

ECG Ischemia Basics - The Silent Scream
Myocardial ischemia from ↓ coronary blood flow creates a spectrum of ECG changes reflecting cellular distress. The location and duration of ischemia determine the pattern.
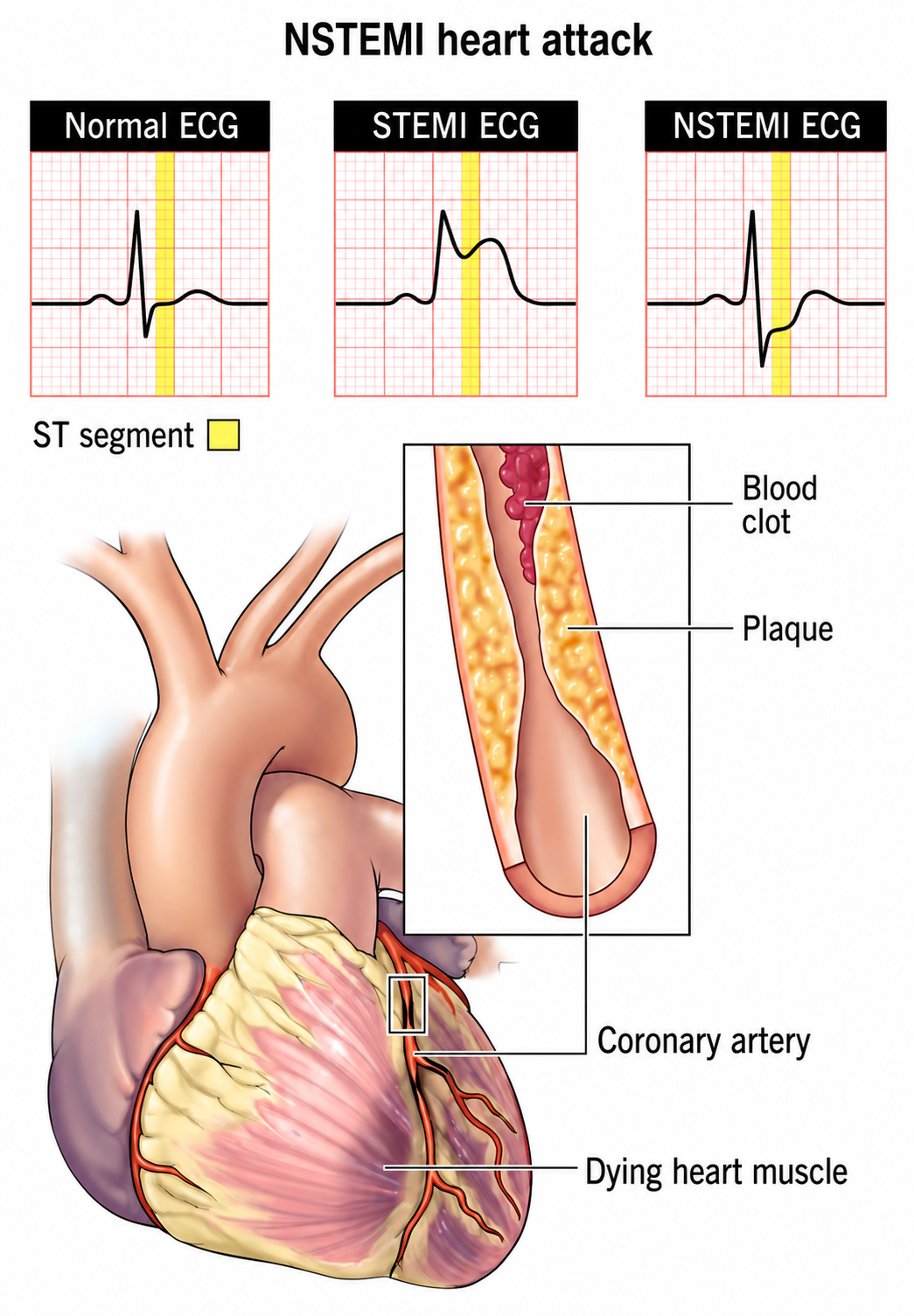
- Subendocardial (NSTEMI): Affects inner myocardial layer. Manifests as ST-segment depression or T-wave inversion.
