DKA vs HHS: High-Yield Clinical Differentiation for NEET PG 2026
Master DKA vs HHS differentiation for NEET PG 2026. Complete guide to pathophysiology, lab findings, clinical presentation, and management of diabetic emergencies.
DKA vs HHS: High-Yield Clinical Differentiation for NEET PG 2026
You are probably staring at a case stem with glucose levels above 400 mg/dL, wondering whether this patient has DKA or HHS. The answer lies in three critical lab values that NEET PG 2026 will test relentlessly: pH, ketones, and serum osmolality. Miss these distinctions, and you'll confuse the two most high-yield diabetic emergencies.
DKA and HHS account for 15-20% of endocrinology questions in NEET PG. Both present with hyperglycemia, but their pathophysiology, clinical presentation, and management protocols are completely different. One kills through acidosis (DKA), the other through severe dehydration and hyperosmolarity (HHS).
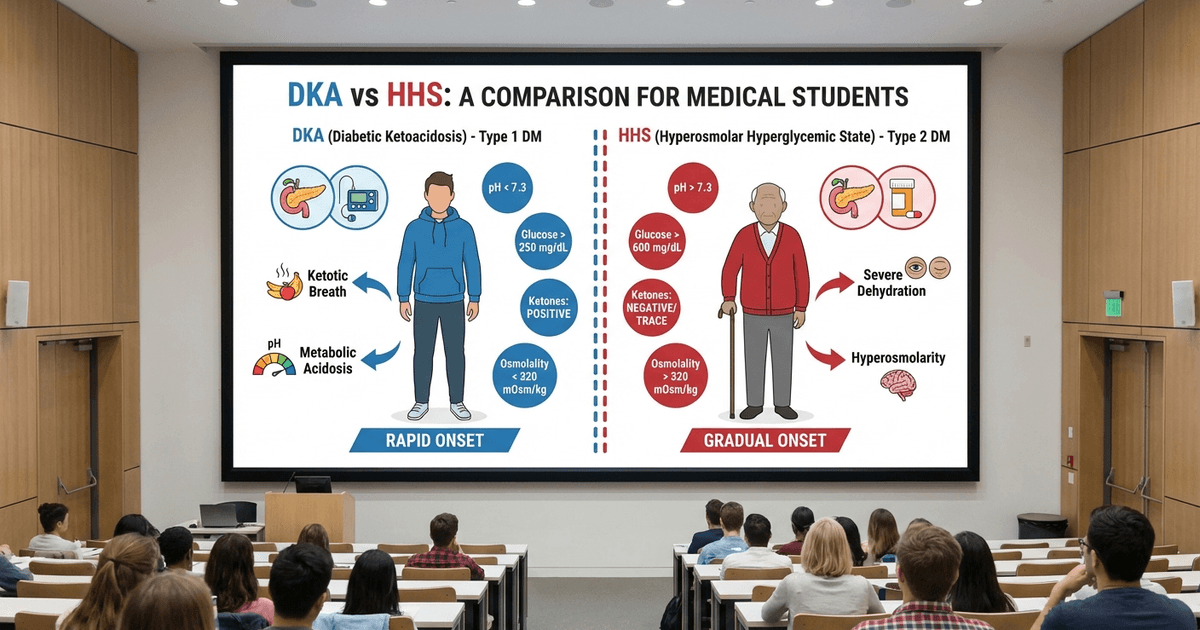
The key insight most students miss: DKA is a ketotic emergency in younger Type 1 diabetics, while HHS is a non-ketotic crisis in elderly Type 2 patients. The presence or absence of ketones isn't just a lab finding — it determines everything from fluid management to insulin protocols.
