Back
USMLE Step 3 CCS Cases: How Clinical Rounds + Explanation Chat Changes Medical Revision
Master USMLE Step 3 CCS cases with clinical rounds thinking, AI explanation chat, and performance analytics. Transform your case management revision from passive review to active clinical reasoning.

USMLE Step 3 CCS Cases: How Clinical Rounds + Explanation Chat Changes Medical Revision
You are probably used to MCQ revision—read, recall, select, move on. But USMLE Step 3 CCS cases demand something completely different. Each case unfolds over 10-20 minutes of simulated time, where a patient's condition changes based on your decisions. You dont just need to know the right diagnosis; you need to sequence orders, monitor responses, and adjust your approach as time progresses.
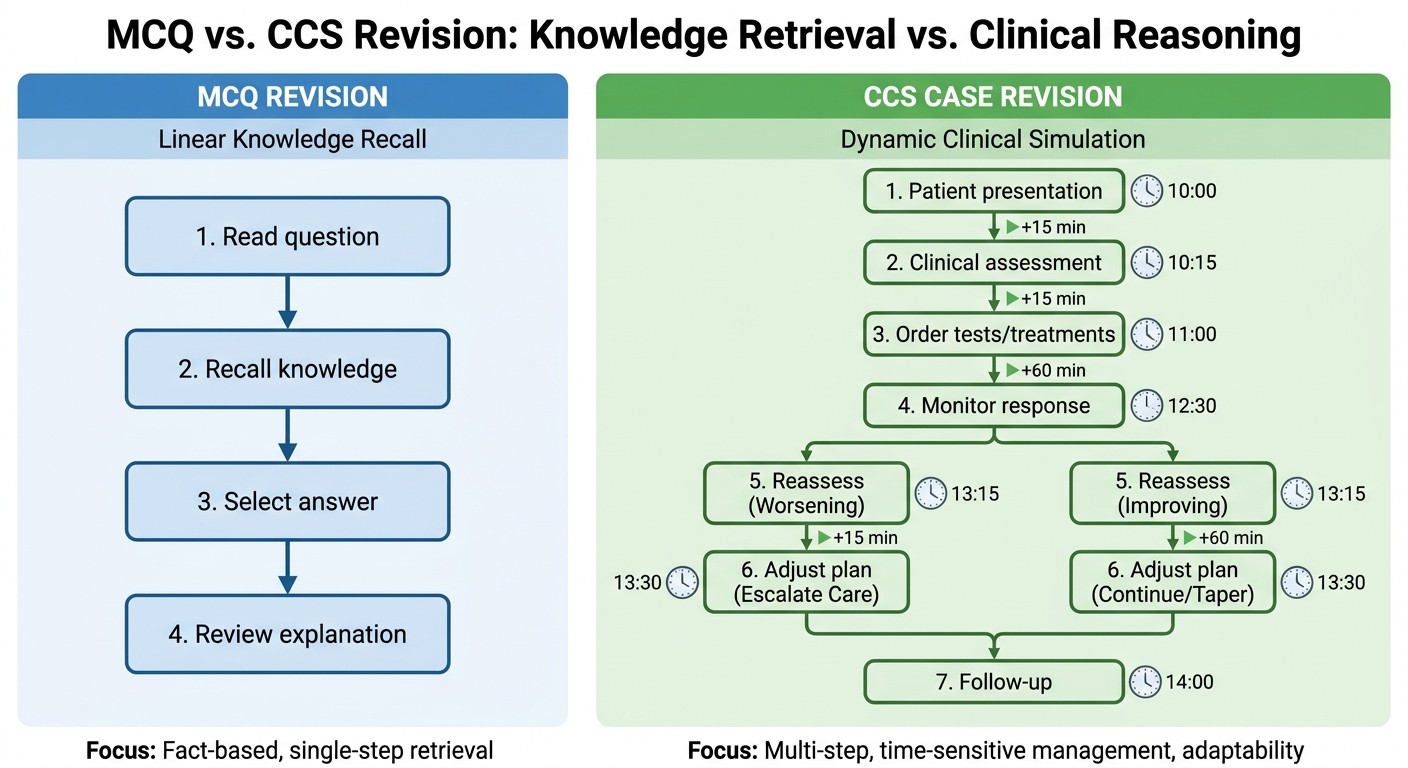
The difference? MCQ revision tests knowledge recall. CCS revision requires clinical reasoning under time pressure—exactly what you'll face as a resident managing real patients.
