USMLE Step 2 CK Musculoskeletal & Orthopedics Study Guide 2026: High-Yield Topics, Clinical Vignettes and Exam Strategy
Master USMLE Step 2 CK musculoskeletal and orthopedics with this comprehensive guide covering fractures, arthritis differentials, bone tumors, and clinical vignette strategies for 2026.

USMLE Step 2 CK Musculoskeletal & Orthopedics Study Guide 2026: High-Yield Topics, Clinical Vignettes and Exam Strategy
You've mastered cardiology, crushed pulmonology, and dominated infectious diseases. Now comes the MSK block — and honestly, it feels different. Unlike other Step 2 CK systems where pattern recognition rules, musculoskeletal medicine demands surgical thinking mixed with medical management. One vignette asks you to differentiate septic arthritis from crystal arthropathy (medical), the next wants you to know when a scaphoid fracture needs surgical fixation (surgical).
Here's what makes MSK challenging: the exam spans pediatric orthopedics, adult trauma, rheumatology, sports medicine, and oncology. A 45-year-old with knee pain could be osteoarthritis, meniscus tear, or osteosarcoma. The demographics, mechanism, and imaging details matter — miss one clue and you pick the wrong answer.
This guide breaks down the 47 highest-yield MSK topics for Step 2 CK, the clinical vignette patterns you'll see, and the exam strategy that converts study time into points. We'll walk through fracture classifications, arthritis differentials, and the pediatric orthopedic conditions that show up every single exam cycle.
How MSK Appears on USMLE Step 2 CK vs Step 1
Step 1 tested MSK pathophysiology — you memorized osteoblast vs osteoclast functions and growth plate anatomy. Step 2 CK tests clinical decision-making. You'll see 8-12 MSK questions (roughly 3% of the exam), and they fall into three categories:
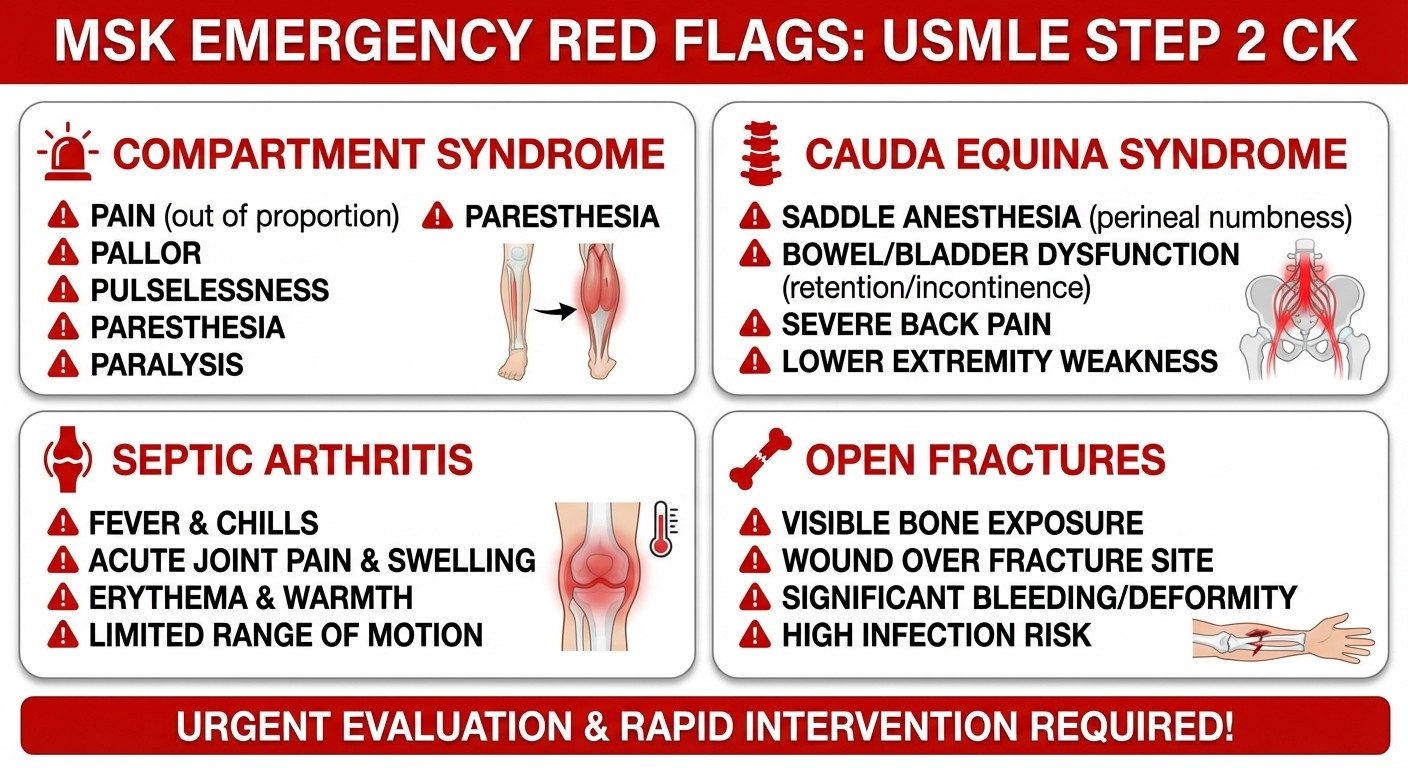
Trauma/Emergency (40% of MSK questions): Compartment syndrome, open fractures, cauda equina syndrome, septic arthritis. These test your ability to recognize surgical emergencies and know the immediate next step. Chronic Conditions (35%): Osteoarthritis vs rheumatoid arthritis vs crystal arthropathy differentials, back pain workup (herniated disc vs spinal stenosis), bone tumors in different age groups. Pediatric Orthopedics (25%): Developmental dysplasia of the hip (DDH), slipped capital femoral epiphysis (SCFE), Legg-Calve-Perthes disease, and Osgood-Schlatter disease. Age demographics are key here.
