Back
45-Year-Old Man with Lower Extremity Edema: MPGN vs RPGN — High-Yield NEET PG Nephrology MCQ Guide (2026)
Master the differential diagnosis between MPGN and RPGN in a 45-year-old man with edema. Complete NEET PG nephrology guide with high-yield MCQ patterns, clinical features, and diagnostic approach.

45-Year-Old Man with Lower Extremity Edema: MPGN vs RPGN — High-Yield NEET PG Nephrology MCQ Guide (2026)
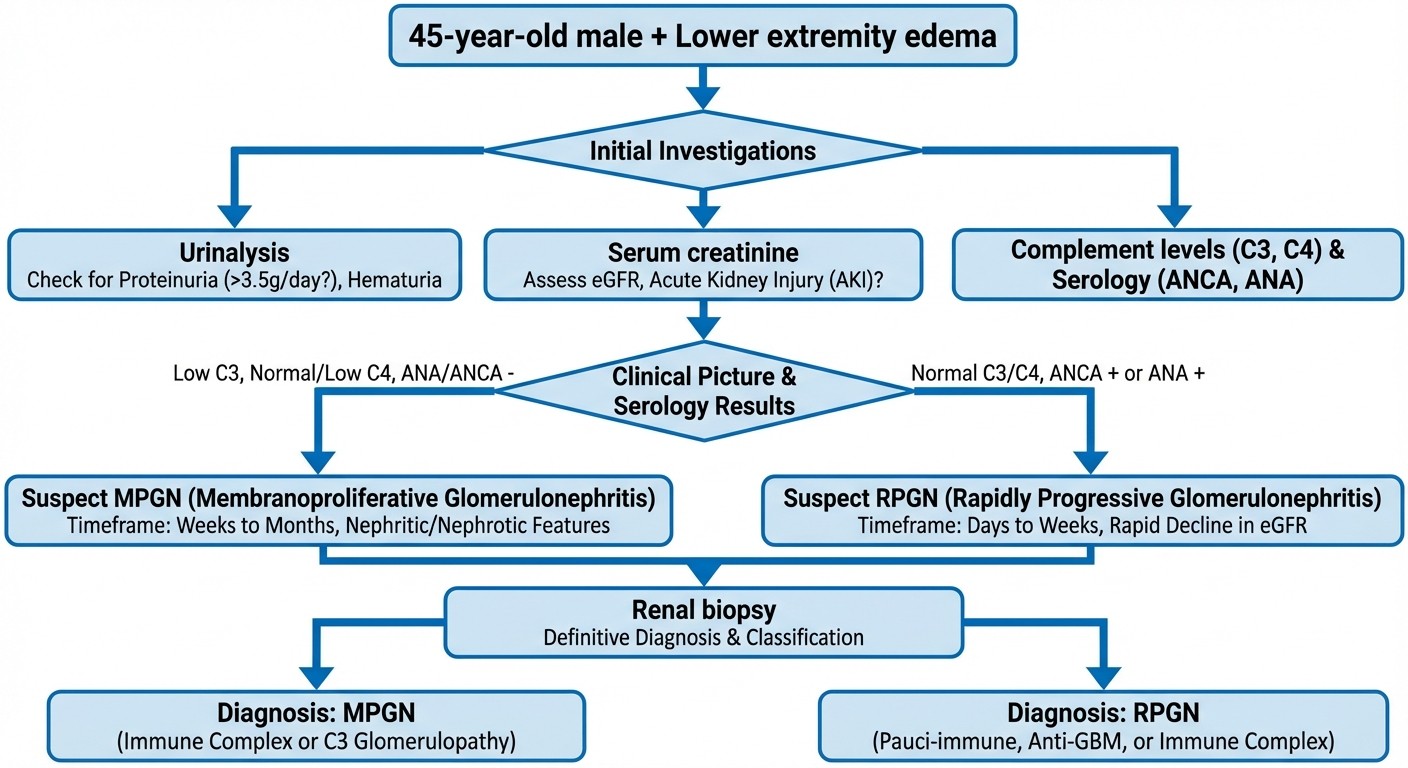
You are staring at a NEET PG question about a 45-year-old man presenting with bilateral lower extremity edema, proteinuria, and declining renal function. The answer choices include membranoproliferative glomerulonephritis (MPGN) and rapidly progressive glomerulonephritis (RPGN).
Your mind races through the differential. Age matters here. So does the timeline. So does that complement level they casually mentioned in the question stem.
NEET PG nephrology questions love this exact scenario because it tests your ability to distinguish between two serious glomerular diseases that can both present with edema and renal dysfunction. The difference? One kills kidneys in weeks, the other takes years. One shows crescents, the other shows thick basement membranes. One consumes complement, the other might not.
