Back
FMGE Biochemistry High Yield Topics 2026 — Subject-Wise Guide for Foreign Medical Graduates
Master FMGE biochemistry with this comprehensive 2026 guide covering 8 high-yield chapters, clinical correlations, and MCQ patterns. Score 32+ out of 40 questions.

FMGE Biochemistry High Yield Topics 2026 — Subject-Wise Guide for Foreign Medical Graduates
FMGE June 2026 has 300 MCQs. Biochemistry contributes 35-40 questions consistently. You have 2 minutes per question.
Here's what matters: FMGE biochemistry tests clinical correlation, not pathway memorization. That child with recurrent infections and G6PD deficiency? The woman with fatty liver and carnitine deficiency? These are the scenarios that matter.
After analyzing 5 years of FMGE papers, I've mapped the 8 highest-yield biochemistry chapters. Master these and you'll nail 32-35 of those 40 questions. The other 5 come from low-yield topics that aren't worth your time.
This guide breaks down each high-yield chapter by clinical presentations, must-know facts, and the exact MCQ patterns FMGE repeats. No fluff, no low-yield pathways — just what shows up on exam day.
Why FMGE Biochemistry Feels Different
Traditional Indian PG exams test detailed pathway steps. FMGE tests clinical reasoning.
A typical NEET-PG question asks: "Which enzyme converts glucose-6-phosphate to 6-phosphogluconate in the pentose phosphate pathway?"
An FMGE question asks: "A 6-year-old boy presents with hemolytic anemia after taking antimalarial medication. What is the most likely enzyme deficiency?"
Same topic (G6PD deficiency), completely different approach. FMGE wants you to connect the biochemical defect to the clinical picture.
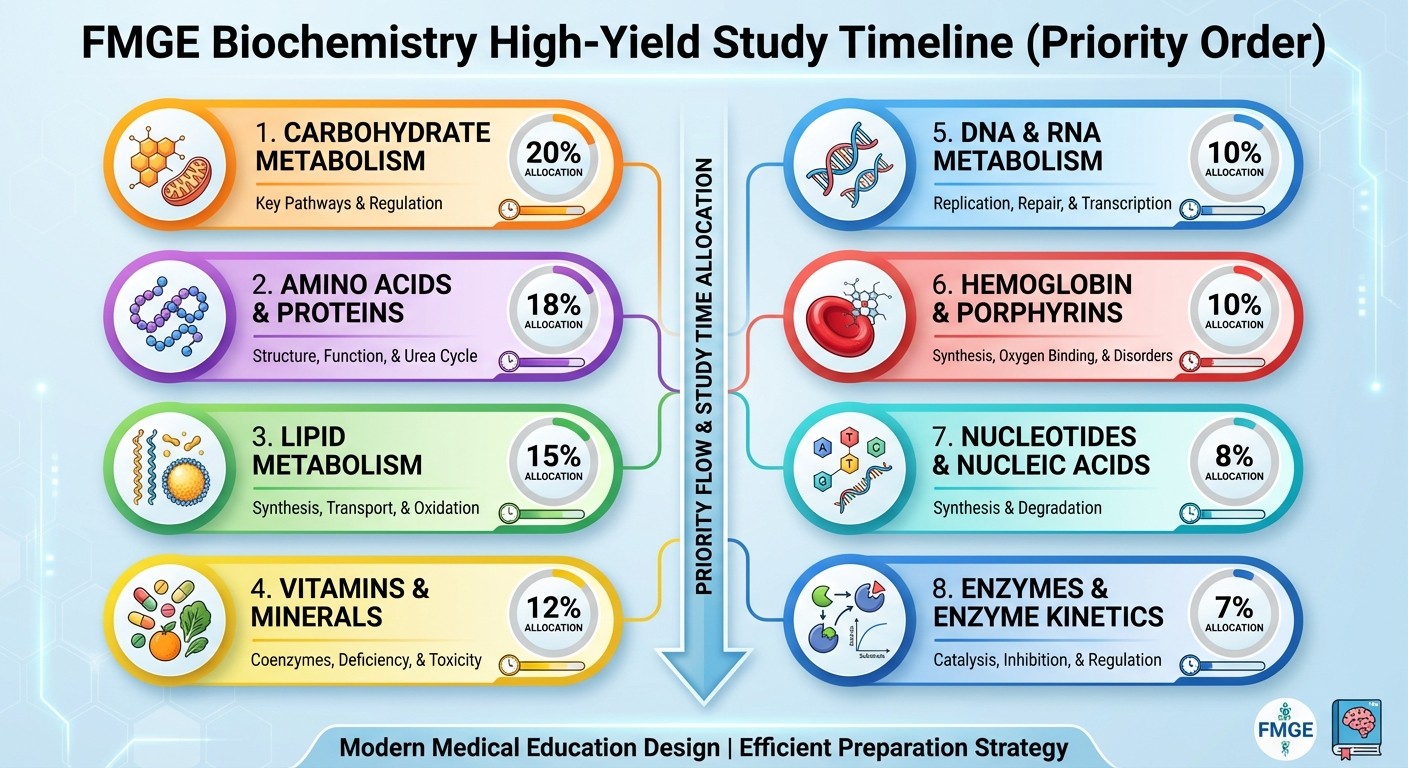
High-Yield Chapter Breakdown by Weightage
Chapter | Questions Per Exam | Clinical Focus |
|---|---|---|
Carbohydrate Metabolism | 8-10 | GSDs, G6PD deficiency, diabetes |
Amino Acid Metabolism | 6-8 | Aminoacidopathies, urea cycle |
Lipid Metabolism | 5-6 | Lipoprotein disorders, fatty acid oxidation |
Vitamins & Coenzymes | 4-5 | Deficiency syndromes |
Hemoglobin & Porphyrins | 3-4 | Thalassemias, porphyrias |
Molecular Biology | 3-4 | DNA repair, chromosomal disorders |
Nucleotide Metabolism | 2-3 | Gout, Lesch-Nyhan |
Enzyme Kinetics | 1-2 | Km/Vmax, isoenzymes |
1. Carbohydrate Metabolism — The Heavyweight (8-10 Questions)