- Transmural (STEMI): Involves the entire myocardial wall. Causes ST-segment elevation, the hallmark of acute injury.
Loading diagram…
⭐ De Winter's T-waves (tall, prominent, symmetric T-waves in precordial leads) are a STEMI equivalent for acute LAD occlusion, even without classic ST elevation.
STEMI vs. NSTEMI - The Great Divide
- Pathophysiology: The core difference lies in the degree of coronary artery occlusion.
| Feature | STEMI (ST-Elevation MI) | NSTEMI (Non-ST-Elevation MI) |
|---|---|---|
| Vessel Blockage | 100% occlusive thrombus | Subtotal occlusion; severe stenosis |
| Infarction | Transmural (full thickness) | Subendocardial (partial thickness) |
| ECG | ST-segment elevation (new) | ST depression, T-wave inversion |
| Biomarkers | ↑ Troponins | ↑ Troponins |
| Immediate Goal | Emergent Reperfusion | Anti-ischemic therapy, risk stratify |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||
| flowchart TD | ||
| START["🩺 Chest Pain • ACS symptoms• Acute presentation"] |
ECG["🔬 12-Lead ECG
• Perform stat• Evaluate rhythm"]
DECISION["📋 ST Elevation?
• Assess segments• Check leads"]
STEMI["⚠️ STEMI
• Activate Cath Lab• Emergent reperfusion"]
NSTEMI["🩺 NSTEMI / UA
• Unstable Angina• Check Troponins"]
START --> ECG ECG --> DECISION DECISION -->|Yes| STEMI DECISION -->|No| NSTEMI