The questions are longer than Step 1 — expect 4-6 sentences with specific imaging findings described in text (since they can't show actual X-rays). Time management becomes crucial when you're parsing "comminuted fracture of the distal radius with dorsal angulation" while the clock ticks.
High-Yield Fracture Patterns and Mechanisms
Fractures make up 30% of Step 2 CK MSK questions, and the exam loves eponymous fractures with specific mechanisms. Here are the must-know patterns:
Wrist and Forearm Fractures
Colles Fracture: Most common wrist fracture. Mechanism: fall on outstretched hand (FOOSH). X-ray finding: distal radius fracture with dorsal angulation ("dinner fork deformity"). Demographics: postmenopausal women. Treatment: closed reduction and casting for nondisplaced, surgical fixation for displaced. Smith Fracture: Less common but high-yield. Mechanism: fall on flexed wrist. X-ray: distal radius fracture with volar angulation (opposite of Colles). Always requires surgical fixation due to instability. Scaphoid Fracture: High-yield because it's commonly missed. Mechanism: FOOSH with radial deviation. Clinical finding: tenderness in anatomical snuffbox. X-ray: often normal initially (15% false negative rate). Key point: if clinically suspected, treat with thumb spica cast even with negative X-ray. Oncourse's spaced repetition flashcards surface these fracture patterns when you need to review them, preventing the "I studied this last month" memory gaps that cost points.
Hip Fractures
Femoral Neck vs Intertrochanteric: Age: >65 years. Mechanism: low-energy fall. Clinical: shortened, externally rotated leg with inability to bear weight.
Key differential: femoral neck fractures disrupt blood supply (risk of avascular necrosis), while intertrochanteric fractures maintain blood supply. Treatment: femoral neck gets hemiarthroplasty or total hip replacement; intertrochanteric gets ORIF with intramedullary nail.
Stress Fractures: High-yield in young athletes. Classic scenario: military recruit with hip pain and normal X-ray. MRI shows fracture line. Treatment: activity modification and gradual return to weight-bearing.
Vertebral Compression Fractures
Demographics: osteoporotic women >70. Mechanism: minimal trauma (coughing, bending forward). Clinical: acute back pain, kyphotic deformity. X-ray: "wedge-shaped" vertebral body on lateral view. Red flags for malignancy: age <50, weight loss, neurologic symptoms.
Arthritis Differentials: The Step 2 CK Classics
Arthritis questions appear in 25% of MSK vignettes, and the exam tests your ability to differentiate based on demographics, joint involvement, lab findings, and synovial fluid analysis.
