Back
Pituitary Disorders: Complete High-Yield Guide for NEET PG and USMLE Step 1 (2026)
Master pituitary disorders for NEET PG and USMLE Step 1 with this comprehensive guide covering anterior/posterior hormones, acromegaly, Cushing disease, prolactinoma, and diabetes insipidus vs SIADH.

Pituitary Disorders: Complete High-Yield Guide for NEET PG and USMLE Step 1 (2026)
You are staring at a 25-year-old woman with galactorrhea, amenorrhea, and bitemporal hemianopia. The prolactin level comes back at 180 ng/mL. Your brain immediately jumps to prolactinoma — but wait, is this a microprolactinoma or macroprolactinoma? Does the degree of prolactin elevation matter? And why does she have visual field defects?
Pituitary disorders are the ultimate systems-based challenge in NEET PG and USMLE Step 1. Unlike other endocrine topics where you memorize isolated facts, pituitary pathology demands you understand how each hormone fits into feedback loops, how tumors disrupt normal anatomy, and why specific lab patterns are pathognomonic.
This guide breaks down every high-yield pituitary disorder into clinically actionable knowledge. We'll cover the hypothalamic-pituitary axis systematically, dive into anterior vs posterior pathology, and tackle the classic clinical vignettes that appear in 15% of endocrinology questions on both exams.
By the end, you'll recognize acromegaly from a single photo, distinguish Cushing disease from Cushing syndrome using lab patterns, and confidently work through diabetes insipidus vs SIADH scenarios.
Pituitary Anatomy and Physiology: Foundation Concepts
The pituitary sits in the sella turcica, connected to the hypothalamus via the infundibulum. Understanding this anatomical relationship explains why large pituitary tumors cause visual field defects (optic chiasm compression) and why posterior pituitary function can be preserved in anterior pituitary destruction.
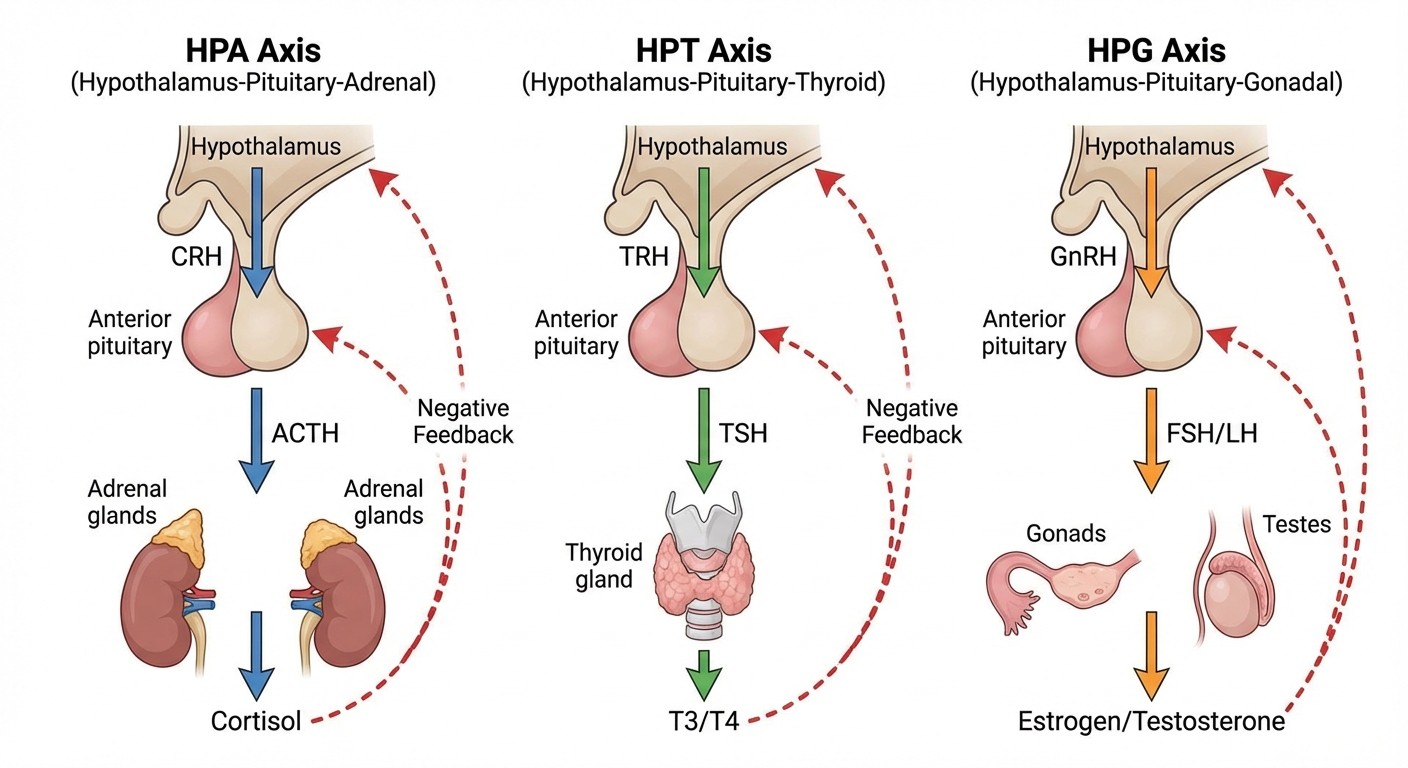
Anterior Pituitary Hormones: The Big Six
The anterior pituitary (adenohypophysis) synthesizes six hormones under hypothalamic control. Each has a specific releasing hormone, target organ, and feedback mechanism:
Hormone | Releasing Factor | Target Organ | Primary Function |
