

Etiology & Genetics - The Extra Chromosome
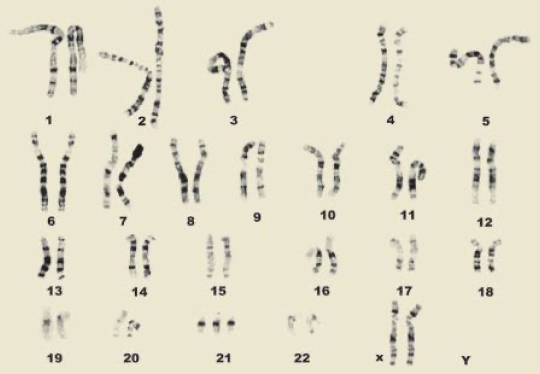
- Trisomy 21: Caused by an extra copy of chromosome 21.
- Primary Mechanism (95%): Meiotic nondisjunction.
- Predominantly due to maternal gamete error (~90%), linked to advanced maternal age.
- Other Mechanisms:
- Robertsonian Translocation (~4%): Unbalanced fusion, e.g., t(14;21). Recurrence risk is high; not age-dependent.
- Mosaicism (~1%): Post-zygotic nondisjunction results in two cell lines. Milder features.
⭐ Risk of Trisomy 21 significantly increases with maternal age >35 years.

Clinical Features - Spotting the Signs
- General: Neonatal hypotonia, poor Moro reflex, joint hypermobility.
- Craniofacial & Neck:
- Flat facial profile, brachycephaly (flat occiput).
- Upslanting palpebral fissures, prominent epicanthic folds.
- Brushfield spots (grey-white spots on iris).
- Small nose with depressed nasal bridge.
- Protruding tongue, high-arched palate.
- Short neck with excess nuchal skin.
- Extremities:
- Single transverse palmar crease (Simian crease).
- Short, broad hands; clinodactyly (incurved 5th finger).
- Wide space between 1st & 2nd toes (Sandal gap).
⭐ The most common associated congenital heart defect is an Atrioventricular Septal Defect (AVSD).
Systemic Associations - The Domino Effect
- Cardiovascular (~50%): Endocardial cushion defect (AVSD) is pathognomonic. Ventricular Septal Defect (VSD) and Atrial Septal Defect (ASD) are also common.
- Gastrointestinal: Duodenal atresia presents with bilious vomiting & the classic "double bubble" sign on X-ray. Also associated with Hirschsprung disease and celiac disease.
- Hematologic: ↑ risk (~20x) of Acute Lymphoblastic Leukemia (ALL). Also, Transient Myeloproliferative Disorder (TMD) in neonates.
- Endocrine: Congenital and acquired hypothyroidism are frequent; regular screening is crucial.
- Musculoskeletal/Neurologic: Atlanto-axial instability (⚠️ screen before anesthesia/sports), generalized hypotonia. Inevitable early-onset Alzheimer's disease.
- Sensory: Brushfield spots in the iris, refractive errors, and congenital cataracts. Chronic ear infections and hearing loss.
⭐ The Amyloid Precursor Protein (APP) gene is located on Chromosome 21, explaining the strong link and early onset of Alzheimer's disease.
Diagnosis & Management - Plan of Action
-
Prenatal Screening:
- 1st Trimester: ↓PAPP-A, ↑β-hCG, ↑Nuchal translucency.
- 2nd Trimester (Quad): ↓AFP, ↓uE3, ↑β-hCG, ↑Inhibin A.
-
Definitive Diagnosis: Karyotyping (postnatal) or CVS/Amniocentesis (prenatal).
-
Anticipatory Guidance & Screening:
Loading diagram…
- **Growth:** Use specific Down syndrome growth charts.
- **Development:** Early intervention programs (Physio, Speech therapy).
⭐ Most common heart defect is Atrioventricular Septal Defect (AVSD). Increased risk (~20x) of Acute Lymphoblastic Leukemia (ALL).
High‑Yield Points - ⚡ Biggest Takeaways
- Trisomy 21 is the most common genetic cause, strongly linked to advanced maternal age.
- Key features include a flat facies, upward-slanting eyes, Brushfield spots, and a single transverse palmar crease.
- Atrioventricular septal defect (AVSD) is the most common and characteristic cardiac anomaly.
- Look for the "double bubble" sign on X-ray, indicating duodenal atresia.
- There's a significantly increased risk of acute leukemias (ALL, AML).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more