USMLE Step 2 CK Emergency Medicine: High-Yield Topics, Clinical Vignette Patterns and Exam Strategy (2026)
Master Emergency Medicine for USMLE Step 2 CK with high-yield topics, vignette patterns, and next-best-step strategies. Complete guide to EM clinical scenarios for 2026.
USMLE Step 2 CK Emergency Medicine: High-Yield Topics, Clinical Vignette Patterns and Exam Strategy (2026)
You are probably staring at your Step 2 CK prep schedule thinking: "Emergency Medicine — how much time do I really need for this?" The answer isnt what most students expect. EM accounts for roughly 8-12% of Step 2 CK questions, but these vignettes test the sharpest clinical reasoning skills on the entire exam. Unlike other subjects where you can reason through pathophysiology, EM questions reward instant pattern recognition and decisive action.
Here's what makes Step 2 CK Emergency Medicine different: you have 37 seconds to read a vignette about chest pain, recognize STEMI criteria, and choose between immediate catheterization versus more testing. The exam doesnt want your differential diagnosis — it wants your next move. This isnt about knowing everything; it's about recognizing the patterns that matter and acting fast.
The students who nail EM vignettes understand something crucial: Step 2 CK Emergency Medicine tests clinical intuition under pressure. When Clinical Rounds walks you through rapid-fire emergency scenarios — unstable patient, limited info, one right move — you build exactly this reflexive pattern recognition that EM vignettes reward.
Understanding Step 2 CK Emergency Medicine Vignette Structure
Step 2 CK EM questions follow predictable patterns that mirror real emergency department decision-making. Unlike shelf exams that test comprehensive knowledge, these vignettes present time-critical scenarios where the "next best step" logic dominates everything else.
The Three-Layer Vignette Pattern
Layer 1: Clinical Presentation — Patient presents with chief complaint (chest pain, shortness of breath, altered mental status). This layer contains the diagnostic clues but often includes red herrings. Layer 2: Critical Findings — Vital signs, physical exam findings, or initial test results that point toward time-sensitive conditions. This is where pattern recognition becomes crucial. Layer 3: Decision Point — The question stem asks for immediate management, next diagnostic step, or most likely diagnosis. The correct answer reflects emergency medicine priorities: airway, breathing, circulation, then definitive treatment.
High-Yield Vignette Templates
Emergency Medicine vignettes on Step 2 CK cluster around these clinical scenarios:
Undifferentiated shock — Hemodynamic instability requiring rapid classification and intervention
Chest pain with ECG changes — Acute coronary syndrome recognition and time-critical management
Acute respiratory distress — Differentiation between cardiogenic vs non-cardiogenic causes
Altered mental status — Metabolic vs structural vs toxicological causes requiring immediate intervention
Trauma with unstable vitals — ATLS protocol application under time pressure
Septic patient — Early recognition and protocol initiation
STEMI and Acute Coronary Syndrome Management
STEMI recognition and management represents one of the highest-yield topics for Step 2 CK Emergency Medicine vignettes. The key insight: these questions test time-critical decision making, not ECG interpretation skills.
