Back
12 kg Child Dehydration Management: Holliday-Segar Formula for USMLE Step 2 CK Pediatrics 2026
Master the Holliday-Segar formula for pediatric fluid management. Complete guide to 12 kg child dehydration scenarios, 4-2-1 rule calculations, and clinical decisions for USMLE Step 2 CK success.
12 kg Child Dehydration Management: Holliday-Segar Formula for USMLE Step 2 CK Pediatrics 2026
You are probably staring at a pediatric fluid management vignette right now. A 12-month-old, 12 kg child presents with vomiting and diarrhea for 2 days. Mild dehydration. Calculate maintenance fluids. Your mind goes blank on the Holliday-Segar formula.
Here's the thing about USMLE Step 2 CK — pediatric fluid questions appear on almost every form. The 12 kg child scenario is their absolute favorite. Not 8 kg. Not 15 kg. Always 12 kg. Because it tests both parts of the 4-2-1 rule in one clean calculation.
This isnt just about memorizing formulas. Step 2 CK wants you to think clinically. When do you choose oral rehydration over IV? Why D5 0.45% NaCl instead of normal saline? Which wrong answers trap most students?
Walk through this once. Get it right on test day.
Understanding the Holliday-Segar Method for Maintenance Fluid Calculation
The Holliday-Segar method calculates how much fluid a child needs per day to maintain normal body functions. Not replacement fluid for losses. Not resuscitation fluid for shock. Just baseline maintenance.
Two ways to calculate this: hourly rate (4-2-1 rule) or daily volume (100-50-20 rule). Step 2 CK typically gives you hourly rates, so master the 4-2-1 rule first.
The 4-2-1 Rule Breakdown
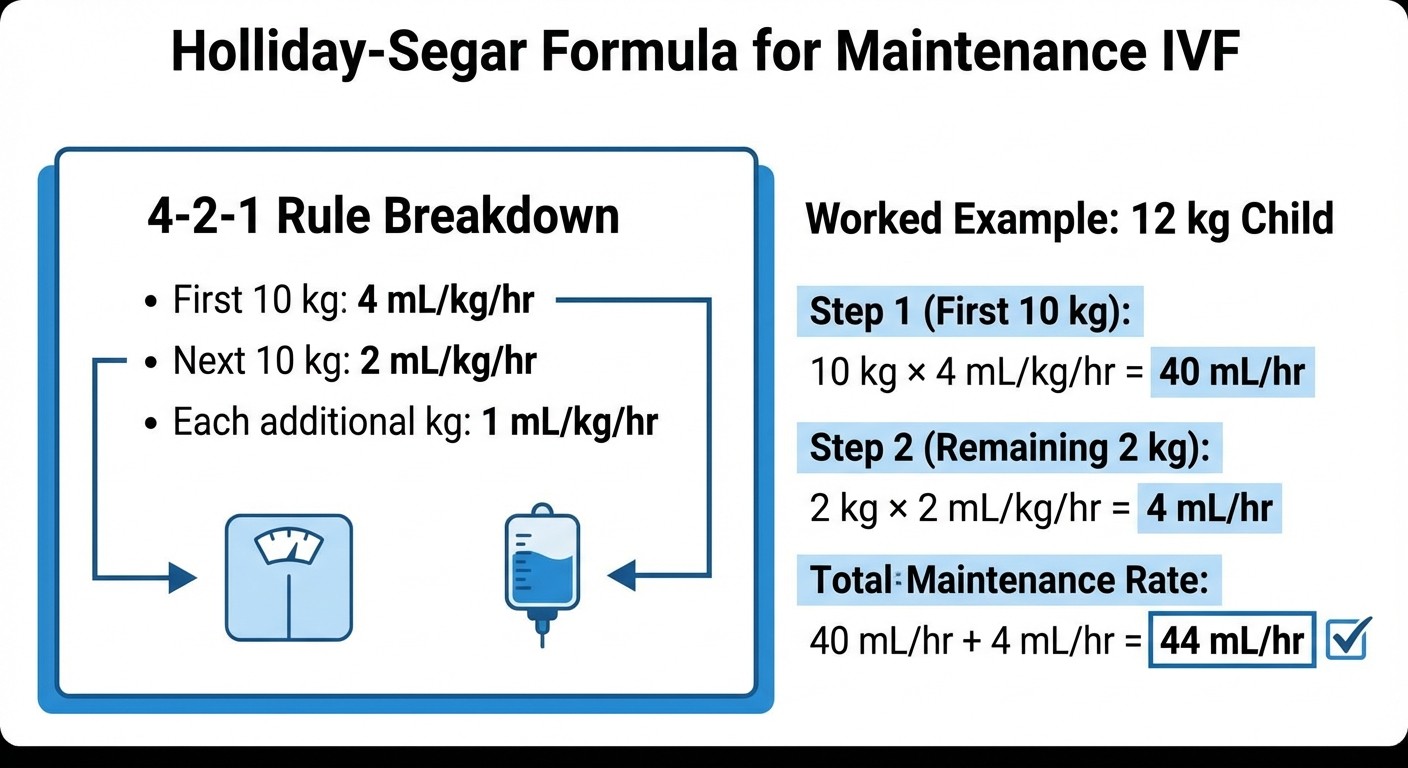
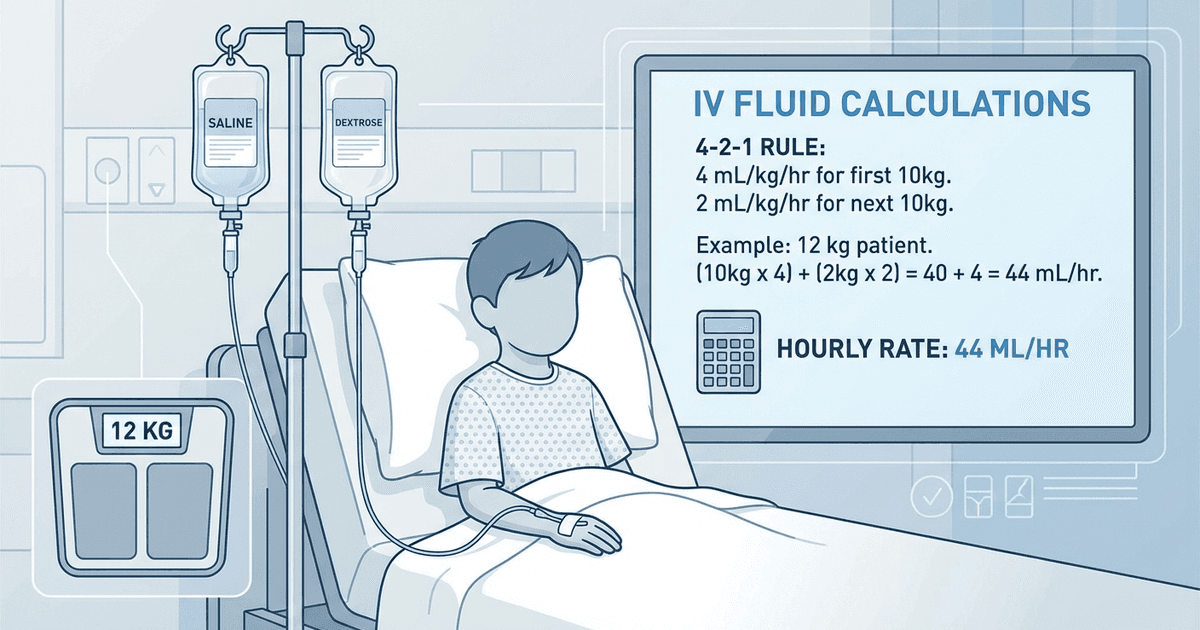
The 4-2-1 rule calculates maintenance fluid needs per hour:
First 10 kg: 4 mL/kg/hr
Next 10 kg: 2 mL/kg/hr
Each additional kg: 1 mL/kg/hr
For a 12 kg child:
First 10 kg: 10 kg × 4 mL/kg/hr = 40 mL/hr
Remaining 2 kg: 2 kg × 2 mL/kg/hr = 4 mL/hr
Total maintenance: 40 + 4 = 44 mL/hr
That's 44 mL/hr × 24 hours = 1,056 mL/day (approximately 1 L/day).
