complete removal
When tracking your ENT performance across multiple practice sessions, Oncourse AI Performance Analytics flags exactly which sub-topics like cholesteatoma vs CSOM are dropping your accuracy, then recommends a personalized revision schedule for your last 4 weeks before FMGE.
7. Otitis Media Spectrum
This appears as pediatric emergency scenarios and chronic disease management cases.
Acute Otitis Media:
Peak age: 6 months to 2 years
S. pneumoniae, H. influenzae, M. catarrhalis (common organisms)
Bulging, red, immobile tympanic membrane
Amoxicillin = first-line (high-dose: 80-90 mg/kg/day)
Otitis Media with Effusion (OME):
Non-infected fluid behind intact tympanic membrane
Hearing loss without pain/fever
Watch and wait for 3 months before intervention
Myringotomy + tubes if persistent beyond 3 months with hearing loss
CSOM vs Cholesteatoma:
CSOM: central perforation, mucopurulent discharge, safe ear
Cholesteatoma: marginal perforation, foul discharge, dangerous ear
8. Laryngeal Pathology
Focuses on voice disorders and airway emergencies. Less frequent but high-impact when it appears.
Vocal Cord Paralysis:
Unilateral: breathy voice, aspiration risk
Bilateral: stridor, airway compromise
Left RLN paralysis more common (longer course, thoracic pathology)
Medialization procedures for unilateral paralysis
Laryngeal Cancer Red Flags:
Hoarseness >2 weeks in smoker >40 years
Odynophagia + otalgia (referred pain pattern)
Neck mass + voice change
Direct laryngoscopy + biopsy = diagnostic gold standard
Common FMGE ENT Question Patterns
Pattern 1: Audiogram Interpretation
"A 45-year-old presents with hearing loss. Audiogram shows air conduction thresholds at 60 dB, bone conduction at 20 dB. What is the diagnosis?"
Answer Approach:
Calculate air-bone gap: 60-20 = 40 dB gap
Gap >30 dB = conductive hearing loss
Think CSOM, otosclerosis, ossicular chain disruption
Pattern 2: Emergency Scenarios
"A 6-year-old presents with severe otalgia, fever, and bulging red tympanic membrane. Best immediate management?"
Answer Logic:
Acute otitis media diagnosis
Age <2 years OR severe symptoms = immediate antibiotics
Amoxicillin high-dose = first choice
Myringotomy if no response in 48-72 hours
Pattern 3: Surgical Decision-Making
"Central tympanic membrane perforation, dry ear, intact ossicular chain on examination. Best surgical option?"
Elimination Strategy:
Central perforation + intact ossicles = Type I myringoplasty
Eliminate mastoidectomy options (no cholesteatoma)
Eliminate ossicular reconstruction (chains intact)
High-Yield FMGE ENT Facts for Last-Minute Revision
Quick Recognition Patterns
Foul otorrhea + marginal perforation = Cholesteatoma
Positional vertigo lasting seconds = BPPV
Hearing loss + tinnitus + vertigo + fullness = Meniere
Unilateral nasal polyp in adult = Rule out malignancy
Hoarseness >2 weeks in smoker = Laryngoscopy needed
Drug Dosages (Commonly Asked)
Acute SNHL: Prednisolone 1 mg/kg (max 80 mg) for 7 days
Acute otitis media: Amoxicillin 80-90 mg/kg/day divided BID
Allergic rhinitis: Fluticasone 2 sprays each nostril daily
Vestibular neuritis: Prednisolone 1 mg/kg within 72 hours
Timeframes (Critical for FMGE)
Sudden SNHL: Steroids within 72 hours
Acute otitis media: Antibiotics if no improvement in 48-72 hours
OME: Watch and wait for 3 months before tubes
Epistaxis: Anterior packing for 48-72 hours maximum
Common FMGE ENT Distractors to Avoid
Distractor Pattern 1: Overtreatment
Question presents simple OME
Distractor options include immediate myringotomy
Correct answer: watchful waiting for 3 months
Distractor Pattern 2: Wrong Drug Choice
Acute otitis media case
Distractor: Azithromycin (not first-line)
Correct: High-dose amoxicillin
Distractor Pattern 3: Misreading Audiograms
Present conductive hearing loss pattern
Distractor: Labels it as SNHL
Key: Always calculate air-bone gap first
Strategic Approach to ENT Revision
Week 1-2: Foundation Building
Master audiogram interpretation basics
Understand Rinne/Weber test logic
Learn cholesteatoma vs CSOM differentiation
Week 3-4: Clinical Pattern Recognition
Practice vertigo case scenarios
Drill tympanoplasty indications
Review epistaxis management protocols
Final Week: High-Yield Facts
Memorize drug dosages and timeframes
Review emergency management steps
Practice elimination strategies for common distractors
The smartest students dont try to master every ENT topic. They identify the 8-10 clusters that deliver maximum FMGE marks, then drill those patterns until recognition becomes automatic. Focus your energy where it counts.
Frequently Asked Questions
What percentage of FMGE questions come from ENT?
ENT typically contributes 8-12 questions out of 300 total FMGE questions, representing about 2.7-4% of the exam weightage.
Which ENT topics have the highest yield for FMGE 2026?
Audiology (SNHL vs CSOM), vertigo disorders (BPPV, Meniere), epistaxis management, tympanoplasty classification, and cholesteatoma diagnosis appear most frequently.
How should I approach audiogram interpretation questions?
Calculate the air-bone gap first. Gap >30 dB indicates conductive hearing loss. Equal air and bone conduction suggests sensorineural hearing loss. This basic principle solves 80% of audiometry questions.
What are the most common ENT emergency scenarios in FMGE?
Acute otitis media management, epistaxis control, sudden sensorineural hearing loss treatment, and acute vertigo evaluation appear regularly as clinical scenarios.
Should I memorize all tympanoplasty types for FMGE?
Focus on Types I-III which cover 90% of clinical scenarios. Type I (intact ossicular chain) and Type III (columella effect) are most commonly tested.
How many months should I dedicate specifically to ENT preparation?
ENT requires 3-4 weeks of focused study within your overall FMGE preparation timeline. Spend 2 weeks on core topics, 1 week on clinical patterns, and 1 week on high-yield review.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for FMGE. Download free on Android and iOS.