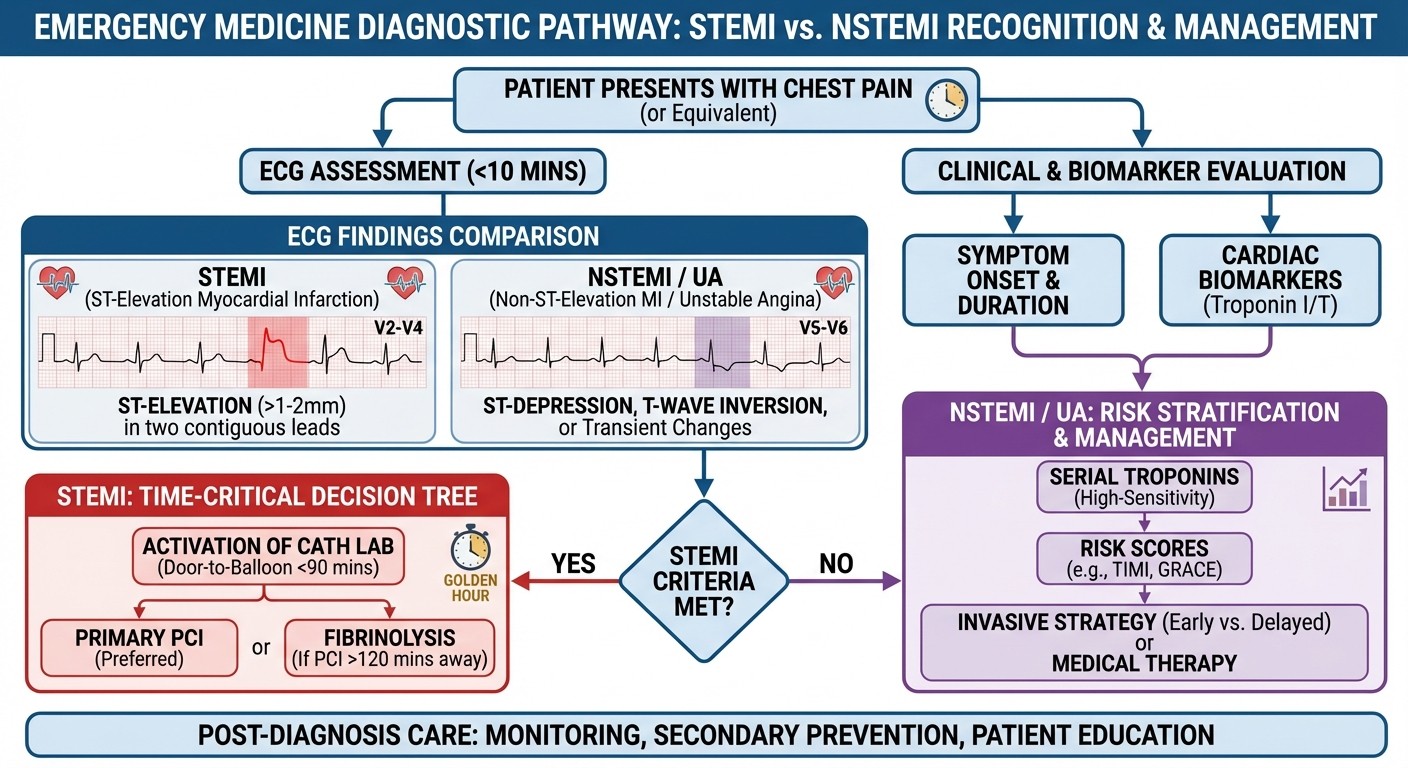
STEMI vs NSTEMI Recognition Patterns
STEMI Criteria (Step 2 CK Focus):
ST elevation ≥1mm in 2 contiguous leads (except V2-V3: ≥2mm in men, ≥1.5mm in women)
New LBBB (consider STEMI equivalent)
Posterior STEMI (tall R waves in V1-V2 with ST depression)
NSTEMI/Unstable Angina Patterns:
ST depression or T-wave inversion
Dynamic ECG changes with symptoms
Elevated troponin without ST elevation
The vignette pattern: 55-year-old patient with crushing chest pain, diaphoresis, and specific ECG findings. The question tests whether you recognize the time-sensitive nature and choose immediate intervention over additional testing.
Reperfusion Strategy Decision Points
For STEMI patients, Step 2 CK vignettes focus on these decision trees:
Primary PCI vs Thrombolysis:
If PCI available within 90 minutes → Primary PCI
If PCI not available or delay >90 minutes → Thrombolytic therapy
Contraindications to thrombolytics: recent surgery, active bleeding, previous hemorrhagic stroke
Antiplatelet/Anticoagulation Sequence:
1. Aspirin 325mg (immediate, unless contraindicated)
2. Clopidogrel loading dose
3. Anticoagulation (unfractionated heparin or enoxaparin)
4. Consider GP IIb/IIIa inhibitors for high-risk patients
Step 2 CK Exam Strategy for ACS Vignettes
The exam rewards aggressive, time-appropriate management. When you see chest pain with STEMI criteria, the answer is never "obtain echocardiogram first" or "check serial troponins." The correct choice reflects emergency medicine thinking: recognize the pattern, act immediately.
Common distractors include reasonable but time-inappropriate choices like stress testing, cardiac catheterization scheduling, or additional biomarker testing. Remember: STEMI is a catheter emergency, not a lab emergency.
