MRCP Part 2 PACES Preparation 2026: Complete Study Guide — Stations, Marking, and First-Attempt Strategy
Master MRCP PACES with our complete 2026 guide. Learn station breakdowns, marking scheme, common failure points, and proven first-attempt strategies for UK medical graduates.
MRCP Part 2 PACES Preparation 2026: Complete Study Guide — Stations, Marking, and First-Attempt Strategy
You are probably staring at your MRCP Part 2 Written results, feeling that familiar mix of relief and dread. Relief because you passed. Dread because PACES is next.
Here's what most guides wont tell you: PACES isnt harder than Part 2 Written — its completely different. This isnt about memorizing facts anymore. Its about performing clinical medicine under pressure, with real patients, real examiners, and zero room for theoretical knowledge without practical application.
PACES has a 73% first-attempt pass rate in 2026, but that statistic hides the real story. The candidates who fail do so because they treat PACES like an academic exam instead of what it actually is: a clinical performance assessment. They memorize textbook presentations instead of practicing station routines. They focus on rare zebra diagnoses instead of mastering bread-and-butter cases.
This guide treats PACES as what it is — a clinical skills exam where your performance in 125 minutes determines whether you become a UK physician. No theory. No padding. Just the exact stations, marking scheme, and first-attempt strategy that works.
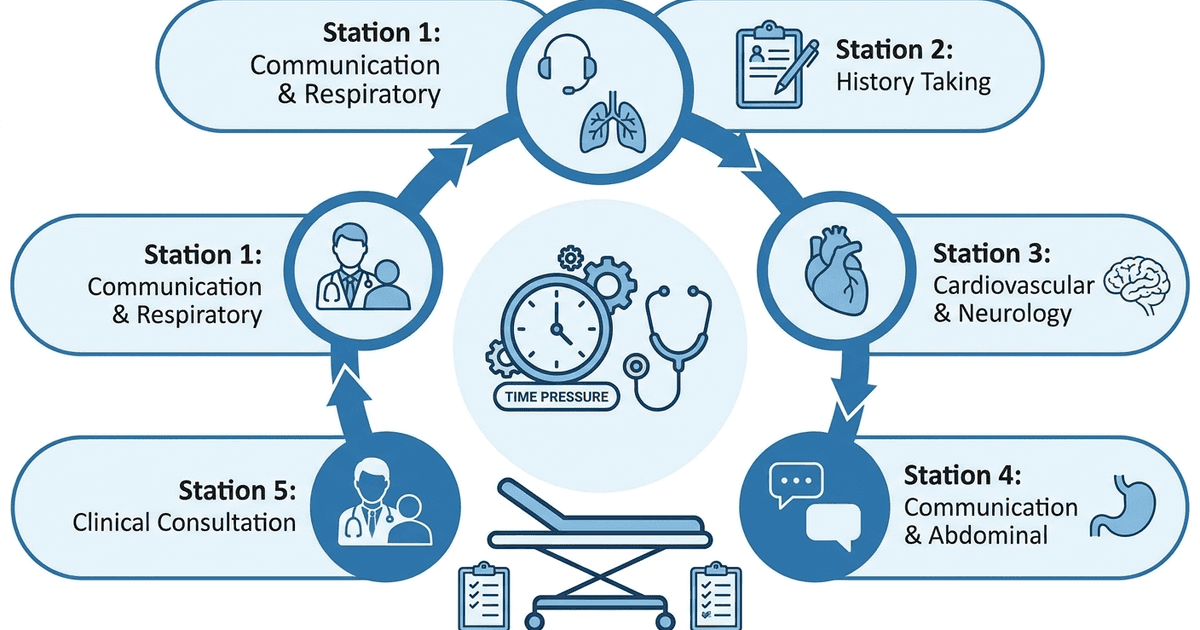
What PACES Actually Tests: The 5-Station Breakdown
PACES uses a carousel format with 5 stations, each lasting exactly 20 minutes. You rotate through all 5 stations regardless of which one you start at. Heres the exact structure you'll face:
Station 1: Respiratory System (10 min) + Communication Skills (10 min)
What happens: You examine a patient with respiratory pathology, then handle a communication scenario with a different patient or surrogate. Common respiratory cases: COPD with cor pulmonale, pulmonary fibrosis, pleural effusion, bronchiectasis, lung consolidation. Forget about rare conditions — 80% of candidates see these five presentations. Communication scenarios: Breaking bad news about lung cancer diagnosis, discussing smoking cessation, explaining CPAP therapy, or addressing family concerns about prognosis. Time management: 6 minutes for examination (including presentation), 4 minutes for questions. Then 8 minutes for communication scenario, 2 minutes for examiner feedback.