The calculation lives in your pediatric fluid and electrolyte management lessons, but you need it automatic by test day. When Oncourse AI's Synapses feature surfaces your spaced repetition flashcards on the 4-2-1 rule, the formula becomes muscle memory — exactly what you need when Step 2 CK time pressure hits.
The Classic 12 kg Child: Complete Worked Example
Here's how Step 2 CK frames the question:
> A 12-month-old child weighing 12 kg presents to the emergency department with a 2-day history of vomiting and diarrhea. Physical examination reveals mild dehydration with slightly dry mucous membranes and decreased skin turgor. Vital signs are stable. What is the appropriate maintenance fluid rate?
Step 1: Calculate maintenance using 4-2-1 rule
First 10 kg: 40 mL/hr
Remaining 2 kg: 4 mL/hr
Maintenance rate: 44 mL/hr
Step 2: Assess dehydration severity
Mild dehydration = 3-5% weight loss. Clinical signs match. No shock, normal vital signs.
Step 3: Calculate replacement needs
Mild dehydration: 30-50 mL/kg over 24 hours
For 12 kg child: 360-600 mL over 24 hours = 15-25 mL/hr additional
Step 4: Total fluid requirement
Maintenance: 44 mL/hr
Replacement: ~20 mL/hr (using midpoint)
Total: 64 mL/hr
Choosing Between Oral Rehydration and IV Fluids
This is where Step 2 CK gets clinical. The decision isnt automatic.
Oral Rehydration Therapy (ORT) Criteria
Use ORT when:
Mild to moderate dehydration (≤10%)
Child can keep fluids down
Normal mental status
No severe electrolyte abnormalities
ORT volume: 75 mL/kg over 4 hours for mild dehydration
For 12 kg child: 75 × 12 = 900 mL over 4 hours = 225 mL/hr initially
This high rate replaces losses quickly, then you drop to maintenance.
IV Fluid Indications
Switch to IV when:
Persistent vomiting
Severe dehydration (>10%)
Shock or altered mental status
Failed ORT trial
Electrolyte abnormalities requiring correction
Step 2 CK loves the "failed ORT" scenario. Child tries oral rehydration for 2 hours, continues vomiting. Now what? IV fluids.
Fluid Type Selection: The Clinical Decision Tree
Not all fluids are created equal. Step 2 CK tests your understanding of when to use what.
Normal Saline (0.9% NaCl) First
Always start with isotonic saline for:
Any degree of shock
Severe dehydration
Initial resuscitation
Why? Isotonic fluid stays in the intravascular space. Hypotonic fluid shifts to cells, worsening hypotension.
Rule: Give 20 mL/kg normal saline bolus if any signs of shock, then reassess.
Maintenance Fluids: D5 0.45% NaCl
Once stabilized, switch to hypotonic maintenance fluid:
D5 0.45% NaCl (dextrose 5% in half-normal saline)
Provides glucose for metabolism
Hypotonic to match normal daily losses
For our 12 kg child with mild dehydration and stable vitals: start with D5 0.45% NaCl at calculated rate (64 mL/hr).
When working through these clinical decisions, Oncourse AI's Clinical Rounds feature simulates exactly this type of USMLE vignette. You see a dehydrated 12 kg child in the ER, choose your history questions, order labs, and select treatment. The 4-step format (History → Tests → Diagnosis → Treatment) mirrors Step 2 CK clinical reasoning.
High-Yield Clinical Scenarios for USMLE Step 2 CK
Scenario 1: The Shock Red Herring
> 12 kg child, severe dehydration, heart rate 150, blood pressure 80/50. Calculate maintenance fluids.
Wrong thinking: Jump to Holliday-Segar calculation. Right thinking: This child needs resuscitation, not maintenance calculation. Give 20 mL/kg normal saline bolus (240 mL) immediately. Maintenance comes after stabilization.
Step 2 CK wants you to prioritize. Sick child = resuscitation first.
Scenario 2: The ORS Success Story
> 12 kg child, mild dehydration, tolerating oral fluids. Mother asks about IV placement.
Wrong answer: "IV fluids are more reliable." Right answer: ORT is first-line for mild-moderate dehydration in children who can drink. More comfortable, equally effective, fewer complications.
Scenario 3: The Electrolyte Trap
> 12 kg child, moderate dehydration, sodium 120 mEq/L. Appropriate initial fluid?