This guide breaks down the high-yield differences, MCQ patterns, and diagnostic approach that separates MPGN from RPGN in middle-aged adults. Because in NEET PG, getting this differential right can be the difference between selecting the correct answer and losing 4 marks.
Understanding the Clinical Scenario: 45-Year-Old Male with Edema
Why This Age Group Matters in NEET PG
NEET PG examiners specifically choose 45-year-old patients for glomerulonephritis questions because this age represents the peak incidence for several key conditions:
MPGN Type I: Peak incidence 30-50 years
RPGN (ANCA-associated): Peak incidence 40-60 years
Secondary causes: More common after age 40
The age alone narrows your differential significantly. Post-infectious glomerulonephritis? Unlikely at 45. Minimal change disease? Rare. IgA nephropathy? Possible but usually presents earlier.
Lower Extremity Edema: The Clinical Clue
Bilateral lower extremity edema in nephrology questions signals:
1. Significant proteinuria (>3.5g/day = nephrotic syndrome)
2. Reduced GFR with fluid retention
3. Hypoalbuminemia from urinary protein loss
But here's the NEET PG trick: Both MPGN and RPGN can present with edema. The key is in the timeline and associated findings.
MPGN vs RPGN: The Core Differential
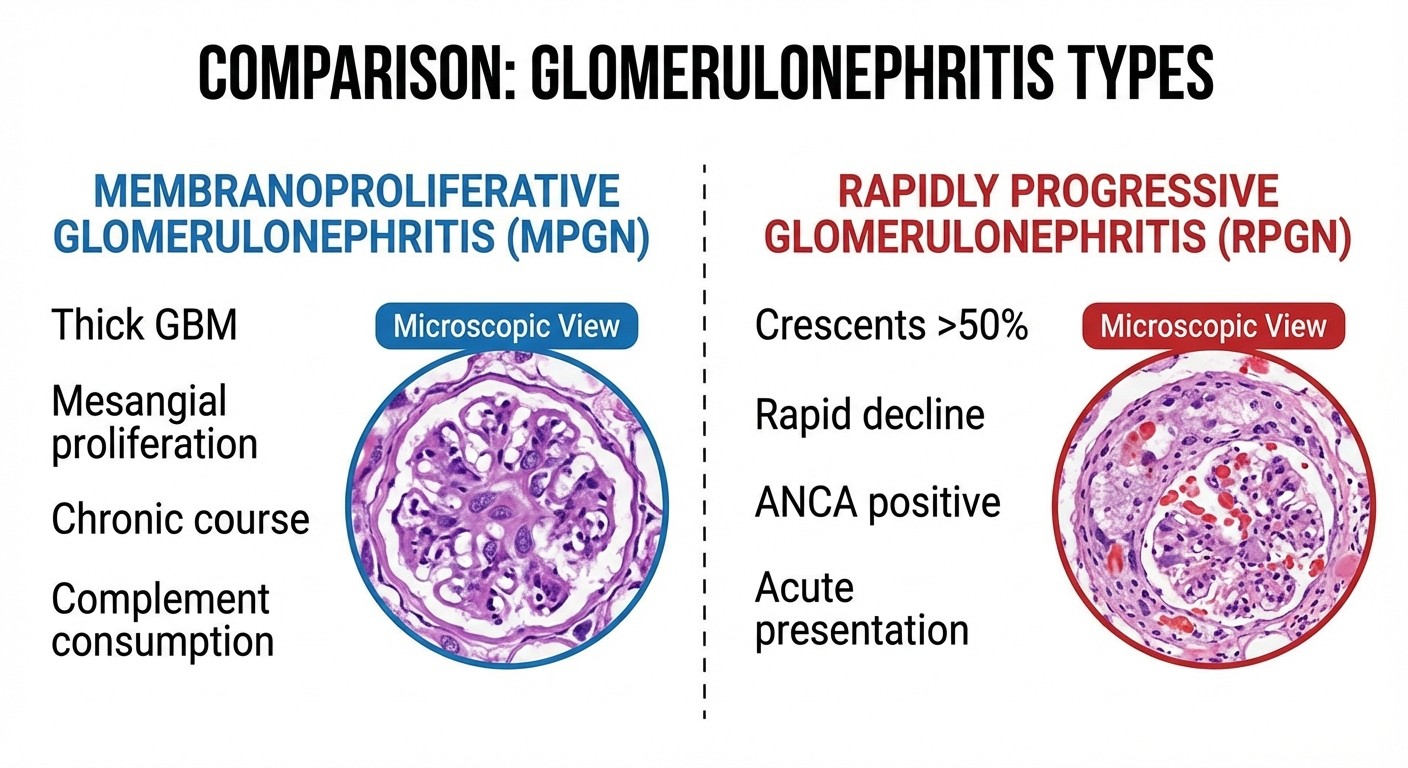
Membranoproliferative Glomerulonephritis (MPGN)
Pathophysiology: Chronic immune complex disease causing mesangial proliferation and basement membrane thickening. Key Clinical Features:
Age: 30-50 years (peak incidence)
Onset: Insidious, chronic course
Timeline: Months to years of progression
Edema: Gradual onset, often nephrotic syndrome
Hematuria: Microscopic, persistent
Hypertension: Common (70-80% of cases)
Laboratory Hallmarks:
C3 complement: Persistently low (diagnostic clue)
C4 complement: Normal in Type I, low in Type II
Proteinuria: Variable (1-15g/day)
Creatinine: Slowly rising over months
NEET PG High-Yield Points:
"Tram-track" appearance on light microscopy
Subendothelial deposits on electron microscopy
Associated with hepatitis C in adults
Poor prognosis: 50% reach ESRD in 10 years
Rapidly Progressive Glomerulonephritis (RPGN)
Pathophysiology: Crescentic glomerulonephritis with >50% glomerular crescents causing rapid nephron loss. Key Clinical Features:
Age: 40-60 years for ANCA-associated
Onset: Rapid, fulminant course
Timeline: Days to weeks of progression
Edema: Acute onset with oliguria
Hematuria: Gross hematuria common