|---|---|---|---|
Growth Hormone (GH) | GHRH | Liver → IGF-1 | Growth, metabolism |
TSH | TRH | Thyroid | T3/T4 synthesis |
ACTH | CRH | Adrenal cortex | Cortisol synthesis |
FSH | GnRH | Gonads | Folliculogenesis, spermatogenesis |
LH | GnRH | Gonads | Ovulation, testosterone synthesis |
Prolactin | - | Breast tissue | Milk production |
High-yield concept: Prolactin is unique — it's under tonic inhibition by dopamine. This explains why dopamine agonists (cabergoline, bromocriptine) treat prolactinomas, and why antipsychotics cause hyperprolactinemia.
Posterior Pituitary Hormones
The posterior pituitary (neurohypophysis) stores and releases two hypothalamic hormones:
ADH (Vasopressin): Water reabsorption in collecting ducts
Oxytocin: Uterine contractions, milk ejection reflex
Clinical pearl: Posterior pituitary hormones are made in hypothalamic nuclei and transported down axons. This is why hypothalamic lesions can cause diabetes insipidus even with intact posterior pituitary tissue.
Anterior Pituitary Disorders: Excess vs Deficiency
Growth Hormone Disorders
#### Acromegaly (GH Excess)
Classic presentation: A 40-year-old man notices his wedding ring doesnt fit anymore. His wife says his facial features have changed over 5 years. He has headaches, joint pain, and enlarging hands and feet. Pathophysiology: Usually caused by a GH-secreting pituitary adenoma (somatotropinoma). Excess GH stimulates IGF-1 production, causing tissue overgrowth. Clinical features:
Skeletal: Enlarged hands, feet, jaw (prognathism)
Soft tissue: Macroglossia, carpal tunnel syndrome
Metabolic: Diabetes mellitus, hypertension
Cardiac: Cardiomyopathy, arrhythmias
Mass effects: Headache, visual field defects
Laboratory findings:
IGF-1: Elevated (best screening test)
Glucose suppression test: GH fails to suppress <1 ng/mL after 75g glucose
MRI: Pituitary adenoma (usually macroadenoma >10mm)
Treatment: 1. Surgery: Trans-sphenoidal resection (first-line) 2. Medical: Octreotide (somatostatin analog), cabergoline (if mixed GH/prolactin tumor) 3. Radiation: For surgical failures NEET PG high-yield: Acromegaly increases colon cancer risk — colonoscopy screening is mandatory.