This chapter alone determines your biochemistry score. Focus on these clinical presentations:
Glycogen Storage Diseases (GSDs)
High-yield clinical triads:
GSD I (von Gierke): Hepatomegaly + hypoglycemia + lactic acidosis
GSD II (Pompe): Cardiomegaly + muscle weakness + death before 2 years
GSD V (McArdle): Exercise intolerance + muscle cramps + normal blood glucose
FMGE favorites:
GSD I: Glucose-6-phosphatase deficiency, cant break down glucose from glycogen
GSD II: Lysosomal α-glucosidase deficiency, glycogen accumulates in lysosomes
GSD III: Debranching enzyme deficiency, mild hepatomegaly
GSD V: Muscle phosphorylase deficiency, exercise intolerance
Oncourse's carbohydrate metabolism MCQs include detailed explanations showing how each enzyme defect leads to the specific clinical picture — exactly what FMGE tests.
G6PD Deficiency
Must-know triggers:
Antimalarials (primaquine, chloroquine)
Sulfonamides
Fava beans
Naphthalene (mothballs)
Clinical presentation: Hemolytic anemia 2-3 days after trigger exposure. X-linked inheritance pattern. Mechanism: G6PD deficiency → reduced NADPH → cant regenerate glutathione → RBC hemolysis under oxidative stress.
Diabetes Mellitus Biochemistry
FMGE tests these pathways:
Polyol pathway: Sorbitol accumulation in diabetic complications
Advanced glycation end products (AGEs): HbA1c formation
Ketogenesis: DKA mechanism
Key enzymes: Aldose reductase (sorbitol formation), hexokinase vs glucokinase (different Km values).
2. Amino Acid Metabolism — Clinical Correlations (6-8 Questions)
FMGE loves amino acid disorders because they present in childhood with characteristic clinical pictures.
Phenylketonuria (PKU)
Clinical triad: Mental retardation + musty odor + fair skin Defect: Phenylalanine hydroxylase deficiency Screening: Heel prick test (Guthrie test) Treatment: Phenylalanine-restricted diet
Alkaptonuria
Clinical: Dark urine + arthritis in adulthood Defect: Homogentisic acid oxidase deficiency Mechanism: Homogentisic acid accumulation → darkening on exposure to air
Urea Cycle Defects
General presentation: Hyperammonemia + altered consciousness Most common: Carbamoyl phosphate synthetase I deficiency Key concept: Urea cycle occurs primarily in liver, defects cause ammonia buildup
Practice with targeted amino acid metabolism questions that mirror FMGE's clinical approach rather than pure pathway memorization.