Crystal Arthropathy vs Septic Arthritis
This is the highest-yield arthritis differential on Step 2 CK. Both present with acute monoarticular arthritis, but the labs and demographics differ:
Gout:
Demographics: middle-aged men, history of alcohol use or diuretics
Joint: first metatarsophalangeal joint (70% of initial episodes)
Labs: elevated uric acid (but normal during acute attack in 30%)
Synovial fluid: WBC 2,000-50,000, needle-shaped uric acid crystals, negative polarization
Treatment: NSAIDs, colchicine, or corticosteroids
Pseudogout (CPPD):
Demographics: elderly patients, often with prior knee surgery
Joint: knee (50%), wrist, ankle
Labs: normal uric acid
Synovial fluid: WBC 2,000-50,000, rectangular calcium pyrophosphate crystals, positive polarization
X-ray: chondrocalcinosis (calcification of menisci/joint capsules)
Septic Arthritis:
Demographics: any age, but higher risk with diabetes, immunosuppression, prosthetic joints
Joint: knee (50%), then hip, shoulder, ankle
Labs: elevated ESR/CRP, blood cultures positive in 50%
Synovial fluid: WBC >100,000 (85% polymorphs), positive gram stain/culture
Treatment: immediate arthrocentesis + IV antibiotics, surgical drainage for hip/shoulder
When a vignette describes acute knee pain, use the synovial fluid WBC count as your discriminator: >100,000 = septic until proven otherwise.
Osteoarthritis vs Rheumatoid Arthritis
Osteoarthritis:
Demographics: >50 years, female predominance
Joints: weight-bearing joints (knees, hips), DIP/PIP joints of hands
Pattern: asymmetric joint involvement
Labs: normal ESR/CRP, negative rheumatoid factor
X-ray: joint space narrowing, osteophytes, subchondral sclerosis
Treatment: NSAIDs, weight loss, physical therapy; intra-articular corticosteroids for flares
Rheumatoid Arthritis:
Demographics: 30-50 years, female 3:1 predominance
Joints: MCP/PIP joints (spares DIPs), wrists, knees; symmetric involvement
Pattern: morning stiffness >1 hour, improvement with activity
Labs: elevated ESR/CRP, positive rheumatoid factor (70%), positive anti-CCP antibodies (95% specific)
X-ray: joint space narrowing, marginal erosions, osteopenia
Treatment: methotrexate + short-term corticosteroids, biologics for severe disease
Compartment Syndrome: The MSK Emergency
Compartment syndrome accounts for 15% of MSK emergency questions and tests your ability to recognize a surgical emergency based on clinical findings.
Mechanism: Increased pressure within fascial compartments, most commonly after tibial fractures, crush injuries, or prolonged compression. Clinical Findings (5 P's): Pain (especially passive stretch), Pallor, Paresthesias, Paralysis, Pulselessness. But here's the key: pulselessness is a late finding. If you wait for absent pulses, you've waited too long. Highest Yield Clinical Sign: Pain with passive stretch of muscles in the affected compartment. For forearm compartment syndrome, passive finger extension causes severe pain. For leg compartment syndrome, passive toe dorsiflexion causes severe pain. Diagnosis: Compartment pressure >30 mmHg or delta pressure <30 mmHg (difference between diastolic BP and compartment pressure). But don't wait for pressure measurements if clinical suspicion is high. Treatment: Immediate fasciotomy. This is a surgical emergency — delayed treatment leads to muscle necrosis, contractures, and limb loss.
Step 2 CK vignette pattern: young patient with tibial fracture, increasing pain despite adequate analgesia, pain with passive toe movement. Next best step: emergent fasciotomy.
Bone Tumors: Age Demographics Drive Diagnosis
Bone tumor questions appear in 10% of MSK vignettes, and age is the strongest predictor of tumor type. The exam tests your knowledge of which tumors occur in which decades.