#### GH Deficiency
Adults: Fatigue, decreased muscle mass, increased fat, poor quality of life Children: Short stature, delayed puberty Diagnosis: Stimulation tests (insulin tolerance test, arginine stimulation) Treatment: Recombinant GH replacement
Prolactin Disorders
#### Prolactinoma
Most common pituitary tumor. Classified by size:
Microprolactinoma: <10mm
Macroprolactinoma: ≥10mm
Clinical presentation by gender: Women:
Galactorrhea (inappropriate milk production)
Amenorrhea or oligomenorrhea
Infertility
Osteoporosis (from estrogen deficiency)
Men:
Erectile dysfunction
Decreased libido
Gynecomastia (less common)
Mass effects (more common — men present later)
Laboratory approach:
Prolactin >200 ng/mL: Almost always prolactinoma
Prolactin 20-200 ng/mL: Could be prolactinoma or other causes
Rule out: Pregnancy, medications (antipsychotics, metoclopramide), hypothyroidism
Treatment: 1. First-line: Cabergoline (dopamine agonist) — shrinks tumor and normalizes prolactin 2. Alternative: Bromocriptine (more side effects) 3. Surgery: For drug-resistant cases or CSF leak risk High-yield drug facts:
Cabergoline: 2x/week dosing, better tolerated than bromocriptine
Monitor for cardiac valve abnormalities with high doses
ACTH Disorders
#### Cushing Disease (ACTH Excess from Pituitary)
Distinguish from Cushing syndrome: Cushing disease is specifically pituitary-driven ACTH excess. Cushing syndrome includes all causes of cortisol excess. Clinical features:
Central obesity: Moon facies, buffalo hump, abdominal striae
Skin: Purple striae, easy bruising, poor wound healing
Metabolic: Diabetes, hypertension, osteoporosis
Psychiatric: Depression, psychosis
Proximal muscle weakness
Laboratory workup (the dexamethasone dance):
Test | Cushing Disease Result | Other Causes |
|---|---|---|
24h urine cortisol | Elevated | Elevated |
Low-dose dex suppression | No suppression | No suppression |
High-dose dex suppression | Suppression | No suppression |
ACTH level | Elevated | Low (adrenal) or Very high (ectopic) |
Key concept: High-dose dexamethasone suppresses pituitary ACTH but not ectopic ACTH sources. Treatment: 1. Surgery: Trans-sphenoidal resection 2. Medical: Ketoconazole, metyrapone (cortisol synthesis inhibitors) 3. Bilateral adrenalectomy: Last resort (causes Nelson syndrome)
#### ACTH Deficiency (Secondary Adrenal Insufficiency)
Presentation: Fatigue, weakness, weight loss, hypoglycemia Key difference from primary: No hyperpigmentation, no hyperkalemia (aldosterone preserved) Treatment: Hydrocortisone replacement
Gonadotropin Disorders (FSH/LH)
#### Hypogonadotropic Hypogonadism
Men: Low testosterone with low/normal FSH/LH Women: Amenorrhea, infertility, estrogen deficiency Causes:
Pituitary tumors compressing normal tissue
Kallmann syndrome (congenital GnRH deficiency with anosmia)
Hyperprolactinemia (inhibits GnRH)
Treatment:
Men: Testosterone replacement or HCG if fertility desired
Women: Estrogen replacement or ovulation induction
TSH Disorders
#### Central Hypothyroidism (TSH Deficiency)
Laboratory pattern: Low T4 with low or inappropriately normal TSH Clinical features: Same as primary hypothyroidism but often milder Treatment: Levothyroxine replacement (dose guided by free T4, not TSH) Critical point: Always treat adrenal insufficiency before thyroid replacement to avoid precipitating adrenal crisis.