style START fill:#F7F5FD,stroke:#F0EDFA,stroke-width:1.5px,rx:12,ry:12,color:#6B21A8 style ECG fill:#FFF7ED,stroke:#FFEED5,stroke-width:1.5px,rx:12,ry:12,color:#C2410C style DECISION fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E style STEMI fill:#FDF4F3,stroke:#FCE6E4,stroke-width:1.5px,rx:12,ry:12,color:#B91C1C style NSTEMI fill:#F7F5FD,stroke:#F0EDFA,stroke-width:1.5px,rx:12,ry:12,color:#6B21A8
> ⭐ **Exam Favorite:** In STEMI, "time is muscle." The primary goal is immediate reperfusion, typically via percutaneous coronary intervention (PCI) within **90 minutes** of first medical contact. This is the most critical management step.
## Infarct Location - Pinpointing the Problem
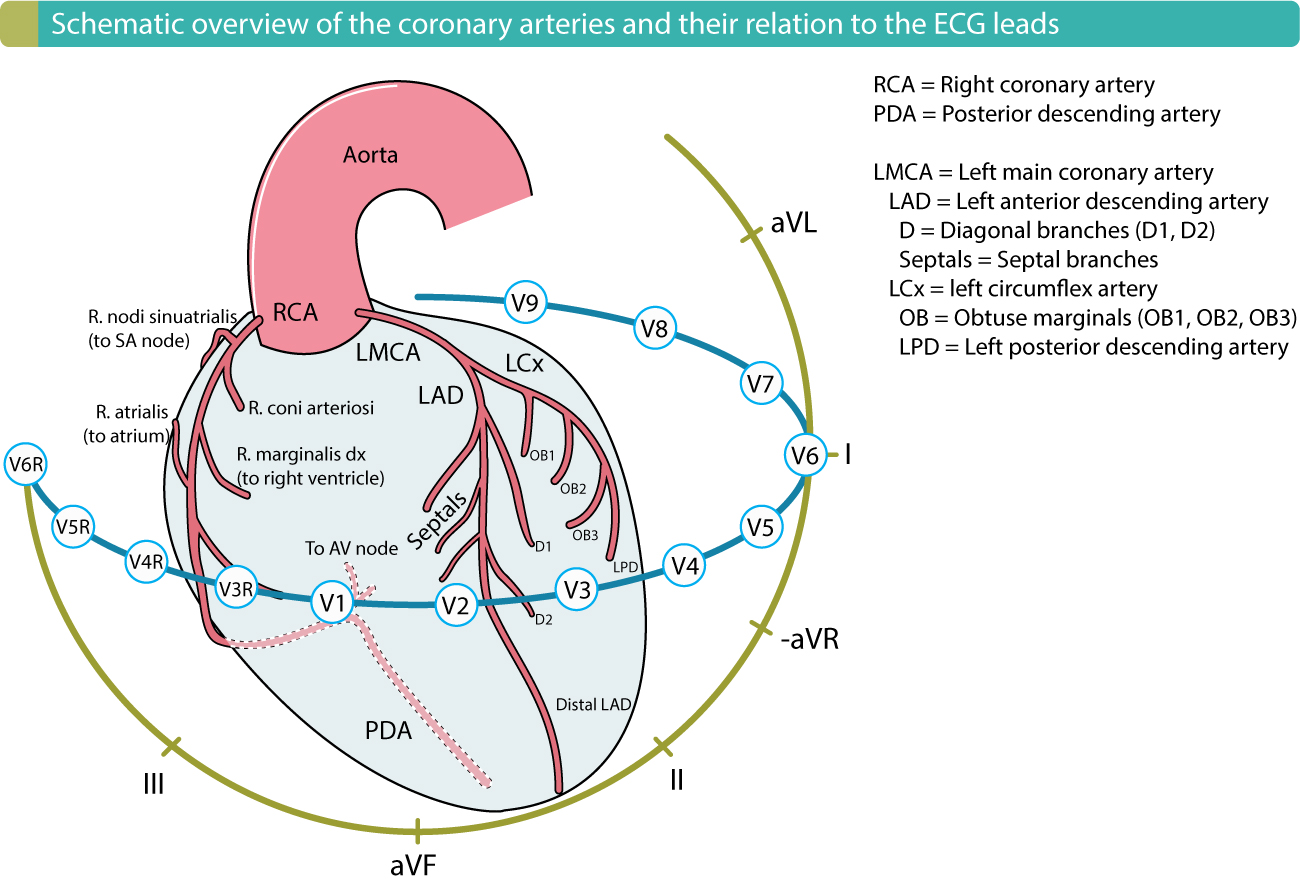
* **ST elevation** in specific lead groups localizes the myocardial injury.
* Look for **reciprocal ST depression** in opposing leads.
| Infarct Location | Leads with ST Elevation | Artery Involved |
| :--- | :--- | :--- |
| **Anteroseptal** | V1-V4 | Left Anterior Descending (LAD) |
| **Lateral** | I, aVL, V5-V6 | Left Circumflex (LCX) |
| **Inferior** | II, III, aVF | Right Coronary Artery (RCA) |
| **Posterior** | ST depression V1-V3, Tall R | Posterior Descending Artery (PDA) |📌 **Mnemonic:**
- **L**ateral: **I**, a**VL**, V5, V6 (Use the "L" in aVL)
- **I**nferior: **II**, **III**, aV**F** (Use the "F" in aVF for "Feet")
> ⭐ **Reciprocal Changes:** An inferior wall MI (↑ST in II, III, aVF) often shows reciprocal ST depression in lateral leads (I, aVL). This pattern strongly confirms the diagnosis of an acute infarction.