Quick Comparison: DKA vs HHS
Parameter | DKA | HHS |
|---|---|---|
Age | Usually <40 years | Usually >60 years |
Diabetes Type | Type 1 (or severe Type 2) | Type 2 |
Onset | Hours to days | Days to weeks |
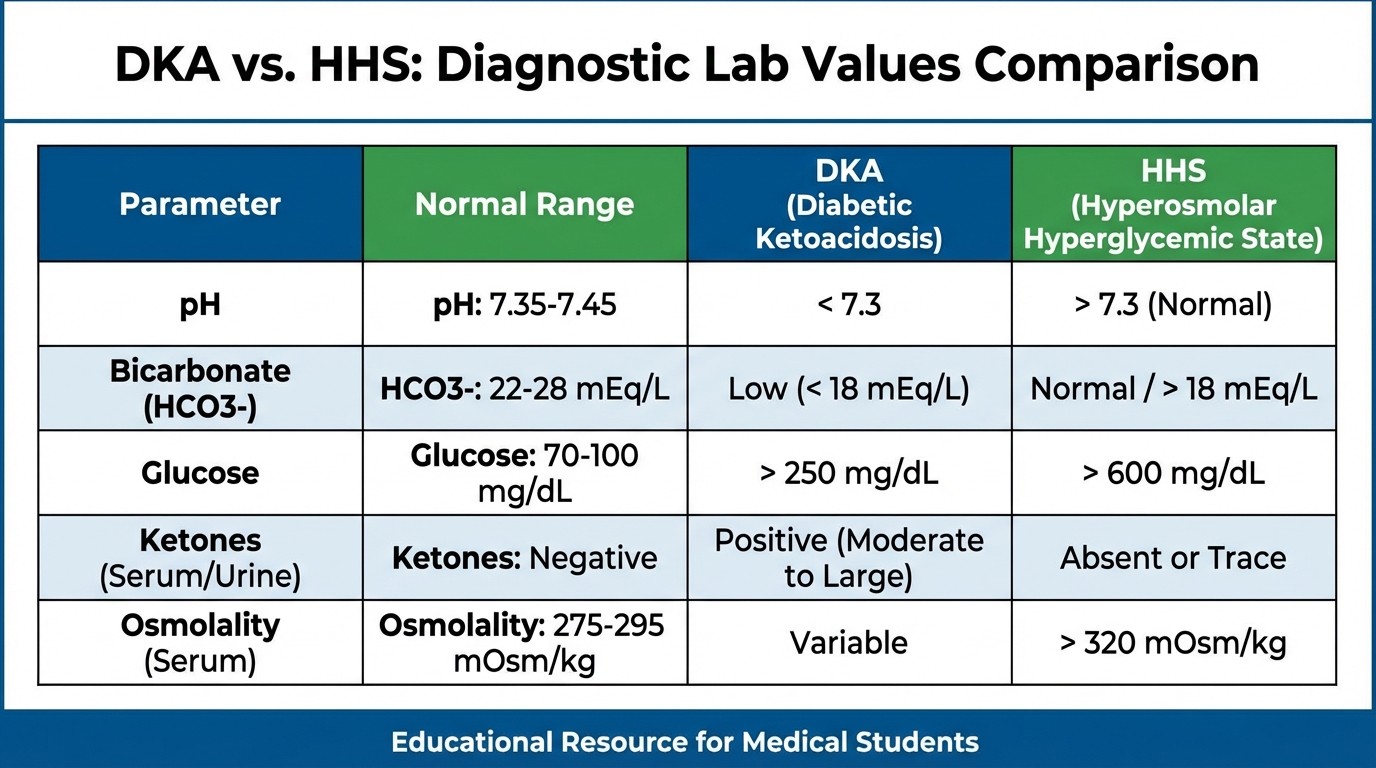
pH | <7.3 | >7.3 (normal) |
Bicarbonate | <15 mEq/L | Normal (>15 mEq/L) |
Ketones | Strongly positive | Absent or minimal |
Glucose | 250-800 mg/dL | >600 mg/dL (often >1000) |
Osmolality | <320 mOsm/kg | >320 mOsm/kg |
Mortality | 5-10% | 15-20% |
Pathophysiology: Why They Develop Differently
Understanding the pathophysiology explains why exam questions can trick you with overlapping presentations.