Primary Bone Tumors by Age
Ages 10-20: Osteosarcoma and Ewing Sarcoma Osteosarcoma:
Demographics: adolescent growth spurt, male predominance
Location: metaphysis of long bones (distal femur 40%, proximal tibia 20%)
X-ray: mixed sclerotic/lytic lesion with "sunburst" pattern, soft tissue mass
Labs: elevated alkaline phosphatase, elevated LDH
Treatment: neoadjuvant chemotherapy + limb salvage surgery
Ewing Sarcoma:
Demographics: age 10-20, slight male predominance
Location: diaphysis of long bones, flat bones (pelvis, ribs)
X-ray: "onion skin" periosteal reaction, soft tissue mass
Labs: normal alkaline phosphatase, elevated ESR
Treatment: chemotherapy + radiation ± surgery
Ages 20-40: Giant Cell Tumor and Chondrosarcoma
Giant Cell Tumor:
Location: epiphysis of long bones (distal femur, proximal tibia)
X-ray: "soap bubble" lytic lesion extending to subchondral bone
Treatment: curettage and bone grafting
Chondrosarcoma:
Location: axial skeleton (pelvis, ribs, scapula)
X-ray: chondroid matrix calcification ("rings and arcs")
Treatment: wide surgical resection (resistant to chemo/radiation)
Ages >40: Metastatic Disease
Most Common Primary Sites: Breast, lung, kidney, thyroid, prostate ("BLT with a Kosher Pickle"). Imaging Patterns:
Blastic metastases: prostate, breast
Lytic metastases: lung, kidney, thyroid
Mixed: breast
When a Step 2 CK vignette presents a >50-year-old with bone pain and a lesion on imaging, think metastatic disease first. Order bone scan to assess for multiple lesions, then search for primary tumor.
Back Pain: Surgical vs Medical Management
Back pain questions test your ability to differentiate mechanical causes (herniated disc, spinal stenosis) from medical causes (compression fracture, malignancy) and know when surgical intervention is indicated.
Herniated Disc vs Spinal Stenosis
Herniated Disc:
Demographics: 30-50 years, often with lifting/twisting injury
Clinical: radicular pain worse with sitting/bending forward, positive straight leg raise
Level: L5-S1 (45%) causes weakness of plantar flexion and loss of Achilles reflex; L4-L5 (35%) causes foot drop and decreased sensation in first web space
MRI: disc herniation with nerve root compression
Treatment: NSAIDs + physical therapy initially, steroid injection for persistent symptoms, surgery if progressive weakness or >6 weeks of symptoms
Spinal Stenosis:
Demographics: >60 years, often bilateral symptoms
Clinical: neurogenic claudication (leg pain with walking, relieved by sitting/flexing forward), "shopping cart sign" (can walk further when leaning on cart)
MRI: central canal narrowing <10mm, ligamentum flavum hypertrophy
Treatment: physical therapy, epidural steroid injections, laminectomy for severe symptoms
Cauda Equina Syndrome: The Neurosurgical Emergency
Clinical Findings: Bilateral leg pain/weakness, saddle anesthesia, bowel/bladder dysfunction (retention > incontinence initially). Mechanism: Central disc herniation, epidural abscess, or tumor compression below L2. Treatment: Emergent MRI + neurosurgical decompression within 24 hours. Delayed treatment leads to permanent neurologic deficits.
Oncourse's AI tutor helps you nail these differentials by explaining exactly which clinical clue you missed when you select "herniated disc" for a spinal stenosis case. Instead of just seeing the right answer, you understand why "shopping cart sign" points specifically to stenosis, converting your miss into pattern recognition for the next similar vignette.
Pediatric Orthopedics: Age-Based Pattern Recognition
Pediatric orthopedic questions appear in 20% of MSK vignettes and rely heavily on age demographics. The exam tests your knowledge of which conditions occur in which age groups and when surgical intervention is indicated.
Hip Disorders by Age
Developmental Dysplasia of Hip (DDH):
Age: newborn to 6 months
Risk factors: female, breech presentation, family history, firstborn
Clinical: asymmetric hip abduction, Galeazzi sign (unequal knee heights), positive Barlow/Ortolani tests
Imaging: ultrasound <6 months, X-ray >6 months
Treatment: Pavlik harness <6 months, surgical reduction if diagnosed late
Legg-Calve-Perthes Disease:
Age: 4-8 years (peak age 6)
Demographics: male 4:1, bilateral in 10%
Pathophysiology: avascular necrosis of femoral head
Clinical: limp, hip/knee pain worse with activity
X-ray: sclerosis and flattening of femoral head
Treatment: activity modification, abduction bracing, surgery for severe cases
Slipped Capital Femoral Epiphysis (SCFE):
Age: 10-16 years (during growth spurt)
Demographics: overweight boys, African American predominance
Clinical: hip/knee pain, externally rotated leg, limp
X-ray: "ice cream falling off the cone" on lateral view
Treatment: immediate surgical pinning to prevent further slippage
Knee Pain in Adolescents
Osgood-Schlatter Disease:
Age: 10-15 years during growth spurt
Demographics: active adolescents (jumping sports)
Clinical: anterior knee pain, tenderness over tibial tuberosity
X-ray: fragmentation of tibial tuberosity
Treatment: activity modification, NSAIDs, stretching; resolves with skeletal maturity
The key to pediatric orthopedic questions is age + mechanism. A 6-year-old with hip pain = Legg-Calve-Perthes. A 14-year-old obese boy with hip pain = SCFE. A 13-year-old basketball player with knee pain = Osgood-Schlatter.