## MI Timeline - A Scar is Born
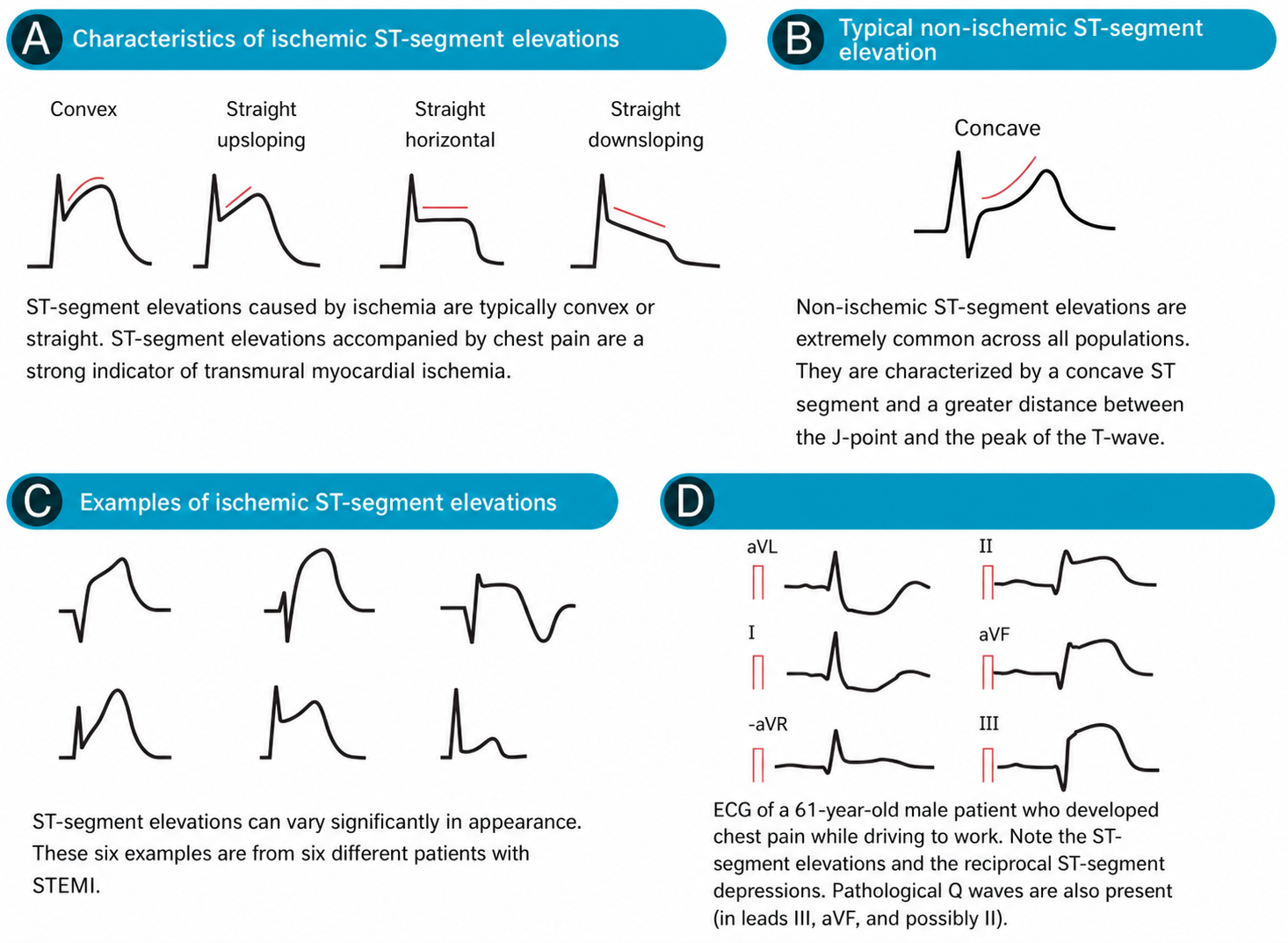
* **Acute (0-12 hrs):** Begins with hyperacute, peaked T-waves, followed by marked ST-segment elevation, indicating transmural injury. Reciprocal ST-depression may be present.
* **Evolving (Hours-Days):** ST-elevation diminishes. Pathological Q-waves (>**0.04s**, >**25%** of R-wave height) develop, and T-waves invert, signifying necrosis and ischemia.
* **Chronic (Weeks-Years):** ST segments and T-waves often normalize. The pathological Q-wave persists indefinitely as electrical evidence of the fibrous scar.
> ⭐ Persistent ST-elevation for several weeks post-MI strongly suggests the formation of a ventricular aneurysm.
> * **ST-segment elevation (STE)** in contiguous leads signifies an **acute transmural injury (STEMI)**.
> * **ST depression** and **T-wave inversion** are classic signs of **subendocardial ischemia**.
> * The presence of **pathological Q waves** indicates a **prior or old infarction**.
> * Always look for **reciprocal changes** (i.e., ST depression) in anatomically opposite leads.
> * **Anterior MI**: STE in **V1-V4**; **Inferior MI**: STE in **II, III, aVF**; **Lateral MI**: STE in **I, aVL, V5-V6**.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more