Station 2: History Taking Skills (20 min)
What happens: Take a focused history from a real patient, then present your findings and differential diagnosis to examiners. High-yield presentations: Chest pain (think ACS, PE, aortic dissection), breathlessness (heart failure, PE, pneumonia), collapse/syncope, headache with red flags, abdominal pain with systemic features. Structure: 14 minutes with patient, 1 minute to organize thoughts, 5 minutes presenting to examiners with Q&A. Common failure point: Candidates spend too long on social history and miss the clinical red flags that matter.
Station 3: Cardiovascular System (10 min) + Neurological System (10 min)
What happens: Two separate 10-minute clinical examinations with different patients. Cardiovascular bread-and-butter: Mitral regurgitation, aortic stenosis, hypertrophic cardiomyopathy, prosthetic valve, heart failure signs. The murmur you hear is usually obvious — dont overthink it. Neurological staples: Cerebellar syndrome, multiple sclerosis, peripheral neuropathy, stroke with residual signs, Parkinsons disease. Visual field defects and cranial nerve palsies are exam favorites. Critical insight: Both examinations follow the same 6-minute rule — inspect, examine systematically, present findings, answer 2-3 questions.
Station 4: Communication Skills (10 min) + Abdominal System (10 min)
What happens: Handle a communication scenario first, then examine an abdominal patient. Communication scenarios: Discussing treatment options for newly diagnosed diabetes, explaining the need for liver biopsy, addressing family concerns about elderly parent's capacity, breaking news about treatment failure. Abdominal cases: Hepatomegaly (usually chronic liver disease), splenomegaly, ascites, polycystic kidney disease, inflammatory bowel disease with systemic signs. Pro tip: The abdominal examination patient often has obvious signs you can see before touching them — jaundice, spider naevi, gynaecomastia, or visible masses.
Station 5: Brief Clinical Consultation (20 min)
What happens: Two separate 10-minute consultations where you take focused histories and provide immediate management advice. Typical scenarios: Acute medical presentations requiring immediate decision-making — acute chest pain in ED, sudden onset headache, acute shortness of breath, drug overdose, acute confusion in elderly patient. Key difference from Station 2: These are acute scenarios requiring urgent clinical decisions, not detailed differential diagnoses. Time split: 7 minutes taking history and focused examination, 3 minutes discussing immediate management and next steps.
The PACES Marking Scheme: How to Actually Pass
PACES uses 7 skill domains, and you must pass ALL of them plus achieve an overall score of 126/168. Heres the breakdown that matters:
Skill A: Physical Examination Skills (Pass mark: 16/24)
What this tests: Your examination technique, not your diagnostic accuracy. Common failures: Poor patient positioning, inadequate exposure, missing basic inspection signs. Strategy: Perfect your examination routine until its automatic. Clinical Rounds lets you practice structured clinical cases that mirror PACES examination scenarios — work through presenting complaints, gather relevant history, and interpret findings under time pressure.
Skill B: Identifying Physical Signs (Pass mark: 14/24)
What this tests: Recognizing abnormal physical findings correctly. Common failures: Reporting findings that arent there, missing obvious signs during inspection. Critical point: This has the lowest pass rate (66%). Only report signs youre confident about.
