

Opioid MOA & Receptors - The Brain's Bliss Buttons
- Receptors: Opioids are agonists at three main G-protein coupled receptors (GPCRs): Mu (μ), Delta (δ), and Kappa (κ).
- Cellular MOA: They act on both presynaptic and postsynaptic neurons.
- ↓ Presynaptic Ca²⁺ influx → ↓ release of neurotransmitters (e.g., Substance P, glutamate).
- ↑ Postsynaptic K⁺ efflux → hyperpolarization → ↓ neuronal signaling.
- Key Receptor Functions:
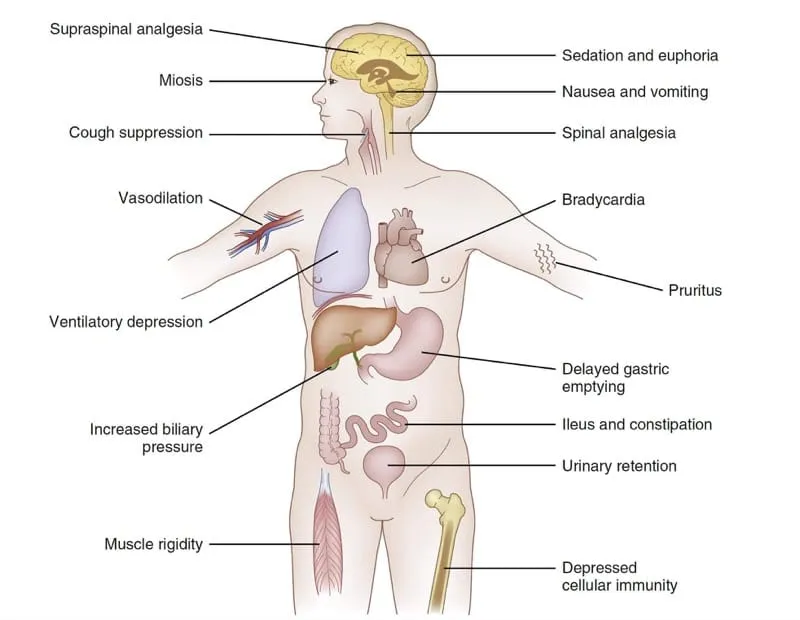
- μ (Mu): Analgesia, euphoria, respiratory depression, miosis, constipation. 📌 Mu = Most effects.
- κ (Kappa): Spinal analgesia, sedation, miosis.
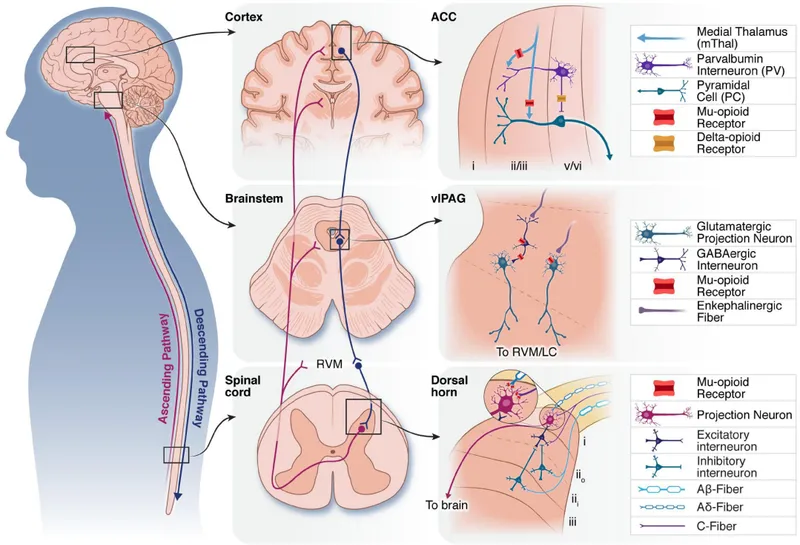
⭐ Opioids primarily exert their powerful analgesic effects by acting on μ-receptors in the spinal cord (substantia gelatinosa) and supraspinal sites (e.g., periaqueductal gray).
Opioid Classification - The Agonist & Antagonist Cast
| Class | Mechanism & Key Drugs | Clinical Notes |
|---|---|---|
| Full Agonists | Strong μ-receptor agonists providing maximal analgesia. | Morphine, fentanyl, methadone, meperidine. Used for severe pain; high abuse potential. |
| Partial Agonists | Mixed agonist-antagonist activity; act as agonists at some receptors and antagonists at others. | Buprenorphine (μ-partial agonist, κ-antagonist), nalbuphine, butorphanol. Can precipitate withdrawal in opioid-dependent patients. |
| Antagonists | Competitive antagonists at all opioid receptors; displace agonists to reverse effects. | Naloxone (short-acting for acute overdose), naltrexone (long-acting for relapse prevention). |
Uses & Side Effects - Pain Relief and Its Perils
-
Primary Uses
- Analgesia: Moderate to severe pain.
- Cough suppression (dextromethorphan, codeine).
- Diarrhea treatment (loperamide, diphenoxylate).
- Anesthesia adjunct (fentanyl).
-
Adverse Effects
- CNS: Sedation, euphoria, miosis (pinpoint pupils).
- Respiratory: ↓ Respiratory rate & depth.
- GI: Nausea, vomiting, constipation (no tolerance).
- CV: Hypotension, bradycardia.
- GU: Urinary retention.
- Skin: Pruritus (histamine release).
- Tolerance and physical dependence with long-term use.
⭐ Opioid Overdose Triad: Coma, respiratory depression, and pinpoint pupils (miosis). Treat with naloxone.
Overdose & Withdrawal - When The Bliss Ends
- Overdose Triad: Coma, respiratory depression, miosis (pinpoint pupils).
- Management: Naloxone (opioid antagonist). Caution: short half-life may require repeat doses.
⭐ Naloxone can precipitate severe, acute withdrawal in opioid-dependent individuals.
- Withdrawal Symptoms: Anxiety, lacrimation, rhinorrhea, yawning, sweating, piloerection ("cold turkey"), mydriasis.
- Treatment: Supportive. Clonidine (↓ autonomic hyperactivity). For long-term detox: methadone (long-acting agonist) or buprenorphine (partial agonist).
High‑Yield Points - ⚡ Biggest Takeaways
- Opioids bind to μ, δ, and κ receptors, causing analgesia, euphoria, and sedation.
- The classic triad of opioid toxicity is coma, pinpoint pupils (miosis), and respiratory depression.
- Naloxone is a competitive antagonist used to reverse opioid overdose.
- Tolerance develops to most effects, but not to miosis or constipation.
- Withdrawal is managed with long-acting agents like methadone or buprenorphine.
- Co-administration with other CNS depressants (e.g., benzodiazepines) risks fatal respiratory depression.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more