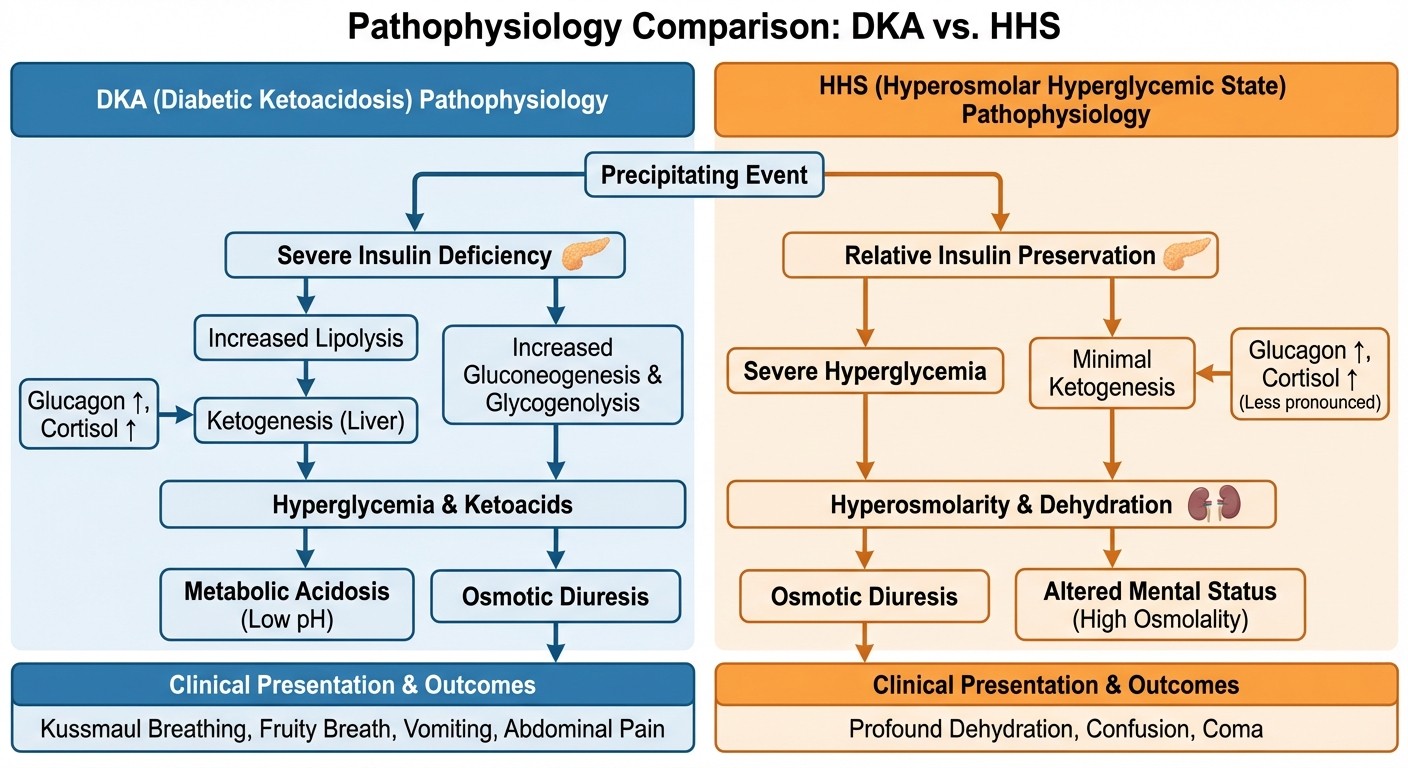
DKA Pathophysiology
DKA develops when absolute insulin deficiency triggers uncontrolled lipolysis and ketogenesis. The process follows this sequence:
1. Insulin deficiency (infection, non-compliance, first presentation)
2. Counter-regulatory hormone surge (glucagon, cortisol, catecholamines)
3. Hepatic glucose production increases + peripheral glucose utilization decreases
4. Lipolysis accelerates → free fatty acids flood the liver
5. Ketogenesis → beta-hydroxybutyrate and acetoacetate accumulation
6. Metabolic acidosis with compensatory hyperventilation
The mnemonic "MUDPILES" helps identify DKA precipitants, but infection remains the most common trigger (40% of cases). When reviewing these mechanisms, Oncourse's smart flashcards drill the exact pathways with spaced repetition.
HHS Pathophysiology
HHS occurs when relative insulin deficiency meets severe dehydration without significant ketosis:
1. Relative insulin deficiency (enough to prevent ketosis, insufficient for glucose control)
2. Progressive hyperglycemia over days to weeks
3. Osmotic diuresis leads to massive fluid losses (9-12 liters)
4. Hyperosmolarity (>320 mOsm/kg) without acidosis
5. Vascular volume depletion with hyperviscosity
The key difference: residual insulin prevents lipolysis and ketogenesis but cant control glucose. This explains why HHS patients develop extreme hyperglycemia (often >1000 mg/dL) without ketones.
Clinical Presentation: Pattern Recognition for NEET PG
DKA Presentation
DKA patients present with the classic triad plus specific signs:
Classic Triad:
Polyuria, polydipsia, polyphagia
Nausea, vomiting, abdominal pain (may mimic acute abdomen)
Altered mental status (confusion to coma)
DKA-Specific Signs:
Kussmaul respirations (deep, labored breathing)
Fruity breath odor (acetone)
Dehydration (5-10% total body water loss)
Tachycardia and hypotension
The abdominal pain in DKA can be severe enough to mimic surgical emergencies. NEET PG loves this clinical trap — always check glucose and ketones in acute abdomen cases.