Sepsis Recognition and Early Management Protocols
Sepsis vignettes on Step 2 CK test your ability to recognize systemic inflammatory response and initiate early goal-directed therapy. The critical insight: these questions reward protocol-based thinking over diagnostic uncertainty.
SIRS vs Sepsis vs Septic Shock Differentiation
SIRS Criteria (≥2 required):
Temperature >38°C or <36°C
Heart rate >90 bpm
Respiratory rate >20 or PaCO2 <32 mmHg
WBC >12,000, <4,000, or >10% bands
Sepsis = SIRS + suspected infection Severe Sepsis = Sepsis + organ dysfunction Septic Shock = Severe sepsis + hypotension despite fluid resuscitation
Step 2 CK vignettes typically present patients with fever, altered mental status, hypotension, and laboratory abnormalities suggesting organ dysfunction. The question tests whether you recognize the syndrome and choose appropriate initial management.
Early Goal-Directed Therapy Sequence
The exam expects this management approach for septic patients:
First Hour Bundle:
1. Blood cultures before antibiotics (if no delay)
2. Broad-spectrum antibiotics within 1 hour
3. Fluid resuscitation with crystalloids
4. Vasopressors if hypotension persists
Antibiotic vs Culture Timing:
If stable enough for cultures → obtain cultures first
If hemodynamically unstable → start antibiotics immediately
Never delay antibiotics >1 hour for cultures
When analyzing sepsis vignettes, Explanation Chat becomes invaluable for understanding why early intervention beats additional testing — it explains the clinical reasoning chain of why waiting costs the patient, exactly the logic gap most students have in EM scenarios.
Sepsis Vignette Red Flags
Watch for these presentation patterns that signal septic shock:
Elderly patient with altered mental status and mild fever
Diabetic with foot infection and confusion
Post-operative patient with fever and hypotension
Immunocompromised host with any infection signs
The key concept: sepsis can present subtly in high-risk populations. Step 2 CK rewards early recognition and aggressive management over watchful waiting.
Trauma Assessment and ATLS Principles
Trauma vignettes test ATLS protocol application under time pressure. These questions reward systematic thinking: primary survey identifies life threats, secondary survey finds everything else.
Primary Survey Priorities (ABCDE)
A - Airway with C-spine control
Assess airway patency while maintaining cervical spine immobilization
Signs of compromise: stridor, voice changes, facial trauma
Management: jaw thrust, oropharyngeal airway, or immediate intubation
B - Breathing and ventilation
Look for tension pneumothorax, open pneumothorax, massive hemothorax
Tension pneumothorax signs: tracheal deviation, JVD, absent breath sounds, hypotension
Management: immediate needle decompression → chest tube
C - Circulation and hemorrhage control
Identify source of blood loss and control
Signs of shock: hypotension, tachycardia, altered mental status
Management: IV access, fluid resuscitation, blood products
D - Disability (neurologic)
Glasgow Coma Scale assessment
Pupil evaluation for increased intracranial pressure
E - Exposure and environmental control
Complete undressing for full assessment
Prevent hypothermia
Tension Pneumothorax vs Hemothorax Differentiation
This distinction appears frequently on Step 2 CK:
Tension Pneumothorax:
Tracheal deviation away from affected side
JVD (increased venous pressure)
Hyperresonant to percussion
Absent breath sounds
Immediate treatment: needle decompression
Massive Hemothorax:
Tracheal deviation toward affected side
Flat neck veins (decreased venous return)
Dull to percussion
Absent breath sounds
Immediate treatment: chest tube placement
When to Go Directly to OR
Step 2 CK trauma vignettes test this decision point frequently. Immediate surgical intervention is indicated for:
Penetrating abdominal trauma with peritoneal signs
Hemodynamic instability despite resuscitation
Obvious internal bleeding source
Expanding abdominal hematoma
The exam rewards decisive action for unstable patients. If the vignette describes shock with obvious bleeding, the answer is operating room, not additional imaging.
Acute Respiratory Failure Recognition and Management
Respiratory failure vignettes test your ability to differentiate causes and choose appropriate ventilatory support. The key concept: match the intervention to the underlying pathophysiology.