Systemic symptoms: Fatigue, weight loss
Laboratory Hallmarks:
Creatinine: Rapidly rising (doubles in <3 months)
ANCA: Positive in 90% (c-ANCA/PR3 or p-ANCA/MPO)
Proteinuria: Variable (1-10g/day)
Complement: Usually normal
NEET PG High-Yield Points:
Crescents in >50% of glomeruli (diagnostic)
Three types: ANCA-associated, anti-GBM, immune complex
Medical emergency: Requires immediate treatment
Without treatment: Irreversible kidney failure in weeks
Diagnostic Approach: The NEET PG Framework
Step 1: Timeline Assessment
MPGN Timeline:
Symptoms present for months
Slow deterioration of renal function
Chronic edema, gradually worsening
RPGN Timeline:
Symptoms present for days to weeks
Rapid deterioration (creatinine doubles in <3 months)
Acute edema with oliguria
Step 2: Laboratory Workup Priority
First-line investigations: 1. Urinalysis: RBC casts suggest glomerulonephritis 2. 24-hour urine protein: Quantifies proteinuria 3. Serum creatinine: Establishes baseline and trend 4. Complete blood count: Anemia suggests chronic disease Second-line (diagnostic): 1. Complement levels (C3, C4): Low C3 points to MPGN 2. ANCA panel: Positive suggests RPGN 3. Anti-GBM antibodies: Rules out Goodpasture syndrome 4. Hepatitis serology: MPGN association
Step 3: Renal Biopsy Decision
Indications for urgent biopsy:
Rapidly rising creatinine (RPGN suspected)
Unexplained acute kidney injury with glomerular signs
Need to confirm crescentic changes
MPGN biopsy findings:
Mesangial proliferation and matrix expansion
Thickened glomerular basement membrane
Subendothelial immune deposits
"Tram-track" appearance on silver stain
RPGN biopsy findings:
Crescents in >50% of glomeruli
Glomerular necrosis and sclerosis
Minimal immune deposits (ANCA-associated)
Acute tubulointerstitial inflammation
High-Yield MCQ Patterns for NEET PG 2026
Pattern 1: Clinical Presentation Differentiation
Classic MPGN question stem:
"A 45-year-old man presents with 6-month history of gradually worsening bilateral leg swelling. BP 160/100 mmHg. Urinalysis shows proteinuria (4+) and microscopic hematuria. Serum C3 is low, C4 normal. Most likely diagnosis?"
Answer approach:
Chronic timeline = MPGN
Low C3, normal C4 = MPGN Type I
Age and presentation fit MPGN
Classic RPGN question stem:
"A 45-year-old man presents with 3-week history of facial puffiness, oliguria, and gross hematuria. Serum creatinine increased from 1.2 to 4.8 mg/dL. ANCA is positive. Most likely diagnosis?"