HHS Presentation
HHS presents with extreme dehydration without ketotic features:
Dominant Features:
Severe dehydration (15-20% total body water loss)
Altered mental status (more profound than DKA)
Hyperviscosity signs (thrombosis risk)
Absent ketotic breath
Normal or shallow breathing (no compensatory hyperventilation)
Neurological Signs:
Focal neurological deficits (reversible)
Seizures (focal or generalized)
Hemiparesis (stroke-like presentation)
The stroke-like symptoms in HHS are completely reversible with treatment — a high-yield fact for NEET PG case scenarios.
Laboratory Diagnosis: The Numbers That Matter
DKA Lab Criteria
NEET PG tests these specific cutoffs:
Essential Labs:
Glucose: >250 mg/dL (usually 250-800 mg/dL)
pH: <7.3 (arterial) or bicarbonate <15 mEq/L (venous)
Ketones: Positive (serum or urine)
Anion gap: >12 mEq/L (high anion gap metabolic acidosis)
Supporting Labs:
BUN/Creatinine: Elevated (prerenal azotemia)
Potassium: Variable (total body depletion despite normal/high levels)
Phosphate: Low
WBC: Elevated (stress response, even without infection)
HHS Lab Criteria
Essential Labs:
Glucose: >600 mg/dL (often >1000 mg/dL)
pH: >7.3 (normal acid-base status)
Bicarbonate: >15 mEq/L
Serum osmolality: >320 mOsm/kg
Ketones: Absent or minimal
Osmolality Calculation:
Serum osmolality = 2(Na + K) + (glucose/18) + (BUN/2.8)
When working through HHS cases, practice MCQs help recognize the pattern where extreme hyperglycemia occurs without acidosis.
Key Laboratory Traps
NEET PG High-Yield Points: 1. Normal glucose doesnt rule out DKA — euglycemic DKA occurs with SGLT2 inhibitors 2. Ketones can be present in HHS — but usually minimal (<3 mmol/L) 3. Serum sodium is falsely low in both conditions (pseudohyponatremia from hyperglycemia) 4. Corrected sodium = measured sodium + [(glucose - 100) × 0.016]
Management Protocols: Treatment Algorithms
DKA Management
Phase 1: Initial Stabilization (0-2 hours) Fluid Replacement:
Normal saline 1-2 L in first hour
Continue with 250-500 mL/hr based on hydration status
Switch to 0.45% saline when glucose <250 mg/dL
Insulin Protocol:
IV regular insulin bolus: 0.1 units/kg
Continuous infusion: 0.1 units/kg/hr
Target glucose reduction: 50-75 mg/dL per hour
Electrolyte Management:
Potassium replacement when K+ <5.3 mEq/L (before insulin)
Phosphate replacement if severe deficiency
Magnesium replacement PRN
Phase 2: Ongoing Management
Add dextrose when glucose <250 mg/dL (continue insulin for ketone clearance)
Bicarbonate only if pH <6.9 or severe hyperkalemia
Monitor anion gap closure
HHS Management
Fluid Management (Critical Difference):
More aggressive initial fluid replacement
Normal saline 1-2 L in first 2 hours
Target: replace 50% of estimated fluid deficit in 12 hours
Monitor for cerebral edema (rare but serious)
Insulin Protocol:
Lower insulin requirements than DKA
Start at 0.05-0.1 units/kg/hr
Target glucose reduction: 50-100 mg/dL per hour
Special Considerations:
DVT prophylaxis (hyperviscosity increases thrombosis risk)
Frequent neurological assessments
Slower correction to prevent cerebral edema
Oncourse's performance analytics track your weak spots in these protocols, auto-scheduling review of insulin calculations and fluid management principles you miss.