ARDS Criteria and Berlin Definition
Timing: Within 1 week of clinical insult Chest imaging: Bilateral opacities not explained by effusions or collapse Origin of edema: Not fully explained by cardiac failure Oxygenation (PaO2/FiO2 ratio):
Mild: 200-300 mmHg
Moderate: 100-200 mmHg
Severe: <100 mmHg
ARDS vignettes typically present patients with bilateral infiltrates, severe hypoxemia, and identifiable risk factors (sepsis, aspiration, massive transfusion). The management focuses on lung-protective ventilation strategies.
Non-invasive vs Invasive Ventilation Decision
NIV Appropriate for:
COPD exacerbation with respiratory acidosis
Cardiogenic pulmonary edema
Immunocompromised patients (avoid intubation if possible)
Immediate Intubation Required for:
Respiratory arrest or apnea
Severe hypoxemia despite high-flow oxygen
Inability to protect airway (GCS <8)
Hemodynamic instability with respiratory distress
The exam tests this decision point with hemodynamically unstable patients. When respiratory failure accompanies shock, the answer is usually mechanical ventilation, not trial of NIV.
Pulmonary Embolism Presenting as Respiratory Failure
PE vignettes focus on high-risk presentations:
Massive PE with RV strain and hypotension
Submassive PE with RV dysfunction but stable BP
High-risk patients (surgery, malignancy, prolonged immobilization)
High-Risk PE Management:
Immediate anticoagulation if no contraindications
Thrombolytic therapy for hemodynamic instability
Embolectomy for massive PE with contraindications to lysis
The key insight: PE can present as undifferentiated respiratory failure. Look for risk factors and consider early CT angiography in appropriate clinical context.
Stroke Recognition and Time-Critical Management
Stroke vignettes test rapid differentiation between hemorrhagic and ischemic stroke, plus time-appropriate interventions. The central concept: "time is brain" — interventions become less effective as minutes pass.
Hemorrhagic vs Ischemic Stroke Differentiation
Clinical Clues Favoring Hemorrhage:
Sudden onset severe headache ("worst headache of life")
Vomiting at onset
Early loss of consciousness
Rapid deterioration
Clinical Clues Favoring Ischemic:
Gradual onset or stuttering progression
Specific vascular territory deficits
History of atrial fibrillation or carotid disease
Critical Decision Point: CT scan without contrast is the first test for any acute stroke presentation. This differentiates hemorrhage from ischemia and determines treatment pathway.
tPA Eligibility and Time Windows
Inclusion Criteria:
Acute ischemic stroke with disabling deficit
Onset <3 hours (extended to 4.5 hours in select patients)
Age >18 years
Major Contraindications:
Recent stroke, surgery, or head trauma
Active bleeding or bleeding diathesis
Platelet count <100,000
INR >1.7
The vignette pattern: patient with acute focal neurologic deficits, clear time of onset, and CT showing no hemorrhage. The question tests whether you recognize tPA candidacy and choose immediate treatment over additional testing.
Blood Pressure Management in Stroke
Ischemic Stroke:
No BP lowering unless >220/120 mmHg
If tPA candidate: target <185/110 before treatment
Gentle BP reduction to avoid hypoperfusion
Hemorrhagic Stroke:
More aggressive BP control
Target systolic 140-180 mmHg
Avoid excessive reduction (increases ischemia risk)
For Step 2 CK purposes, remember that stroke patients need permissive hypertension unless receiving thrombolytics or having intracerebral hemorrhage.
Shock Types and Hemodynamic Differentiation
Shock recognition represents core emergency medicine knowledge for Step 2 CK. These vignettes test your ability to classify shock type based on hemodynamic profile and choose appropriate initial management.