Answer approach:
Rapid progression = RPGN
ANCA positive = ANCA-associated RPGN
Needs immediate treatment
Pattern 2: Laboratory Value Interpretation
MPGN laboratory pattern:
Persistently low C3
Normal C4 (Type I) or low C4 (Type II)
Proteinuria >3g/day
Slowly rising creatinine
RPGN laboratory pattern:
Normal complement levels
ANCA positive (90% of cases)
Variable proteinuria
Rapidly rising creatinine
Pattern 3: Treatment and Prognosis
MPGN treatment questions:
ACE inhibitors for proteinuria control
Blood pressure management
Immunosuppression controversial
Monitor for progression to ESRD
RPGN treatment questions:
Medical emergency requiring immediate treatment
High-dose corticosteroids
Cyclophosphamide for severe cases
Plasmapheresis if anti-GBM positive
Key Learning Points for NEET PG Success
Memory Tricks
MPGN = "Slow and Low"
Slow: Chronic progression over months
Low: Low complement (especially C3)
RPGN = "Fast and Furious"
Fast: Rapid progression in weeks
Furious: Crescents cause aggressive kidney damage
Common NEET PG Traps
Trap 1: Both conditions can present with edema
Solution: Focus on timeline (chronic vs acute)
Trap 2: Both can have proteinuria and hematuria
Solution: Look for complement levels and ANCA
Trap 3: Age overlap between conditions
Solution: Use clinical course and laboratory findings
Trap 4: Missing the urgency in RPGN
Solution: Rising creatinine = medical emergency
High-Yield Facts for Quick Revision
MPGN Quick Facts:
Peak age: 30-50 years
C3 consumption classic
"Tram-track" on microscopy
Associated with hepatitis C
50% progress to ESRD
RPGN Quick Facts:
Crescents >50% diagnostic
ANCA positive in 90%
Medical emergency
Can lose kidney function in weeks
Requires immediate immunosuppression
Practice with Oncourse AI
Understanding glomerulonephritis differentials requires practice with varied clinical scenarios. Oncourse provides:
1,000+ nephrology MCQs with detailed explanations
Case-based questions mimicking NEET PG patterns
AI-powered explanations for complex differentials
Spaced repetition for long-term retention
Master glomerulonephritis concepts with our comprehensive lessons, practice with targeted MCQs, and reinforce learning with high-yield flashcards.
Advanced Concepts for High Scorers
Secondary Causes in 45-Year-Old Males
MPGN secondary causes:
Hepatitis C infection (most common in adults)
Systemic lupus erythematosus
Chronic liver disease
Malignancy (especially lymphoma)
RPGN secondary causes:
ANCA-associated vasculitis (GPA, MPA, EGPA)
Anti-GBM disease (Goodpasture syndrome)
Systemic lupus erythematosus
Post-infectious (rare in adults)
Prognosis and Management Pearls
MPGN prognosis factors:
Poor prognosis: Nephrotic syndrome, hypertension, reduced GFR at presentation
Better prognosis: Isolated proteinuria, normal blood pressure
10-year kidney survival: Approximately 50%
RPGN prognosis factors:
Critical factor: Time to treatment initiation
Poor prognosis: >50% crescents, severe acute tubular necrosis
Recovery potential: If treated early, some patients recover significant kidney function
Histopathological Pearls
MPGN electron microscopy:
Type I: Subendothelial and mesangial deposits
Type II: Dense deposit disease (intramembranous)
Type III: Subepithelial and subendothelial deposits
RPGN types by immunofluorescence:
Type I: Linear IgG (anti-GBM)
Type II: Granular IgG (immune complex)
Type III: Pauci-immune (ANCA-associated)
Frequently Asked Questions
What is the most important distinguishing feature between MPGN and RPGN in a 45-year-old man?
The timeline of progression is crucial. MPGN develops over months to years with slowly declining kidney function, while RPGN progresses rapidly over days to weeks with doubling of serum creatinine within 3 months.
Why are complement levels important in this differential diagnosis?
Low C3 complement levels are characteristic of MPGN, particularly Type I. RPGN typically has normal complement levels. This laboratory finding can be diagnostic when combined with clinical presentation.
How quickly should treatment be initiated if RPGN is suspected?
RPGN is a medical emergency requiring immediate treatment within hours to days of diagnosis. Delay in treatment can result in irreversible kidney damage and progression to end-stage renal disease.
What role does ANCA testing play in this differential?
ANCA is positive in 90% of RPGN cases (ANCA-associated vasculitis) but is typically negative in MPGN. A positive ANCA with rapid kidney function decline strongly suggests RPGN.
Can both conditions present with nephrotic syndrome?
Yes, both MPGN and RPGN can present with nephrotic syndrome (proteinuria >3.5g/day, hypoalbuminemia, edema). The key difference is the timeline and associated laboratory findings rather than the presence of nephrotic syndrome itself.
What is the significance of crescents in kidney biopsy?
Crescents in >50% of glomeruli define RPGN and indicate active glomerular inflammation with potential for rapid kidney function loss. MPGN typically shows proliferative changes without extensive crescent formation.
Master nephrology differentials with confidence. The key to NEET PG success lies in understanding the subtle differences that distinguish similar presentations.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.