Panhypopituitarism: When Everything Fails
Sheehan Syndrome
Classic scenario: A woman develops fatigue, inability to breastfeed, and amenorrhea after a complicated delivery with significant postpartum hemorrhage. Pathophysiology: Postpartum pituitary necrosis due to:
1. Pregnancy enlarges pituitary (estrogen effect)
2. Postpartum hemorrhage → hypotension
3. Enlarged gland more vulnerable to ischemia
Clinical presentation (depends on which hormones are lost first): 1. Prolactin deficiency: Inability to breastfeed (earliest sign) 2. GH deficiency: Fatigue, weakness 3. FSH/LH deficiency: Amenorrhea, infertility 4. ACTH deficiency: Adrenal insufficiency 5. TSH deficiency: Hypothyroidism Diagnosis:
Low levels of multiple pituitary hormones
MRI: Empty or partially empty sella turcica
History of postpartum hemorrhage
Treatment: Hormone replacement in order of urgency: 1. Hydrocortisone (most critical) 2. Levothyroxine 3. Estrogen/testosterone 4. Growth hormone (if indicated)
Other Causes of Panhypopituitarism
Pituitary apoplexy: Sudden hemorrhage/infarction
Craniopharyngioma: Especially in children
Radiation damage
Infiltrative diseases: Sarcoidosis, hemochromatosis
Posterior Pituitary Disorders
Diabetes Insipidus vs SIADH: The Water Wars
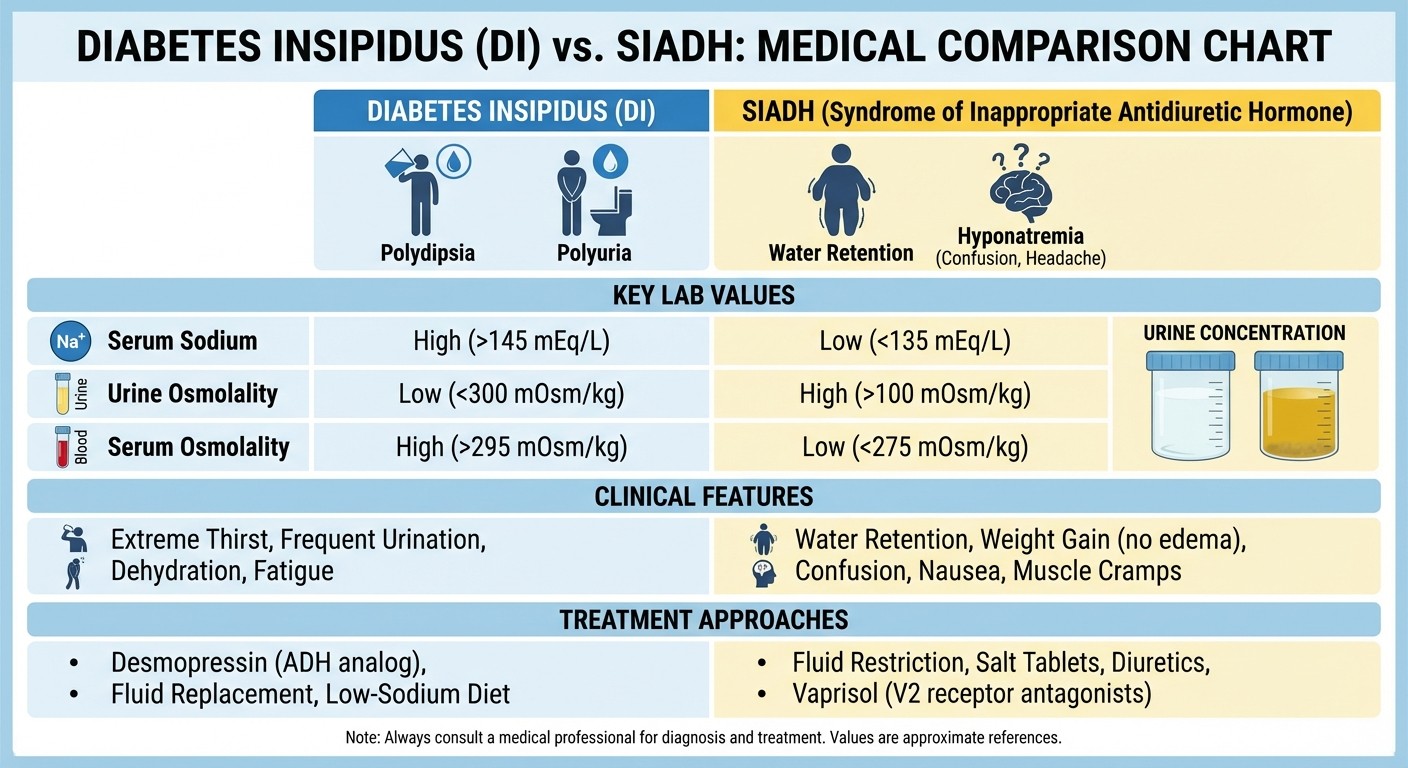
Diabetes Insipidus (DI)
Clinical presentation: Polyuria (>3L/day), polydipsia, nocturia, dehydration if water intake cant match losses. Types: 1. Central DI: ADH deficiency (pituitary/hypothalamic damage) 2. Nephrogenic DI: Kidney resistance to ADH Laboratory findings:
Serum osmolality: >295 mOsm/kg (concentrated blood)
Urine osmolality: <300 mOsm/kg (dilute urine)
Serum sodium: Often elevated (hypernatremia)
Water deprivation test (the definitive test): 1. Normal response: Urine concentrates (>600 mOsm/kg) 2. Central DI: Urine stays dilute, improves with desmopressin 3. Nephrogenic DI: Urine stays dilute despite desmopressin Treatment:
Central DI: Desmopressin (synthetic ADH)
Nephrogenic DI: Thiazide diuretics, amiloride
SIADH (Syndrome of Inappropriate ADH Secretion)
Clinical presentation: Often asymptomatic until severe hyponatremia. When symptomatic: confusion, seizures, coma. Laboratory findings:
Serum osmolality: <280 mOsm/kg (dilute blood)
Urine osmolality: >100 mOsm/kg (inappropriately concentrated)
Serum sodium: <135 mEq/L (hyponatremia)
Urine sodium: >20 mEq/L (euvolemic)
Common causes:
Malignancy: Lung cancer (especially small cell)
CNS disorders: Stroke, trauma, infections
Drugs: SSRIs, carbamazepine, cyclophosphamide
Pulmonary: Pneumonia, ARDS
Treatment (depends on severity):
Mild/chronic: Water restriction