Wrong answer: 3% hypertonic saline (too aggressive). Right answer: Normal saline initially. Hyponatremia in dehydrated children is usually dilutional from ADH release. Correct volume first, sodium follows.
Common Wrong Answers and Why Students Pick Them
"Double the maintenance rate"
Some students see dehydration and think "more fluid = better." Wrong. You calculate maintenance separately from replacement. Doubling maintenance gives too much sodium, not enough free water.
"Use D5W for maintenance"
D5W (dextrose in water) has no electrolytes. Fine for short procedures, dangerous for maintenance. Children need sodium and chloride for normal losses.
"Start with lactated Ringer's"
LR is great for trauma, wrong for pediatric maintenance. Too much potassium for a child who hasnt eaten. Stick to D5 0.45% NaCl.
"Calculate based on adult formulas"
Adult maintenance is ~25-30 mL/kg/day. Pediatric is much higher (~100 mL/kg/day for first 10 kg) because children have higher metabolic rates and larger surface area to weight ratios.
When you miss these types of questions, Oncourse's Explanation Chat activates instantly — breaking down not just why the right answer works, but why each wrong answer fails. For Holliday-Segar MCQs, this means understanding the clinical reasoning behind fluid type selection, not just memorizing formulas.
Special Considerations in USMLE Step 2 CK
Age-Specific Factors
Infants (<1 year): Higher fluid needs relative to weight. More susceptible to dehydration and electrolyte shifts. Toddlers (1-3 years): The classic Step 2 CK demographic. Old enough to show clear dehydration signs, young enough to need careful monitoring.
Monitoring Parameters
Step 2 CK expects you to know when to reassess:
Every 2 hours for severe dehydration
Every 4-6 hours for mild-moderate dehydration
Watch urine output (goal: 1-2 mL/kg/hr)
Monitor electrolytes every 6-12 hours
Red Flags That Change Management
Persistent vomiting: Switch from ORT to IV
Altered mental status: Aggressive IV resuscitation
Poor urine output: Increase fluid rate or investigate other causes
Worsening electrolytes: Consider specialist consultation
Quick Reference Table
Dehydration Severity | Clinical Signs | Fluid Choice | Rate |
|---|---|---|---|
Mild (3-5%) | Slightly dry mucous membranes | ORT preferred | 75 mL/kg over 4h |
Moderate (6-9%) | Decreased skin turgor, sunken eyes | ORT or IV | 100 mL/kg over 4h |
Severe (>10%) | Shock, altered mental status | IV only | 20 mL/kg bolus + maintenance |
For your Step 2 CK pediatric emergency management practice questions, this table covers 90% of fluid scenarios.
Frequently Asked Questions
How do you calculate maintenance fluids for a 12 kg child?
Use the 4-2-1 rule: First 10 kg gets 4 mL/kg/hr (40 mL/hr), remaining 2 kg gets 2 mL/kg/hr (4 mL/hr). Total maintenance = 44 mL/hr.
When should you use normal saline vs D5 0.45% NaCl in pediatric dehydration?
Normal saline for resuscitation and severe dehydration. D5 0.45% NaCl for maintenance once the child is stable. Never use hypotonic fluids for initial resuscitation.
What's the difference between maintenance and replacement fluids?
Maintenance fluids replace normal daily losses (breathing, sweating, urine). Replacement fluids correct existing dehydration. You calculate and give both separately.
How much ORS should a 12 kg child with mild dehydration receive?
75 mL/kg over 4 hours for mild dehydration = 900 mL over 4 hours, then switch to maintenance ORS at 150 mL/kg/day.
When do you switch from oral to IV rehydration?
Switch to IV if the child cant keep fluids down, shows signs of severe dehydration, has altered mental status, or fails a trial of ORT.
What are the most common USMLE mistakes with Holliday-Segar calculations?
Using adult fluid rates, choosing wrong fluid types (D5W or LR for maintenance), calculating only maintenance without replacement, and not prioritizing resuscitation in shock.
The 12 kg child dehydration scenario will show up on your Step 2 CK. Master the Holliday-Segar method, know when to choose ORT vs IV, and understand fluid type selection. These arent just formulas — they're clinical decisions that separate good scores from great ones.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.