Sports Medicine: ACL Tears and Rotator Cuff Injuries
Sports medicine questions focus on knee and shoulder injuries, testing your knowledge of specific examination maneuvers and treatment decisions.
Knee Injuries
ACL Tear:
Mechanism: noncontact pivoting injury (basketball, soccer)
Clinical: "pop" heard at injury, immediate swelling, positive Lachman test (most sensitive), positive anterior drawer test
MRI: hyperintense signal in ACL, bone marrow edema
Treatment: surgical reconstruction for young athletes, conservative for older sedentary patients
Meniscus Tear:
Mechanism: twisting injury on planted foot
Clinical: mechanical symptoms (locking, catching), joint line tenderness, positive McMurray test
MRI: hyperintense signal extending to meniscal surface
Treatment: arthroscopic repair for peripheral tears, meniscectomy for central tears
Shoulder Injuries
Rotator Cuff Tear:
Demographics: >40 years, overhead athletes
Clinical: shoulder pain worse with overhead activity, weakness with abduction, positive "empty can" test
MRI: full-thickness vs partial-thickness tear
Treatment: physical therapy initially, surgical repair for young patients with acute tears
Shoulder Impingement:
Clinical: pain with overhead activity, positive Hawkins test, positive Neer sign
Treatment: NSAIDs, physical therapy, subacromial corticosteroid injection
Practice sports medicine cases with detailed explanations to master the examination maneuvers and treatment algorithms.
Clinical Vignette Strategy: Dissecting MSK Questions
MSK vignettes follow predictable patterns. Here's how to systematically approach them:
Step 1: Extract Demographics and Mechanism
Age (narrows differential significantly for bone tumors and pediatric conditions)
Sex (males more likely for Legg-Calve-Perthes and SCFE, females for osteoporosis fractures)
Mechanism (FOOSH = wrist fractures, twisting = ACL/meniscus, overhead activity = rotator cuff)
Step 2: Identify Key Clinical Findings
Location of pain (first MTP = gout, heel = plantar fasciitis, groin = hip pathology)
Quality of pain (mechanical = osteoarthritis, inflammatory = RA, radicular = disc herniation)
Associated symptoms (fever = infection, weight loss = malignancy, bowel/bladder = cauda equina)
Step 3: Interpret Imaging Descriptions
Since Step 2 CK can't show actual images, they describe findings in text:
"Sunburst pattern" = osteosarcoma
"Onion skin appearance" = Ewing sarcoma
"Joint space narrowing with osteophytes" = osteoarthritis
"Marginal erosions" = rheumatoid arthritis
Step 4: Analyze Laboratory Data
Synovial fluid WBC >100,000 = septic arthritis
Uric acid crystals = gout (but uric acid level may be normal during acute attack)
Elevated alkaline phosphatase in adolescent = consider osteosarcoma
Elevated ESR/CRP with joint pain = inflammatory arthritis or infection
Step 5: Choose Management Based on Urgency
Surgical emergencies: compartment syndrome, cauda equina, open fractures, septic arthritis
Urgent referrals: progressive neurologic deficits, suspected malignancy
Conservative management: most overuse injuries, stable fractures, degenerative conditions
Laboratory Interpretation in MSK Conditions
Understanding lab patterns helps differentiate similar conditions:
Inflammatory Markers
Normal ESR/CRP: Osteoarthritis, mechanical back pain, stable chronic conditions
Elevated ESR/CRP: Rheumatoid arthritis, septic arthritis, osteomyelitis, malignancy
Synovial Fluid Analysis
WBC <2,000: Osteoarthritis, trauma
WBC 2,000-50,000: Crystal arthropathy, inflammatory arthritis
WBC >100,000: Septic arthritis (85% neutrophils)
Bone-Specific Markers
Elevated Alkaline Phosphatase: Bone tumors (osteosarcoma), Paget disease, metastatic disease, growing adolescents
Normal Alkaline Phosphatase: Ewing sarcoma (helps differentiate from osteosarcoma)
Common Step 2 CK MSK Traps and How to Avoid Them
Trap 1: Gout During Acute Attack
Uric acid levels are normal in 30% of patients during acute gout attacks. Don't rule out gout based on normal uric acid — use synovial fluid analysis for definitive diagnosis.