Severe/acute: Hypertonic saline (careful correction rate)
Chronic management: Tolvaptan (ADH receptor antagonist)
Critical concept: Correct hyponatremia slowly (8-12 mEq/L per day max) to avoid central pontine myelinolysis.
Pituitary Tumors: Functional vs Non-Functional
Functional Adenomas (Hormone-Secreting)
Classification by hormone: 1. Prolactinoma (40%): Most common functional adenoma 2. Somatotropinoma (20%): GH-secreting → acromegaly 3. Corticotropinoma (15%): ACTH-secreting → Cushing disease 4. Mixed adenomas: Often GH + prolactin
Non-Functional Adenomas
Presentation: Mass effects without hormone excess
Visual symptoms: Bitemporal hemianopia (optic chiasm compression)
Headaches: From sellar expansion
Hypopituitarism: From compression of normal tissue
Diagnosis:
MRI showing pituitary mass
Normal hormone levels (or hypopituitarism)
Visual field testing
Treatment:
Surgery: For mass effects or visual symptoms
Observation: For small, asymptomatic adenomas
Hormone replacement: For resulting deficiencies
Craniopharyngioma
Bimodal age distribution: Children (6-14 years) and adults (50-60 years) Clinical features:
Children: Growth retardation, delayed puberty
Adults: Visual field defects, hypopituitarism
Both: Headaches, diabetes insipidus
Imaging: Calcified cystic mass, often suprasellar Treatment: Surgery ± radiation (high recurrence risk)
High-Yield Clinical Vignettes for Exams
Vignette 1: The Enlarged Hands
A 45-year-old construction worker notices his work gloves no longer fit. His wife says his facial features have changed over 3 years. He has new-onset diabetes and sleep apnea. Physical exam shows enlarged hands, prognathism, and coarse facial features. Answer: Acromegaly. Next step: IGF-1 level and glucose suppression test.
Vignette 2: The Missing Period
A 28-year-old woman has not had periods for 8 months and notices milky discharge from her breasts. She is not pregnant. She takes no medications except over-the-counter antacids. Answer: Prolactinoma. Next step: Serum prolactin and MRI pituitary.
Vignette 3: The Postpartum Problem
A 32-year-old woman develops fatigue and inability to breastfeed after a delivery complicated by massive postpartum hemorrhage requiring multiple transfusions. She also has not resumed menstruation 6 months postpartum. Answer: Sheehan syndrome. Next step: Full pituitary hormone panel.
Vignette 4: The Thirsty Patient
A 25-year-old man presents with urinating 8 liters per day and constant thirst after a motorcycle accident with head trauma 2 weeks ago. Serum sodium is 148 mEq/L, urine specific gravity is 1.002. Answer: Central diabetes insipidus. Next step: Water deprivation test and trial of desmopressin.