Here's what changes when you approach CCS cases like clinical rounds instead of traditional study sessions, and how explanation chat transforms every missed case into a learning opportunity.
Why CCS Revision Differs from MCQ Revision
Traditional MCQ study follows a linear path: question → knowledge recall → answer → explanation. You can review 50 questions in an hour and feel productive.
CCS cases work differently. According to the official USMLE guidelines, each case is "a dynamic, interactive simulation" where patient conditions change based on your management decisions and underlying disease progression. You're not just selecting from predetermined options—you're typing free-text orders and making real-time clinical decisions.
The scoring reflects this complexity. CCS awards points across six domains: Diagnosis (20%), Therapy (40%), Monitoring (15%), Timing (10%), Sequencing (10%), and Location (5%). Miss the timing on antibiotics for sepsis, and you lose points even with the correct diagnosis and treatment choice.
This means your revision needs to mirror actual patient management, not just knowledge testing.
How Clinical Rounds Thinking Transforms CCS Preparation
Clinical rounds follow a structured approach: assessment, plan, implementation, reassessment, adjustment. This same thinking pattern directly applies to CCS cases.
Traditional study approaches focus on "what's the diagnosis?" Clinical rounds thinking asks: "What's the patient's current status, what needs immediate attention, and what's my next move?"

The Rounds-Style CCS Approach
Initial Stabilization (First 60 seconds)
Start every case with the ABC framework, regardless of the presenting complaint. Order continuous monitoring, establish IV access, and check vitals. This isn't about the diagnosis—it's about patient safety. The clinical rounds mentality is: "Stabilize first, then investigate."
When practicing with Oncourse AI Clinical Rounds, students develop this systematic approach through case-style scenarios that mirror real ward round decision-making.
Focused Assessment Phase
After stabilization, gather targeted history and physical findings. Dont order every possible test—focus on high-yield information that changes management. In clinical rounds, you present relevant findings, not exhaustive lists.
Diagnostic and Treatment Orders
This is where clinical rounds thinking shines. Instead of ordering tests randomly, sequence them based on urgency and diagnostic yield. Critical interventions (oxygen, IV antibiotics for sepsis, cardiac monitoring for chest pain) come first. Confirmatory tests follow.
Reassessment and Monitoring
The key difference between MCQ and CCS thinking: you must actively monitor response to treatment. Order repeat vitals, reassess symptoms, and adjust based on patient response. This mirrors real rounds where you check how patients responded to overnight interventions.
Patient Counseling and Disposition
CCS cases often include counseling and discharge planning components. Clinical rounds always end with "what's the plan?"—and CCS scoring rewards appropriate follow-up planning and patient education.
Common CCS Traps and How Rounds Thinking Avoids Them
The Shotgun Testing Trap
Many students order comprehensive metabolic panels, complete imaging workups, and multiple consultations immediately. Clinical rounds thinking asks: "What specific information do I need to make the next decision?" Order targeted tests that change management.
The Diagnosis Delay Trap
Waiting for test results before starting treatment can cost points in time-sensitive cases. In clinical rounds, you often start empiric treatment for high-probability diagnoses while awaiting confirmation. The same applies to CCS—start antibiotics for likely sepsis while blood cultures are pending.
The Static Management Trap
After initial orders, many students advance time without reassessing. Clinical rounds involve continuous evaluation. In CCS, check response to treatments, adjust doses, and modify plans based on patient trajectory.
How Explanation Chat Fills CCS Learning Gaps
Traditional CCS review shows you the "correct" sequence of orders but doesnt explain the clinical reasoning behind timing decisions, order prioritization, or why certain approaches score better.