Precipitating Factors: What Triggers Each Emergency
Common DKA Precipitants
NEET PG Favorites: 1. Infection (40% of cases) — UTI, pneumonia, skin infections 2. Insulin non-compliance (25%) 3. First presentation of Type 1 diabetes (20%) 4. Medical illness — MI, stroke, pancreatitis 5. Medications — steroids, thiazides, atypical antipsychotics New-Onset Precipitants:
SGLT2 inhibitors (euglycemic DKA)
COVID-19 infection
Immune checkpoint inhibitors
Common HHS Precipitants
Typical Triggers: 1. Infection (most common) — pneumonia, UTI, sepsis 2. Medication non-compliance 3. Cardiovascular events — MI, stroke 4. Medications — thiazides, beta-blockers, steroids 5. Medical procedures — dialysis, surgery High-Risk Populations:
Elderly patients with limited fluid access
Nursing home residents
Patients with dementia or functional impairment
Clinical Reasoning: Exam-Style Case Analysis
Case 1: Typical DKA
"A 22-year-old student presents with 2-day history of nausea, vomiting, and abdominal pain. On examination: dehydrated, fruity breath, deep labored breathing. Labs: glucose 450 mg/dL, pH 7.15, bicarbonate 8 mEq/L, positive urine ketones." Reasoning Process:
1. Young age → think Type 1 diabetes
2. Fruity breath + Kussmaul respirations → ketosis
3. pH <7.3 + low bicarbonate → metabolic acidosis
4. Positive ketones + hyperglycemia = DKA
Case 2: Typical HHS
"A 68-year-old diabetic presents with 1-week progressive confusion. Family reports decreased oral intake. On examination: severely dehydrated, focal weakness right arm. Labs: glucose 1200 mg/dL, pH 7.38, bicarbonate 22 mEq/L, osmolality 350 mOsm/kg, trace ketones." Reasoning Process:
1. Elderly + Type 2 diabetes → consider HHS
2. Normal pH/bicarbonate → no acidosis
3. Extreme hyperglycemia + high osmolality → HHS
4. Trace ketones (not significant) + neurological signs confirm HHS
When drilling through these case patterns, Oncourse's adaptive MCQ engine serves similar vignettes at increasing difficulty, helping you catch the subtle differences before exam day.
Complications and Monitoring
DKA Complications
Immediate Risks:
Cerebral edema (especially in children)
Hypokalemia from insulin therapy
Hypoglycemia from aggressive insulin
Pulmonary edema from fluid overload
Monitoring Parameters:
Hourly glucose, electrolytes
ABG every 2-4 hours until pH >7.3
Anion gap closure
Mental status
HHS Complications
Major Risks:
Thrombotic events (stroke, MI, PE)
Cerebral edema (from rapid correction)
Cardiovascular collapse
Rhabdomyolysis
Monitoring Focus:
Neurological status (stroke-like symptoms)
Fluid balance (avoid rapid correction)
Glucose trending
Osmolality normalization
High-Yield Mnemonics and Memory Aids
DKA vs HHS Memory Device:
DKA = Deep breathing, Dehydration, Dangerous ketones
HHS = Hyperosmolar, Heavy glucose (>1000), Half-dead from dehydration
MUDPILES for DKA Precipitants:
Methanol, Uremia, DKA, Paraldehyde, Infection, Lactic acidosis, Ethylene glycol, Salicylates
Treatment Priority Mnemonic:
FINE: Fluids, Insulin, Need electrolytes, Examine frequently
Frequently Asked Questions
What pH cutoff differentiates DKA from HHS?
The critical pH cutoff is 7.3. DKA always has pH <7.3 due to ketoacidosis, while HHS maintains normal acid-base status with pH >7.3. This single lab value is often the deciding factor in NEET PG questions.
Can a patient have both DKA and HHS simultaneously?
Yes, though rare. Mixed presentations occur in severely ill patients with significant ketosis (DKA component) and extreme hyperosmolarity (HHS component). Look for pH between 7.25-7.30 with very high glucose and osmolality.
When should bicarbonate be given in DKA?
Bicarbonate is controversial and only recommended when pH <6.9 or severe hyperkalemia exists. Most DKA cases resolve acidosis with insulin and fluid therapy alone. Never give bicarbonate empirically.
How fast should glucose be corrected in HHS?
Target glucose reduction of 50-100 mg/dL per hour in HHS, slower than DKA's 50-75 mg/dL per hour. Rapid correction risks cerebral edema, especially dangerous in elderly HHS patients with compromised autoregulation.
What glucose level rules out DKA?
No glucose level rules out DKA. Euglycemic DKA (glucose <250 mg/dL) occurs with SGLT2 inhibitors, pregnancy, or alcohol use. Always check ketones and pH when DKA is suspected, regardless of glucose level.
Why do HHS patients have stroke-like symptoms?
Extreme hyperosmolarity (>350 mOsm/kg) causes cellular dehydration in brain tissue, leading to focal neurological deficits that mimic strokes. These symptoms are completely reversible with osmolality correction — a key differentiating feature from actual strokes.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG 2026. Download free on Android and iOS.