Trap 2: Scaphoid Fracture with Normal X-Ray
Initial X-rays are negative in 15% of scaphoid fractures. If clinical suspicion is high (anatomical snuffbox tenderness after FOOSH), treat with thumb spica cast and repeat X-rays in 2 weeks.
Trap 3: Compartment Syndrome with Present Pulses
Pulselessness is a late finding in compartment syndrome. Don't wait for absent pulses — the key finding is pain with passive muscle stretch.
Trap 4: Septic Arthritis in Prosthetic Joints
Septic arthritis in prosthetic joints may present more subtly than native joint infections. Even low-grade fever with joint pain warrants immediate evaluation.
Trap 5: Vertebral Compression Fractures in Young Patients
Compression fractures in patients <50 should raise concern for malignancy, not osteoporosis. Order MRI and search for primary tumor.
Time Management for MSK Questions
MSK questions are longer than average Step 2 CK questions due to detailed mechanism descriptions and imaging findings. Use these strategies:
30-Second Rule for Fractures
If the vignette describes a fracture, identify:
1. Location (wrist, hip, spine)
2. Mechanism (FOOSH, fall, high-energy trauma)
3. Age (osteoporotic vs young adult vs pediatric)
This immediately narrows your differential to 2-3 options.
Pattern Recognition for Arthritis
For joint pain vignettes:
1. Acute vs chronic (septic arthritis vs degenerative)
2. Mono vs polyarticular (crystal vs inflammatory)
3. Symmetric vs asymmetric (RA vs osteoarthritis)
Emergency vs Elective Decision Tree
MSK questions often test urgency of treatment:
Emergent (next step: immediate surgery): Compartment syndrome, cauda equina, open fracture, septic arthritis
Urgent (next step: referral within 24-48 hours): Closed fractures, progressive neurologic deficits
Elective (next step: conservative treatment): Stable chronic conditions, overuse injuries
Use Oncourse's performance analytics to identify whether you're missing emergency cases (suggesting you need to memorize red flags) or overuse injuries (suggesting you need to review conservative management algorithms). This targeted feedback prevents broad, unfocused review sessions.
High-Yield MSK Mnemonics for Step 2 CK
Memory aids help consolidate the dense factual content in musculoskeletal medicine:
Bone Tumor Mnemonics
Age Groups: "CAGE" - Children (10-20): Ewing and Osteosarcoma; Adults (20-40): Giant cell and Chondrosarcoma; Golden years (>40): Metastatic disease Metastatic Sources: "BLT with a Kosher Pickle" - Breast, Lung, Thyroid, Kidney, Prostate
Compartment Syndrome (5 P's)
Pain, Pallor, Paresthesias, Paralysis, Pulselessness - but remember, pulselessness is late
Pediatric Hip Disorders by Age
"DDH at Diapers (0-6 months), LCP during License (4-8 years), SCFE during Sports (10-16 years)"
Crystal Arthropathy
Gout crystals: "Negatively birefringent Needle-shaped" (both start with N) Pseudogout crystals: "Positively birefringent Parallelogram-shaped" (both start with P)
Oncourse's mnemonic database surfaces these memory aids during your flashcard reviews, connecting abstract facts to memorable phrases. When you're reviewing bone tumors two weeks before your exam, seeing "BLT with a Kosher Pickle" instantly recalls the five most common primary sources of bone metastases.