Skill C: Clinical Communication Skills (Pass mark: 11/16)
What this tests: How you interact with patients and handle difficult conversations. Common failures: Using medical jargon, not checking patient understanding, rushing through explanations. Strategy: Use chunk-and-check method — give information in small pieces, then ask "Does that make sense?" before continuing.
Skill D: Differential Diagnosis (Pass mark: 15/24)
What this tests: Your clinical reasoning and most likely diagnoses. Common failures: Generic differential lists, not tailoring to the specific clinical scenario. Pro approach: Always lead with the most likely diagnosis based on your findings, then add 2-3 relevant alternatives.
Skill E: Clinical Judgement (Pass mark: 20/32)
This is the highest-weighted skill: Your ability to prioritize investigations and management. Common failures: Ordering every possible test, not considering urgency or practicality. Strategy: Think like an FY2 — what would you actually do first in this clinical situation?
Skill F: Managing Patients' Concerns (Pass mark: 10/16)
What this tests: Addressing what patients are actually worried about. Common failures: Focusing on medical facts while ignoring patient's emotional concerns. Key technique: Always ask "What concerns you most about this?" and address those specific worries.
Skill G: Maintaining Patient Welfare (Pass mark: 28/32)
Highest pass rate skill: Basic professional behavior and patient safety. Common failures: Not checking if examination causes pain, poor privacy/dignity, rushing patients. Non-negotiable: Always ask "Is this comfortable?" during examinations and adjust immediately if not.
Station-by-Station Failure Points and How to Avoid Them
Communication Stations (1 and 4): Where 40% of Marks Live
Biggest mistakes:
Opening with closed questions instead of exploring patient concerns
Using medical jargon without checking understanding
Not addressing the emotional impact of diagnoses
Failing to involve family when appropriate
Winning approach:
Start with "Tell me what you understand about your condition"
Use ICE framework (Ideas, Concerns, Expectations) for every communication
For breaking bad news, use SPIKES model but adapt to time constraints
Always end with "What questions do you have?" not "Do you have questions?"
Practice insight: Use Rezzy to explore ethical principles behind common PACES communication scenarios. Ask Rezzy to explain the reasoning behind breaking bad news protocols or capacity assessments — understanding the why makes your responses more natural than memorizing scripts.
History Taking Station (2 and 5): Time Management Critical
Biggest mistakes:
Spending 5+ minutes on background when the diagnosis is in the first 2 minutes
Not exploring red flag symptoms thoroughly
Poor presentation structure to examiners
Winning structure:
Minutes 1-3: History of presenting complaint with red flag questions
Minutes 4-6: Relevant past medical history and medications
Minutes 7-10: Social history only if relevant to diagnosis
Minutes 11-14: Systems review focused on differential
Minute 14: Organize your presentation mentally
Clinical reasoning shortcut: For chest pain, your first question should be "Can you describe exactly what the pain felt like?" The answer immediately narrows your differential more than 10 minutes of detailed background.
Examination Stations (1, 3, 4): Perfect Your Routine
Biggest mistakes:
Not positioning patients correctly (especially abdominal examinations)
Missing inspection signs because you rush to palpation
Reporting normal findings as abnormal under pressure
Universal examination structure:
Introduce yourself and explain what you'll do
Position patient correctly BEFORE starting
Inspection for 30 seconds minimum — this is where most diagnoses live
Systematic examination with running commentary
Present findings clearly: "On examination, I found..."
Memory aid: Practice your examination sequence until muscle memory takes over. Synapses spaced repetition flashcards help build instant recall of examination findings and normal vs abnormal signs, reducing the cramming that trips candidates up in pressure situations.