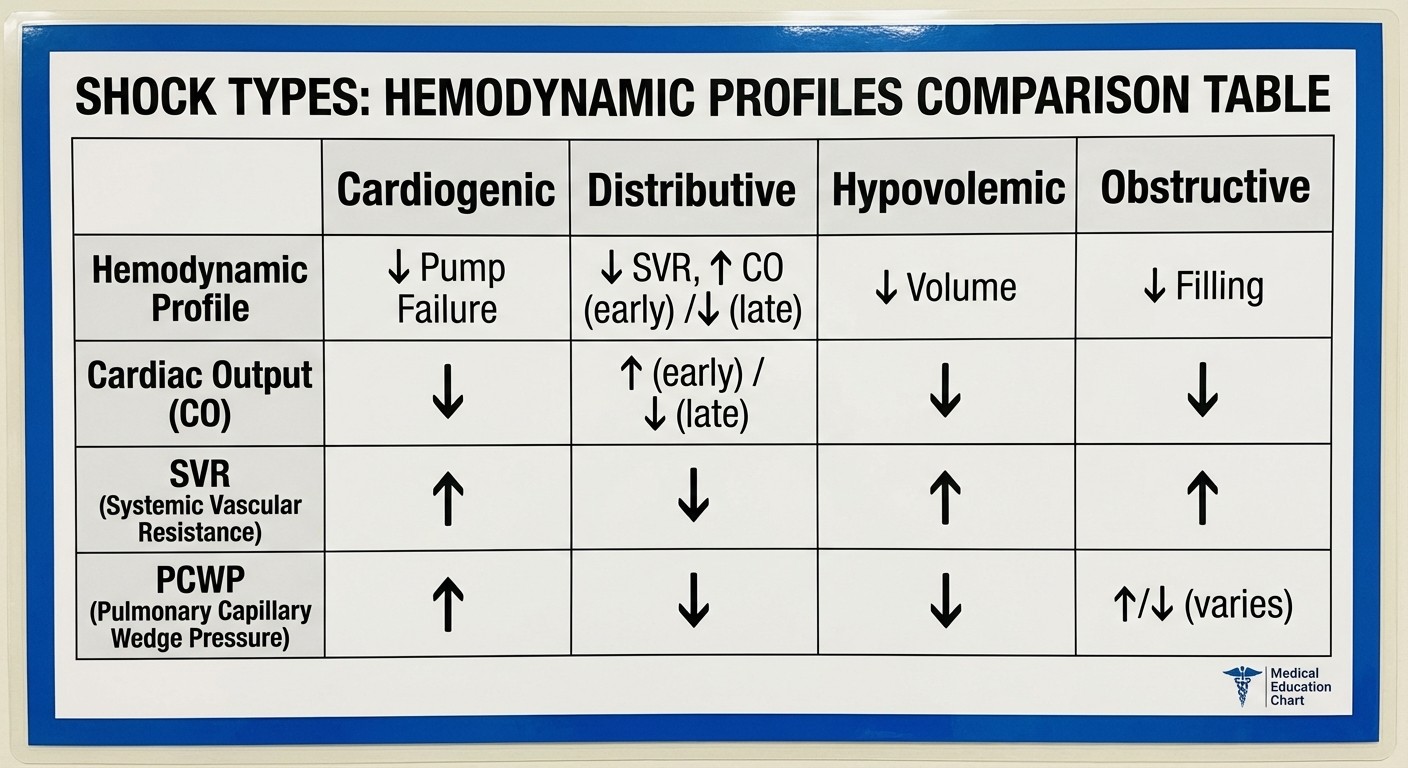
Hemodynamic Profiles by Shock Type
Shock Type | Cardiac Output | SVR | PCWP | Examples |
|---|---|---|---|---|
Cardiogenic | ↓ | ↑ | ↑ | MI, cardiomyopathy |
Hypovolemic | ↓ | ↑ | ↓ | Bleeding, dehydration |
Distributive | ↑ | ↓ | ↓ | Sepsis, anaphylaxis |
Obstructive | ↓ | ↑ | Variable | PE, tamponade |
The pattern recognition here becomes crucial under exam time pressure. For toxicology and shock differentials that require pure memorization, Oncourse AI's Mnemonic engine generates custom recall chains for complex lists like these hemodynamic profiles, giving you a retrieval handle under exam pressure.
Cardiogenic Shock Recognition
Presentation: Hypotension, elevated JVD, pulmonary edema, cool extremities Hemodynamics: Low cardiac output, high SVR (compensatory vasoconstriction), high PCWP Management: Optimize preload, consider inotropes, emergent revascularization for ACS
Distributive Shock (Sepsis/Anaphylaxis)
Presentation: Hypotension with warm extremities, altered mental status Hemodynamics: High cardiac output (early), low SVR, low PCWP Management: Fluid resuscitation, vasopressors, treat underlying cause
Hypovolemic Shock
Presentation: Hypotension, tachycardia, poor skin turgor, flat neck veins Hemodynamics: Low cardiac output, high SVR, low PCWP Management: Identify bleeding source, IV access, fluid/blood resuscitation
Obstructive Shock
Cardiac Tamponade:
Beck's triad: hypotension, JVD, muffled heart sounds
Pulsus paradoxus >10 mmHg
Management: pericardiocentesis
Massive PE:
Right heart strain on ECG
Elevated JVD with clear lungs
Management: anticoagulation, consider thrombolytics
Toxicology and Antidote Recognition
Toxicology vignettes test pattern recognition for classic toxidromes and appropriate antidote selection. These questions reward memorization paired with clinical reasoning.
