

Diagnosis & Screening - Spotting the Signs
- Screening Tools: CAGE questionnaire (quick), AUDIT-C (more sensitive).
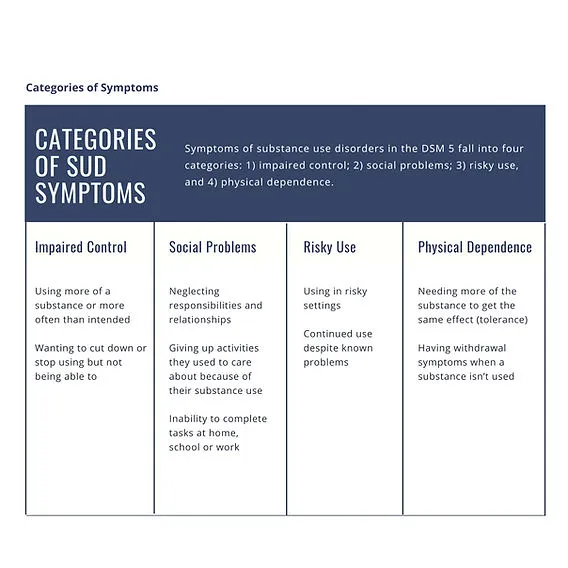
- DSM-5 Criteria: Problematic pattern of use with impairment, requiring ≥2 of 11 criteria in 12 months.
- Categories: Impaired control, social impairment, risky use, and pharmacological (tolerance/withdrawal).
- Biomarkers:
- ↑ GGT (gamma-glutamyl transferase) - most sensitive marker.
- ↑ AST:ALT ratio (typically >2:1).
- ↑ MCV (macrocytosis).
⭐ An AST:ALT ratio >2 is highly suggestive of alcoholic hepatitis.
Acute Intoxication - The Tipsy Turmoil
- Pathophysiology: Potentiates GABA-A receptors (inhibitory) & inhibits NMDA receptors (excitatory), causing widespread CNS depression.
- Clinical Features:
- Slurred speech, ataxia, incoordination, nystagmus.
- Disinhibition, impaired judgment, blackouts.
- Diagnosis: Clinical; serum ethanol level correlates poorly with impairment due to tolerance.
- Management: Supportive care, monitor vitals and glucose.
⭐ In suspected chronic alcohol use, always give thiamine before glucose to prevent precipitating Wernicke-Korsakoff syndrome.
Alcohol Withdrawal - The Shakes & Quakes
Pathophysiology: Chronic EtOH use → ↓ GABAergic tone & ↑ NMDA receptor activity. Cessation causes CNS hyperexcitation.

- Management:
- Benzodiazepines (Chlordiazepoxide, Diazepam, Lorazepam) guided by CIWA-Ar scale.
- Give Thiamine (B1) before glucose to prevent Wernicke's encephalopathy.
⭐ In liver failure, use LOT: Lorazepam, Oxazepam, Temazepam, as they are metabolized outside the liver.
Chronic Complications - The Body's Toll
- Neurologic: Wernicke-Korsakoff syndrome (thiamine deficiency), cerebellar degeneration (ataxia), peripheral neuropathy.
- Cardiovascular: Dilated cardiomyopathy, hypertension, atrial fibrillation.
- Gastrointestinal:
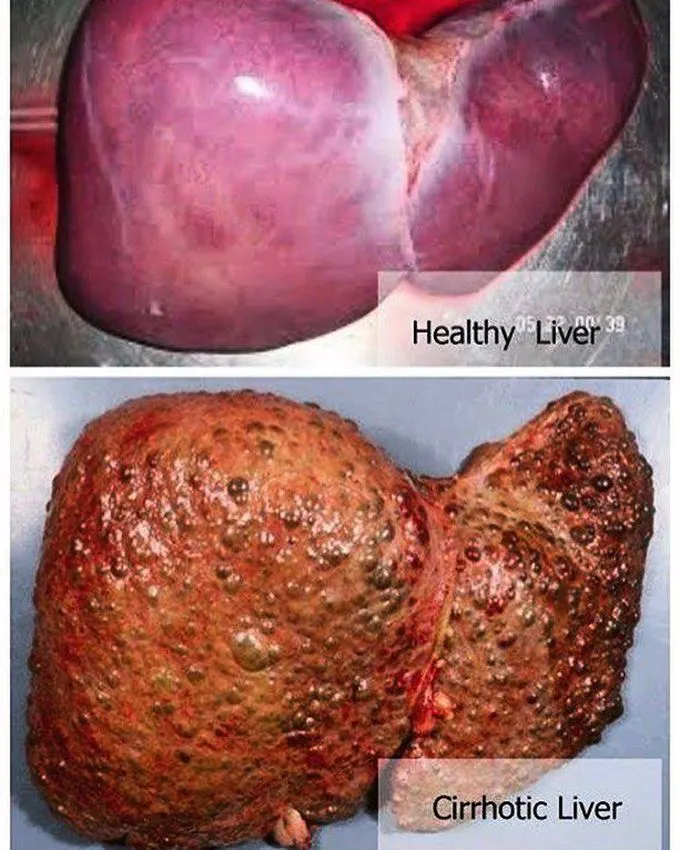
- Liver: Steatosis → Alcoholic Hepatitis → Cirrhosis
- Pancreatitis (acute & chronic)
- Gastritis, Mallory-Weiss tears
- Hematologic: Macrocytosis (↑ MCV), thrombocytopenia.
- Endocrine: Gynecomastia, testicular atrophy.
⭐ Wernicke's encephalopathy presents with a classic triad: Confusion, Ophthalmoplegia (e.g., nystagmus), and Ataxia (mnemonic: COAt). Always give thiamine before glucose to prevent precipitating the syndrome.
Management - The Recovery Roadmap
- Pharmacotherapy is key to preventing relapse.
- Naltrexone: ↓ cravings & rewarding effects. Oral or long-acting injection.
- Acamprosate: Modulates glutamate, good for maintaining abstinence. Requires 3x/day dosing.
- Disulfiram: Aversive agent. Causes nausea/vomiting with alcohol. Requires high motivation.
⭐ Naltrexone is contraindicated in patients taking opioids (can precipitate withdrawal) and those with acute hepatitis or liver failure.
High‑Yield Points - ⚡ Biggest Takeaways
- CAGE questionnaire is the key screening tool.
- Withdrawal is life-threatening; it starts with tremors and can progress to seizures, hallucinosis, and delirium tremens (DTs).
- Treat acute withdrawal with benzodiazepines (e.g., lorazepam).
- Maintenance therapy includes naltrexone (reduces cravings) and acamprosate.
- Disulfiram creates an aversive reaction to alcohol.
- Always give thiamine before glucose to prevent precipitating Wernicke-Korsakoff syndrome.
- Lab findings often show ↑GGT, ↑AST > ↑ALT (2:1 ratio), and macrocytosis.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more