Time Management Inside the Exam
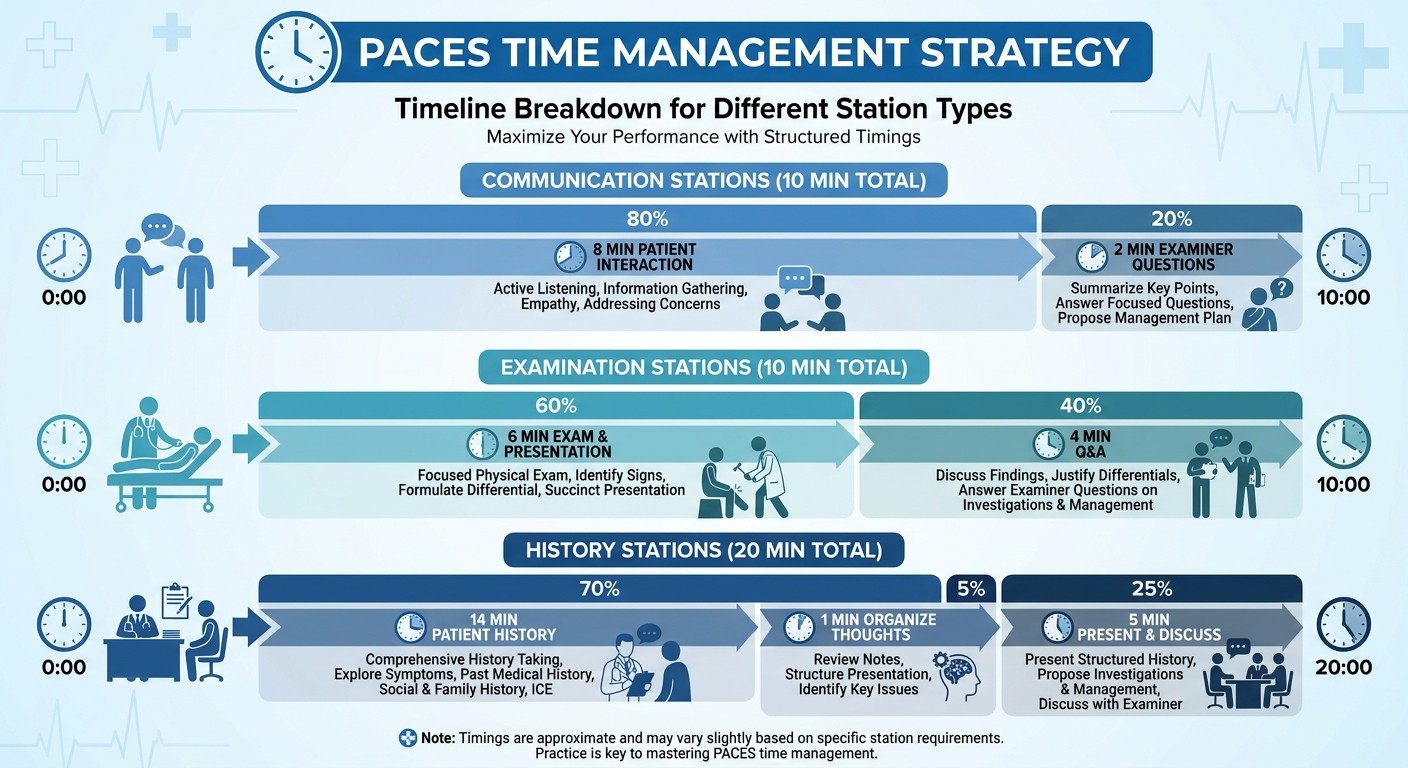
PACES timing is unforgiving. Theres no extra time, no extensions, and no second chances if you run over. Heres how successful candidates pace each station type:
20-Minute Single Stations (2 and 5)
Minutes 1-14: Patient interaction (history taking, focused examination) Minute 15: Organize your thoughts — write down 3 key findings and your top diagnosis Minutes 16-20: Present to examiners and handle Q&A Critical rule: Never spend more than 14 minutes with the patient, even if they keep talking. Politely interrupt: "Thank you, let me just clarify a few key points before we finish."
10+10 Split Stations (1, 3, 4)
Each 10-minute segment follows the same pattern: Minutes 1-6: Clinical activity (examination or communication) Minutes 7-10: Questions and discussion with examiners Transition management: You get exactly 30 seconds between the two parts of each station. Use this to reset mentally — the second part is completely independent.