Methionine Cycle & Homocystinuria
Clinical: Marfan-like features + lens dislocation + mental retardation Defect: Cystathionine synthase deficiency Biochemical marker: Elevated homocysteine in blood and urine
3. Lipid Metabolism — Beyond Cholesterol (5-6 Questions)
Lipoprotein Disorders
Type I Hyperlipoproteinemia: Lipoprotein lipase deficiency → chylomicronemia → pancreatitis Type II (Familial hypercholesterolemia): LDL receptor defects → premature CAD Type IV: Increased VLDL → hypertriglyceridemia
Fatty Acid Oxidation Defects
Medium-chain acyl-CoA dehydrogenase deficiency: Hypoketotic hypoglycemia in children Carnitine deficiency: Muscle weakness + fatty liver + cannot oxidize long-chain fatty acids Key concept: Carnitine shuttle required for long-chain fatty acids to enter mitochondria for β-oxidation. When discussing fatty acid oxidation defects, Oncourse's adaptive daily plans automatically increase your exposure to these metabolic disorders based on your MCQ performance patterns.
Essential Fatty Acids
Linoleic acid deficiency: Scaly skin + growth retardation Arachidonic acid pathway: COX vs LOX pathways, aspirin mechanism
Study these patterns with lipid metabolism lessons that emphasize clinical presentations over biochemical details.
4. Molecular Biology & Genetics — DNA Repair Focus (3-4 Questions)
DNA Repair Syndromes
Xeroderma pigmentosum: UV sensitivity + skin cancers + nucleotide excision repair defect Ataxia telangiectasia: Cerebellar ataxia + telangiectasias + ATM gene defect Bloom syndrome: Growth retardation + DNA helicase defect
Chromosomal Disorders
Turner syndrome: 45,X + short stature + primary amenorrhea Klinefelter syndrome: 47,XXY + tall stature + gynecomastia + small testes Down syndrome: Trisomy 21 + characteristic facies + mental retardation FMGE pattern: They give clinical presentation, you identify the chromosomal abnormality.
5. Vitamins & Coenzymes — Deficiency-Disease Pairs (4-5 Questions)
Water-Soluble Vitamins
Vitamin | Deficiency Disease | Key Clinical Feature |
|---|---|---|
B1 (Thiamine) | Beriberi, Wernicke-Korsakoff | Peripheral neuropathy, confabulation |
B2 (Riboflavin) | Ariboflavinosis | Angular cheilitis, magenta tongue |
B3 (Niacin) | Pellagra | 4 Ds: Dermatitis, Diarrhea, Dementia, Death |
B6 (Pyridoxine) | Peripheral neuropathy | Isoniazid-induced neuropathy |
B12 (Cobalamin) | Megaloblastic anemia | Subacute combined degeneration |
Folate | Megaloblastic anemia | Neural tube defects |
Vitamin C | Scurvy | Bleeding gums, poor wound healing |
Fat-Soluble Vitamins
Vitamin | Deficiency | Key Feature |
|---|---|---|
A | Night blindness | Bitot's spots, keratomalacia |
D | Rickets/Osteomalacia | Bone deformities, hypocalcemia |
E | Hemolytic anemia | Neurological symptoms |
K | Bleeding disorders | Prolonged PT, easy bruising |
Enzyme-Coenzyme High-Yields:
TPP (thiamine): Pyruvate dehydrogenase, transketolase
FAD (riboflavin): Succinate dehydrogenase
NAD (niacin): Glycolysis, TCA cycle
PLP (B6): Aminotransferases
The vitamin deficiency clinical pictures are perfect for Synapses spaced repetition — these biochemistry flashcards help lock in the deficiency-disease pairs through spaced intervals.
6. Hemoglobin & Porphyrins — Genetic Focus (3-4 Questions)
Thalassemias
β-thalassemia major: Severe anemia + hepatosplenomegaly + requires regular transfusions β-thalassemia minor: Mild microcytic anemia + elevated HbA2 (>3.5%) α-thalassemia: 4 α-genes, severity depends on number of deleted genes HbS (Sickle cell): Glu6→Val substitution, causes polymerization under low oxygen
Porphyrias
Acute intermittent porphyria: Abdominal pain + neuropsychiatric symptoms + PBG deaminase deficiency Porphyria cutanea tarda: Photosensitive skin lesions + uroporphyrinogen decarboxylase deficiency FMGE focus: Clinical presentation → identify the type of thalassemia or porphyria.
7. Nucleotide Metabolism — Purine/Pyrimidine Disorders (2-3 Questions)
Purine Metabolism Defects
Lesch-Nyhan syndrome: Self-mutilation + mental retardation + HGPRT deficiency Gout: Hyperuricemia + joint pain + uric acid crystal deposition Adenosine deaminase deficiency: SCID (bubble boy disease)
Pyrimidine Metabolism
Orotic aciduria: Megaloblastic anemia + orotic acid in urine + UMP synthase deficiency Clinical correlation: These present as neurological disorders (Lesch-Nyhan), joint disorders (gout), or immunodeficiency (ADA deficiency).