Classic Toxidrome Patterns
Opioid Toxidrome:
Miotic pupils, respiratory depression, altered mental status
Antidote: Naloxone 0.4-2mg IV/IM
Consider fentanyl (requires higher doses, repeated dosing)
Anticholinergic Toxidrome:
"Mad as a hatter, red as a beet, hot as a hare, dry as a bone, blind as a bat"
Dilated pupils, hyperthermia, dry skin, delirium, urinary retention
Antidote: Physostigmine (only for pure anticholinergic, not tricyclics)
Cholinergic Toxidrome (Organophosphates):
SLUDGE syndrome: Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis
Miotic pupils, muscle fasciculations, respiratory failure
Antidote: Atropine + Pralidoxime
Sympathomimetic Toxidrome:
Hyperthermia, hypertension, tachycardia, diaphoresis, agitation
Dilated pupils, hyperreflexia
Management: Benzodiazepines, avoid beta-blockers
Serotonin Syndrome vs Neuroleptic Malignant Syndrome
This differentiation appears frequently on Step 2 CK:
Serotonin Syndrome:
Rapid onset (hours)
Hyperreflexia, clonus, mydriasis
Recent addition of serotonergic agent
Treatment: Cyproheptadine, supportive care
Neuroleptic Malignant Syndrome:
Gradual onset (days to weeks)
Lead-pipe rigidity, hyporeflexia
Recent antipsychotic use
Treatment: Dantrolene, bromocriptine
High-Yield Antidote Associations
Acetaminophen: N-acetylcysteine
Organophosphates: Atropine + Pralidoxime
Opioids: Naloxone
Benzodiazepines: Flumazenil (caution: seizure risk)
Digoxin: Digoxin-specific antibodies
Iron: Deferoxamine
Lead: EDTA or Succimer
Methanol/Ethylene glycol: Fomepizole or ethanol
Pediatric Emergency Medicine Essentials
Pediatric EM vignettes focus on age-specific presentations and management differences. The key insight: children compensate well until they crash suddenly.
Epiglottitis vs Croup Differentiation
Epiglottitis (Haemophilus influenzae):
Acute onset, toxic appearance
High fever, drooling, difficulty swallowing
Muffled voice, sitting upright
Management: Secure airway in OR, avoid examination
Croup (Viral laryngotracheobronchitis):
Gradual onset, viral prodrome
Barking cough, inspiratory stridor
Low-grade fever, less toxic appearance
Management: Dexamethasone, racemic epinephrine for severe cases
Intussusception vs Volvulus
Intussusception:
Age 6 months - 2 years
Intermittent cramping pain with periods of normalcy
Currant jelly stools, RUQ mass
Management: Air/contrast enema (diagnostic and therapeutic)
Midgut Volvulus:
Age <1 year (usually <1 month)
Sudden onset bilious vomiting
Shock and abdominal distension
Management: Emergent surgical detorsion
Febrile Seizures
Simple Febrile Seizures:
Age 6 months - 5 years
Generalized, <15 minutes
No focal features or recurrence
Management: Supportive care, antipyretics
Complex Febrile Seizures:
Focal features, >15 minutes, or recurrence
Requires neurologic evaluation and LP consideration
Step 2 CK Emergency Medicine Exam Strategy
Success on Step 2 CK EM vignettes requires specific test-taking strategies that mirror emergency medicine thinking patterns.