Diagnostic Tests: Stimulation vs Suppression
Understanding when to stimulate vs suppress is crucial for both exams:
Stimulation Tests (Test for Deficiency)
GH deficiency: Insulin tolerance test, arginine stimulation
ACTH deficiency: Cosyntropin stimulation test
GnRH deficiency: GnRH stimulation test
Suppression Tests (Test for Excess)
GH excess: Glucose suppression test
ACTH excess: Dexamethasone suppression tests
Prolactin excess: Usually direct measurement sufficient
Key Drugs in Pituitary Disorders
Drug | Mechanism | Primary Use | Key Side Effects |
|---|---|---|---|
Cabergoline | Dopamine agonist | Prolactinoma | Cardiac valvulopathy (high doses) |
Octreotide | Somatostatin analog | Acromegaly | GI upset, gallstones |
Desmopressin | Synthetic ADH | Central DI | Hyponatremia, water intoxication |
Ketoconazole | Blocks cortisol synthesis | Cushing disease | Hepatotoxicity |
Metyrapone | Blocks 11β-hydroxylase | Cushing disease | Hypertension, hirsutism |
Leveraging Oncourse AI for Pituitary Mastery
Pituitary disorders are notorious for their overlapping presentations and complex hormone interactions. This is where Oncourse AI's specialized tools become invaluable:
Mnemonics for hormone chaos: The Daily Mnemonic Challenge generates interactive puzzles that encode all six anterior pituitary hormones and their target organs in memorable patterns. Instead of struggling to recall "GH, TSH, ACTH, FSH, LH, PRL" during exams, you'll have a systematic retrieval strategy. Real-time feedback loop clarification: Use Rezzy AI while studying to generate custom flowcharts explaining why Cushing disease has elevated ACTH but Cushing syndrome from adrenal tumors has suppressed ACTH. Ask specific questions like "explain the dexamethasone suppression test for someone who keeps confusing high-dose vs low-dose" — Rezzy adapts the explanation to your exact confusion point. Competitive recall training: The Probe Game challenges you to beat an AI opponent in recalling drug-disorder associations under time pressure. When you lose to the AI on "octreotide is used for...", that's evidence-based identification of your weak spots — not the false confidence of passive re-reading.
Frequently Asked Questions
What's the difference between Cushing disease and Cushing syndrome?
Cushing syndrome is the umbrella term for all causes of excess cortisol. Cushing disease specifically refers to ACTH-secreting pituitary adenomas causing cortisol excess. Think of Cushing disease as a subset of Cushing syndrome.
How do you distinguish central diabetes insipidus from nephrogenic diabetes insipidus?
The water deprivation test followed by desmopressin administration is key:
Central DI: Urine concentrates after desmopressin
Nephrogenic DI: No response to desmopressin
Normal: Urine concentrates during water deprivation (before desmopressin needed)
When should you suspect Sheehan syndrome?
Any woman with postpartum hemorrhage who develops:
1. Inability to breastfeed (earliest sign)
2. Amenorrhea persisting >6 months postpartum
3. Fatigue and weakness
4. Signs of multiple hormone deficiencies
What's the best screening test for acromegaly?
IGF-1 level is the best screening test because it's stable throughout the day (unlike GH which is pulsatile). If IGF-1 is elevated, confirm with glucose suppression test — GH should suppress to <1 ng/mL after 75g glucose load.
How do you manage a prolactinoma in pregnancy?
Microprolactinomas: Usually stop cabergoline, monitor symptoms
Macroprolactinomas: Continue cabergoline if visual symptoms, monitor closely
Surgery: Reserved for significant mass effects unresponsive to medical therapy
What's the urgency order for hormone replacement in panhypopituitarism?
1. Hydrocortisone (life-threatening if missed)
2. Levothyroxine (after ensuring adequate cortisol)
3. Sex hormones (quality of life)
4. Growth hormone (specific indications)
Never start thyroid replacement before ensuring adequate cortisol — it can precipitate adrenal crisis.
---
Pituitary disorders represent the intersection of anatomy, physiology, and clinical reasoning. Master the feedback loops, understand the diagnostic tests, and practice with clinical vignettes — the patterns will become second nature.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG and USMLE Step 1. Download free on Android and iOS.