The 5-Minute Reading Break
Before stations 2, 4, and 5, you get 5 minutes to read the clinical scenario. This is where PACES is won or lost.
Reading strategy:
Minute 1: Read scenario twice, noting patient age, key symptoms, and setting
Minutes 2-3: Plan your opening questions based on most likely diagnoses
Minutes 4-5: Anticipate examiner questions and prepare your structured approach
Common mistake: Trying to memorize every detail instead of identifying the most likely clinical problem.
8-12 Week Preparation Strategy for First-Attempt Success
Phase 1: Foundation Building (Weeks 1-4)
Week 1-2: Master basic examination techniques for all systems
Practice examination routines daily until automatic
Record yourself examining friends/family to identify timing issues
Focus on positioning, exposure, and systematic approach
Week 3-4: Build pattern recognition for common cases
Study high-yield cases: top 5 presentations per system
Use clinical images and videos for visual sign recognition
Practice differential diagnosis frameworks for each presentation
Clinical insight: During this phase, use structured case practice to build the mental framework PACES demands. Work through presenting complaints systematically, gathering relevant history and interpreting findings — exactly what the examination stations require.
Phase 2: Station-Specific Skills (Weeks 5-8)
Week 5-6: Communication and ethics mastery
Practice breaking bad news scenarios with structured frameworks
Master ICE and SPIKES techniques with real timing constraints
Record practice sessions to identify filler words and unclear explanations
Week 7-8: History taking and presentation skills
Practice 20-minute history scenarios with strict timing
Develop concise presentation style (2 minutes maximum)
Learn to interrupt politely when patients go off-track
Ethical reasoning practice: When preparing communication scenarios, dont just memorize scripts. Use AI tutoring to understand the ethical principles behind difficult conversations — why certain approaches work better for capacity assessments or end-of-life discussions. This deeper understanding makes your responses more natural under pressure.
Phase 3: Exam Simulation (Weeks 9-12)
Week 9-10: Full PACES simulation
Complete 5-station carousel practice with timing
Get feedback from different examiners to adapt to various styles
Practice transitioning between stations without losing focus
Week 11-12: Fine-tuning and confidence building
Focus on weak areas identified during simulations
Practice presenting under pressure with hostile questioning
Maintain clinical exposure to stay sharp with real patients
Memory consolidation: Throughout this phase, use spaced repetition to keep all station types fresh simultaneously. Build targeted flashcard sets for each station (respiratory signs, cardiovascular findings, neurological examination) and run daily 10-minute reviews to prevent knowledge fade.
Daily Practice Schedule (Final 4 Weeks)
Monday: Full station simulation (2 hours) Tuesday: Communication skills practice (1 hour) Wednesday: Examination technique refinement (1 hour) Thursday: History taking and presentation (1 hour) Friday: Mixed practice and weak area focus (1 hour) Saturday: Mock PACES with feedback (3 hours) Sunday: Review and mental preparation (30 minutes)
Common Mistakes That Cause First-Attempt Failures
The "Rare Disease" Trap
What happens: Candidates study zebra diagnoses and miss obvious horses. Reality check: 90% of PACES cases are common conditions presenting typically. Fix: Spend 80% of study time on the top 5 cases per station, 20% on everything else.
The "Perfect Textbook Answer" Mistake
What happens: Giving comprehensive differential lists instead of focused clinical reasoning. What examiners want: "Based on this 65-year-old smoker with clubbing and coarse crackles, I think this is bronchiectasis. The main alternatives would be..." Fix: Always lead with your most likely diagnosis, then add 2-3 relevant alternatives.
The Communication Jargon Barrier
What happens: Using medical terms without checking patient understanding. Example failure: "You have acute ST-elevation myocardial infarction requiring primary PCI." Winning version: "You've had a heart attack. That means one of the blood vessels to your heart was blocked. The good news is we can open it up with a procedure. Let me explain what that involves..."