Explanation chat changes this. When you miss points on a CCS case, you can ask specific questions about your management decisions: "Why did starting antibiotics at 15 minutes instead of 5 minutes cost points?" or "What monitoring parameters should I have ordered for this heart failure case?"
The key advantage? Instead of generic explanations, you get answers tailored to your specific management gaps. If you consistently score poorly on monitoring in respiratory cases, explanation chat can walk through exactly which parameters to track and when to reassess.
Using Oncourse AI's Rezzy explanation chat after CCS practice, students can dig deeper into management reasoning, understanding not just what to do but why the timing and sequencing matter for scoring.
Reviewing Missed CCS Cases Effectively
Immediate Post-Case Analysis
Right after completing a case, review your order sequence chronologically. Identify where you lost points in each scoring domain. Dont just look at missed diagnoses—examine timing, monitoring gaps, and inappropriate orders.
Domain-Specific Review
Break down your performance by scoring domain. Weak in Therapy? Focus on evidence-based treatment protocols. Struggling with Timing? Practice recognizing time-sensitive interventions. Missing Monitoring points? Develop checklists for reassessment parameters.
Pattern Recognition
Track your performance across case types. Are you consistently missing points in cardiac cases? Struggling with sepsis management timing? This data-driven approach mimics how clinical performance is evaluated in residency.
The performance analytics approach helps identify specific weak areas rather than general "CCS practice." When you know you're missing 60% of monitoring points in respiratory cases, your next study session has clear focus.
Building CCS Confidence Through Systematic Practice
Start with High-Frequency Cases
Begin CCS practice with common presentations: chest pain, shortness of breath, abdominal pain, altered mental status. Master the systematic approach on bread-and-butter cases before tackling rare diagnoses.
Practice Time Management
Real CCS cases have varying time limits. Practice completing cases efficiently without rushing critical decisions. The clinical rounds approach helps—you're thinking systematically, not scrambling through random orders.
Simulate Real Testing Conditions
Practice CCS cases in blocks, just like the actual exam. Dont review explanations between cases—complete 3-4 cases, then review your performance patterns. This builds stamina and maintains focus under pressure.
The Integration Advantage: Rounds + Chat + Analytics
When you combine clinical rounds thinking, explanation chat, and performance analytics, CCS revision becomes targeted and efficient. You're not just practicing cases—you're building systematic clinical reasoning skills.
The approach works because it mirrors how you'll actually manage patients as a resident. Every case becomes practice for real clinical decision-making, not just test-taking strategy.
Students using this integrated approach report feeling more confident about CCS cases because they're thinking like clinicians, not test-takers. The systematic rounds approach reduces anxiety and improves performance across all scoring domains.
Frequently Asked Questions
How long should I spend reviewing each CCS case?
Spend 10-15 minutes reviewing each completed case. Focus on order timing, missed monitoring opportunities, and management gaps. Dont just review incorrect cases—analyze your high-scoring cases to understand what worked.
Should I memorize order sets for different conditions?
Avoid rigid memorization. Instead, understand the clinical reasoning behind common order patterns. Focus on stabilization principles, evidence-based treatments, and appropriate monitoring rather than fixed protocols.
How important is typing speed for CCS performance?
Typing speed matters less than systematic thinking. The CCS interface includes auto-complete and common order shortcuts. Practice using the software efficiently, but dont sacrifice clinical reasoning for typing speed.
Can I change my management plan mid-case?
Yes, and you should. CCS rewards dynamic management based on patient response. If initial treatment isnt working or new information emerges, adjust your approach. This mirrors real clinical practice.
How do I know if Im monitoring enough parameters?
Use the clinical rounds approach: after each intervention, ask "How will I know if this is working?" For cardiac medications, monitor heart rate and blood pressure. For antibiotics, track fever and white count. For respiratory treatments, follow oxygen saturation and respiratory rate.
What if I finish a CCS case early?
Use remaining time for patient counseling, discharge planning, or preventive care measures. CCS scoring includes these components, and they often differentiate high-scoring from average performance.
Prepare smarter with Oncourse AI—adaptive MCQs, clinical reasoning cases, and AI explanations built for USMLE Step 3. Download free on Android and iOS.