8. Enzyme Kinetics — Diagnostic Focus (1-2 Questions)
Km and Vmax Concepts
Km: Substrate concentration at half Vmax (affinity measure)
Low Km = high affinity
High Km = low affinity
Competitive inhibition: Km increases, Vmax unchanged Non-competitive inhibition: Km unchanged, Vmax decreases
Diagnostic Isoenzymes
CK-MB: Heart-specific, elevated in MI LDH1 > LDH2: Cardiac damage (normally LDH2 > LDH1) Alkaline phosphatase isoenzymes: Bone vs liver vs placental FMGE pattern: Given clinical scenario + enzyme levels, identify the organ damage.
Smart Study Strategy for FMGE Biochemistry 2026
Time Allocation (Based on Question Weightage)
Weeks 1-2: Carbohydrate metabolism (40% of study time)
Week 3: Amino acid metabolism
Week 4: Lipid metabolism + Vitamins
Week 5: Hemoglobin/Porphyrins + Molecular biology
Week 6: Nucleotide metabolism + Enzyme kinetics + Revision
Daily Study Pattern
Morning (2 hours): New topic theoretical concepts Afternoon (1 hour): MCQ practice on yesterday's topics Evening (30 mins): Flashcard review of previously studied chapters
Each FMGE biochemistry MCQ on Oncourse includes detailed explanations connecting the biochemical defect to clinical presentation — building the exact reasoning pattern FMGE tests.
Common FMGE Biochemistry Traps
Trap 1: Confusing GSD types Solution: Remember the organs affected — liver (I,III), heart (II), muscle (V) Trap 2: Vitamin deficiency look-alikes Solution: B12 has neurological symptoms, folate doesnt Trap 3: Thalassemia vs Iron deficiency Solution: Thalassemia has elevated HbA2, iron deficiency has low ferritin Trap 4: Porphyria types Solution: Acute = abdominal pain, cutaneous = skin lesions
Integration with Other FMGE Subjects
Biochemistry connects heavily with:
Pathology: Enzyme markers, genetic disorders
Pharmacology: Vitamin supplements, enzyme inhibitors
Pediatrics: Inborn errors of metabolism
Medicine: Diabetes, liver diseases, anemia workup
When you study GSD in biochemistry, review the pathology changes. When you cover vitamin deficiencies, check the pharmacology of supplements. This integrated approach mirrors FMGE's clinical correlation style.
For a complete FMGE preparation strategy covering all subjects, check our FMGE 2026 complete exam guide and complement your biochemistry preparation with our FMGE pathology high-yield topics.
Frequently Asked Questions
How many biochemistry questions appear in FMGE June 2026?
FMGE consistently has 35-40 biochemistry questions out of 300 total MCQs. This represents about 13% of the exam, making it the fourth highest-weighted subject after Medicine, Surgery, and Pediatrics.
Should I memorize all metabolic pathways for FMGE biochemistry?
No. FMGE tests clinical correlations, not pathway details. Focus on enzyme defects that cause diseases, not every step of glycolysis. Learn what happens when the pathway breaks, not how it normally works.
Which biochemistry chapter has the highest yield for FMGE?
Carbohydrate metabolism contributes 8-10 questions per exam. Within this, glycogen storage diseases and G6PD deficiency are absolute must-knows. These topics appear in every FMGE exam.
How is FMGE biochemistry different from NEET-PG biochemistry?
FMGE tests "pathway defect → clinical presentation" reasoning. NEET-PG tests "enzyme → substrate → product" memorization. FMGE gives you symptoms, you identify the metabolic disorder. NEET-PG gives you a pathway step, you complete the sequence.
Can I skip enzyme kinetics for FMGE biochemistry preparation?
Enzyme kinetics contributes only 1-2 questions but they're often high-scoring. Focus on Km/Vmax concepts and diagnostic isoenzymes (CK-MB, LDH). Skip detailed mathematical calculations.
What's the best way to remember vitamin deficiency diseases?
Use clinical pictures, not vitamin names. "Night blindness" → Vitamin A. "Bleeding gums" → Vitamin C. "Confabulation" → B1 deficiency. The clinical presentation is what FMGE tests, not the biochemical structure of vitamins.
---
Master these 8 high-yield chapters with clinical focus and you'll score 32+ out of 40 biochemistry questions in FMGE June 2026. Remember — FMGE rewards clinical reasoning over rote memorization.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for FMGE. Download free on Android and iOS.