The Time Management Disaster
What happens: Running out of time because you dont track minutes actively. Reality: PACES examiners will interrupt you mid-sentence when time expires. Fix: Wear a watch and check it every 2-3 minutes. Practice with strict timing until its second nature.
The Examination Technique Breakdown
What happens: Forgetting basic clinical skills under pressure. Most common: Not lying patient flat for abdominal examination, missing inspection phase, poor auscultation technique. Fix: Practice examination sequences until theyre automatic, even when nervous.
What Distinguishes Passers from Repeaters
Passers Think Like Clinicians, Repeaters Think Like Students
Passers: Focus on what they would actually do as an FY2 in this clinical situation Repeaters: Try to demonstrate everything they know about the condition
Passers Adapt, Repeaters Stick to Scripts
Passers: Modify their approach based on patient responses and examiner cues Repeaters: Follow memorized frameworks regardless of context
Passers Practice Performance, Repeaters Study Content
Passers: Spend 70% of time practicing stations, 30% learning facts Repeaters: Spend 70% time reading, 30% practicing actual PACES skills
Passers Master Time, Repeaters Fight Time
Passers: Work within time constraints and finish all required elements Repeaters: Run out of time because they dont practice with strict timing
First-Attempt Strategy: The 48-Hour Pre-Exam Protocol
48 Hours Before: Final Preparation
Review high-yield examination findings using flashcard rotation
Practice one complete 5-station simulation
Confirm exam location, travel plans, and required documentation
Stop learning new material — focus on consolidating existing knowledge
24 Hours Before: Mental Preparation
Light review of communication frameworks only
Ensure good sleep (aim for 8 hours)
Avoid discussing PACES with other candidates
Pack exam essentials: photo ID, watch, professional attire
Exam Morning: Performance Mode
Arrive 30 minutes early to settle nerves and complete registration
During the briefing, listen for any station-specific instructions
Between stations, take three deep breaths and reset mentally
Trust your preparation — dont second-guess clinical decisions
During Each Station: Execution
Read scenarios carefully and identify the key clinical question
Use the first 30 seconds to organize your approach
Stay within time limits even if it feels rushed
Answer examiner questions directly — dont elaborate unless asked
Frequently Asked Questions
How many months should I prepare for PACES?
Most successful first-attempt candidates prepare for 8-12 weeks with dedicated clinical practice. You need time to build muscle memory for examination techniques and develop confidence with communication scenarios.
What happens if I fail one skill but pass everything else?
You fail the entire exam. PACES requires passing all 7 skills AND achieving the overall pass mark of 126/168. This is why balanced preparation across all stations is essential.
Can I use my own stethoscope in PACES?
Yes, bring your own stethoscope if you prefer it. However, centers provide standard equipment, so dont worry if you forget yours. If you need specialized equipment (like an amplifying stethoscope), declare this during registration.
How much clinical experience do I need before attempting PACES?
While theres no minimum requirement, successful candidates typically have at least 6-12 months of UK clinical experience. The exam tests practical skills that develop through patient contact, not textbook reading.
What should I do if a patient becomes unwell during my station?
Stop your examination immediately and alert the examiners. Patient safety always comes first in PACES. This demonstrates Skill G (Maintaining Patient Welfare) and wont count against you.
Is the marking different for international medical graduates?
No, all candidates are marked using the same criteria and pass marks. However, international graduates often need extra practice with UK clinical communication styles and NHS-specific scenarios.
PACES rewards clinical competence, not theoretical knowledge. The candidates who pass first attempt treat it as a performance exam where technique, timing, and patient interaction matter more than encyclopedic medical knowledge.
Master your examination routines until theyre automatic. Practice communication scenarios until you can handle difficult conversations naturally. Develop clinical reasoning that focuses on practical next steps, not academic differential lists.
Most importantly, remember that PACES tests the skills you need as a UK physician. Every station reflects situations you'll encounter regularly in clinical practice. The better you become at PACES, the better doctor you'll be.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for MRCP success. Download free on Android and iOS.