Practice Question Patterns and Answer Strategies
Here are the most common Step 2 CK MSK question stems and how to approach them:
"Next Best Step" Questions
Trauma with obvious deformity: X-ray first (rule out fracture) Acute joint pain with fever: Arthrocentesis first (rule out septic arthritis) Back pain with neurologic symptoms: MRI first (rule out cord compression) Suspected compartment syndrome: Immediate fasciotomy (don't wait for pressure measurements)
"Most Likely Diagnosis" Questions
Use age as primary discriminator:
0-6 months with hip asymmetry: DDH
4-8 years with hip pain: Legg-Calve-Perthes
10-16 years obese with hip pain: SCFE
>65 with hip pain after fall: Hip fracture
>40 with bone lesion: Metastatic disease
"Best Initial Treatment" Questions
Conservative first: Overuse injuries, stable fractures, degenerative arthritis Surgical emergencies: Compartment syndrome, cauda equina, septic arthritis, open fractures Steroid injections: Trigger finger, carpal tunnel, subacromial impingement
MSK Question Bank Strategy
Effective question practice for MSK requires targeting specific weaknesses:
Week 1: Foundation Building
Focus on high-yield topics: fractures, arthritis differentials, bone tumors
Practice MSK questions with immediate review of explanations
Build spaced repetition cards for eponymous fractures and pediatric age cutoffs
Week 2: Pattern Recognition
Mixed MSK question sets to simulate exam conditions
Focus on emergency vs non-emergency decision making
Review imaging description interpretation
Week 3: Weakness Remediation
Use performance analytics to identify specific gaps
Target practice in weakest areas (emergency recognition vs chronic management)
Final review of high-yield mnemonics and age-based differentials
Review bone tumor classifications using spaced repetition to ensure age demographics and tumor characteristics stick for exam day.
Integration with Other Step 2 CK Systems
MSK pathology appears in non-orthopedic contexts on Step 2 CK:
Internal Medicine Integration
Rheumatoid arthritis: May present as constitutional symptoms before joint involvement
Gout: Associated with diabetes, hypertension, metabolic syndrome
Osteoporosis: Screen in postmenopausal women, initiate bisphosphonates
Emergency Medicine Integration
Compartment syndrome: Often presents with polytrauma
Septic arthritis: May present with sepsis, especially in immunocompromised
Cauda equina: Neurologic emergency requiring immediate recognition
Pediatrics Integration
Developmental milestones: When to refer for delayed walking
Growth plate injuries: Salter-Harris classifications and growth implications
Child abuse: Pattern of fractures suspicious for non-accidental trauma
Frequently Asked Questions
How many MSK questions can I expect on Step 2 CK?
Expect 8-12 MSK questions (roughly 3% of 280 total questions). They're distributed across internal medicine, surgery, emergency medicine, and pediatrics blocks, not grouped in a dedicated orthopedics section.
Should I memorize all fracture eponyms for Step 2 CK?
Focus on the highest-yield fractures with specific clinical implications: Colles, Smith, scaphoid, Jones, and Maisonneuve fractures. Skip rare eponyms that don't change management.
How detailed should my knowledge of surgical techniques be?
Step 2 CK tests decision-making (when to operate) not technical details (how to operate). Know indications for surgery, not specific surgical approaches.
What imaging findings are most important to recognize?
Focus on imaging descriptions rather than pattern recognition: "sunburst pattern" (osteosarcoma), "onion skin" (Ewing), "joint space narrowing with osteophytes" (osteoarthritis), "marginal erosions" (RA).
How do I differentiate pediatric hip disorders if age ranges overlap?
Use the peak age: DDH at birth, Legg-Calve-Perthes at age 6, SCFE at age 14. Also consider demographics: DDH in girls, LCP and SCFE in boys.
Should I focus more on traumatic or non-traumatic MSK conditions?
Both are equally important. Trauma questions test emergency recognition, while medical conditions test differential diagnosis skills. Balance your study time between both categories.
---
MSK medicine demands precision — the difference between compartment syndrome and muscle strain is immediate surgery vs rest. Between septic arthritis and gout is antibiotics vs anti-inflammatories. Master the demographics, recognize the emergencies, and differentiate the arthritis patterns.
The clinical vignettes test your systematic approach more than pure memorization. Age narrows bone tumor differentials. Mechanism predicts fracture patterns. Synovial fluid analysis distinguishes septic from crystal arthropathy. Lab values separate inflammatory from degenerative conditions.
Focus your remaining study time on emergency recognition, arthritis differentials, and pediatric age cutoffs. These three areas generate 70% of MSK points on Step 2 CK.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.