Time Management for EM Vignettes
The 37-Second Rule: Each EM vignette should take 30-45 seconds maximum. These questions reward rapid pattern recognition, not detailed analysis. Triage Reading Strategy:
1. Read the last sentence first (what's being asked)
2. Identify the chief complaint and vital signs
3. Look for time-critical findings
4. Choose the most immediate intervention
Pattern Recognition vs Differential Diagnosis
Emergency medicine vignettes don't want your differential diagnosis — they want your next action. The correct answer reflects emergency priorities:
1. Airway/Breathing threats — Always addressed first
2. Circulation issues — Shock, bleeding, arrhythmias
3. Disability concerns — Neurologic emergencies
4. Definitive treatment — After stabilization
Common Distractors in EM Vignettes
"More Information" Distractors:
Additional history taking
Serial laboratory monitoring
Echocardiogram for obvious STEMI
CT scan for hemodynamically unstable trauma
"Reasonable but Premature" Distractors:
Subspecialty consultation before stabilization
Definitive procedures before resuscitation
Discharge planning for unstable patients
Next Best Step Logic
The "next best step" in emergency medicine follows predictable patterns:
For Unstable Patients: Stabilize before testing For Obvious Diagnoses: Treat immediately, don't confirm For Time-Critical Conditions: Act within therapeutic windows For Multiple Problems: Address the most life-threatening first
High-Yield Study Strategies for Step 2 CK EM
Focus on Decision Points, Not Pathophysiology
Unlike other Step 2 CK topics where pathophysiology helps reason through answers, Emergency Medicine rewards memorized decision trees and rapid pattern recognition.
Study Method 1: Algorithm Memorization
ACLS protocols for cardiac arrest
ATLS sequence for trauma
Sepsis bundles for infection
Stroke protocols for neurologic emergencies
Study Method 2: Vignette Pattern Training Practice rapid case recognition with tools like Clinical Rounds that put you through rapid-fire scenarios — this builds the reflexive pattern recognition that EM vignettes reward on test day.
Time-Critical Condition Flashcards
Create flashcards for conditions where timing determines outcome:
STEMI reperfusion windows
Stroke thrombolytic eligibility
Sepsis antibiotic timing
Trauma golden hour interventions
Use spaced repetition flashcards to drill these time-critical decision points until they become automatic.
Practice Under Time Pressure
Emergency Medicine questions should feel urgent. Set a 30-second timer for each practice vignette. If you cant identify the pattern and choose an answer within 45 seconds, you need more pattern recognition practice.
Antidote and Protocol Memorization
Toxicology and emergency protocols require pure memorization. Use active recall techniques:
Write out toxidrome features from memory
Practice antidote associations without looking
Quiz yourself on shock hemodynamic patterns
For complex lists like toxidromes or shock types, memory devices help you recall under pressure — exactly what spaced repetition tools like flashcard systems provide for instant recall that timed Step 2 CK blocks demand.
Frequently Asked Questions
How much time should I spend studying Emergency Medicine for Step 2 CK?
Emergency Medicine should account for 8-12% of your study time, roughly 1-2 weeks in a 3-month prep schedule. Focus on high-yield topics like ACS, sepsis, stroke, and shock rather than trying to cover everything comprehensively.
Are Emergency Medicine questions harder on Step 2 CK compared to shelf exams?
Step 2 CK EM questions test clinical decision-making under time pressure rather than comprehensive knowledge. They're not necessarily harder, but they require faster pattern recognition and more decisive thinking than typical shelf exam questions.
Should I memorize all the antidotes and toxidromes?
Yes — toxicology is pure memorization and appears frequently on Step 2 CK. Focus on the classic toxidromes (opioid, anticholinergic, cholinergic, sympathomimetic) and their specific antidotes. Use spaced repetition to make these automatic.
How do I improve my speed on Emergency Medicine vignettes?
Practice rapid pattern recognition with timed questions. Set a 30-45 second limit per vignette and focus on identifying the key clinical pattern rather than analyzing every detail. Emergency Medicine rewards decisive thinking over exhaustive analysis.
What's the best way to remember shock types and their hemodynamic profiles?
Create a comparison table and use spaced repetition flashcards. The key is memorizing the patterns: cardiogenic (low CO, high SVR, high PCWP), distributive (high CO, low SVR, low PCWP), hypovolemic (low CO, high SVR, low PCWP), obstructive (variable patterns depending on cause).
Do I need to know pediatric Emergency Medicine for Step 2 CK?
Yes, but focus on high-yield topics like febrile seizures, croup vs epiglottitis, and common pediatric emergencies. Pediatric EM represents a smaller portion than adult EM, but the concepts appear regularly on the exam.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.