

Neuro & Cardiac - Lifelong Watch
-
Neural Tube Defects (e.g., Myelomeningocele)
- Hydrocephalus: Lifelong shunt monitoring (blockage, infection).
- Neurogenic Bladder: Regular renal function tests (RFTs) & ultrasounds; clean intermittent catheterization (CIC) to prevent hydronephrosis.
- Tethered Cord Syndrome: Monitor for new motor/sensory deficits, back pain.
- Orthopedic surveillance for scoliosis, hip dislocation.
-
Congenital Heart Disease (CHD)
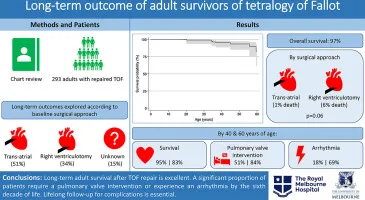
- Post-Repair (e.g., ToF, VSD): Annual cardiology f/u. Monitor for arrhythmias, ventricular dysfunction, residual shunts.
- Infective Endocarditis (IE) Prophylaxis: Required for high-risk patients (prosthetic valves, previous IE, unrepaired cyanotic CHD).
- Eisenmenger Syndrome: Monitor for polycythemia, heart failure. Avoid dehydration & high altitudes.
⭐ Post-ToF Repair: The most common long-term complication leading to re-operation is severe pulmonary regurgitation. The most life-threatening arrhythmia is ventricular tachycardia (VT), a major risk for sudden cardiac death.
GI & GU Issues - Gut Feelings & Flow Problems
-
Gastrointestinal (GI):
- TEF Repair: ↑ risk of GERD, dysphagia, strictures. Needs EGD surveillance.
- Hirschsprung's: Post-op risks include enterocolitis, chronic constipation, incontinence.
- Anorectal Malformations (ARM): Fecal incontinence & constipation are major concerns requiring a bowel management program.
-
Genitourinary (GU):
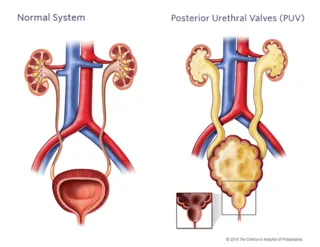
- Posterior Urethral Valves (PUV): High risk of CKD/ESRD. Monitor creatinine, BP. "Valve bladder" causes poor compliance & incontinence.
- Vesicoureteral Reflux (VUR): Risk of recurrent UTIs, renal scarring. DMSA scan assesses scarring.
⭐ Prognostic Pearl: The nadir serum creatinine level at 1 year of age is the best predictor of long-term renal function in boys treated for Posterior Urethral Valves (PUV).
Systemic & Structural - Bones, Syndromes & Beyond
- Osteogenesis Imperfecta (OI): Lifelong fracture risk. Follow-up includes audiology (hearing loss), DEXA scans, and cyclical bisphosphonate therapy (Pamidronate).
- Marfan Syndrome: Regular cardiology for aortic root dilatation (Z-score monitoring). Annual ophthalmology for ectopia lentis. Beta-blockers or ARBs (Losartan) to slow aortic root growth.
- Down Syndrome: Surveillance for hypothyroidism (TSH), atlantoaxial instability (symptom-based screening), and vision/hearing deficits.
- Turner Syndrome: Monitor for coarctation of aorta, bicuspid aortic valve, and renal anomalies. Requires estrogen replacement for puberty & bone health.
⭐ In Down Syndrome, the Amyloid Precursor Protein (APP) gene on Chromosome 21 leads to amyloid plaque deposition, causing a high risk of early-onset Alzheimer's disease (often by age 40).
Growth & Mind - Tracking & Thriving
-
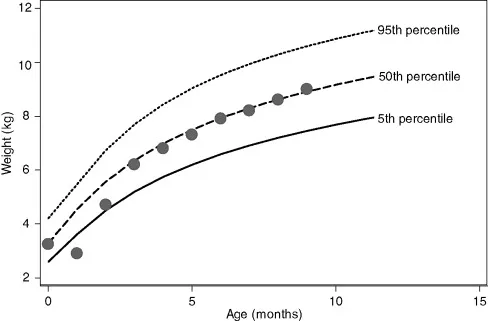
Growth Monitoring: Regular plotting on WHO/IAP growth charts. Crucial for detecting failure to thrive (FTT).
- Red flags: Crossing >2 major centiles, weight-for-height < -2 SD.
- Assess bone age if height is affected.
-
Developmental Surveillance: Screen at every well-child visit. Use standardized tools.
- Domains: Gross Motor, Fine Motor, Language, Social/Cognitive.
- Tools: DDST-II, Trivandrum Development Screening Chart (TDSC).
-
Psychosocial Health: Monitor for behavioral issues, learning disabilities, and social integration challenges. Crucial for quality of life.
⭐ Global Developmental Delay (GDD): Significant delay (≥2 SD below mean) in ≥2 developmental domains in children <5 years old.
High‑Yield Points - ⚡ Biggest Takeaways
- Neurodevelopmental delay is a key long-term risk in major congenital heart and CNS defects.
- Failure to thrive is common in significant cardiac and GI anomalies, needing nutritional support.
- Congenital renal anomalies demand lifelong follow-up for CKD and hypertension.
- Large uncorrected shunts can lead to irreversible pulmonary hypertension (Eisenmenger syndrome).
- SBE prophylaxis is vital for high-risk cardiac lesions, including prosthetic valves and unrepaired cyanotic CHD.
- A planned transition to adult care improves long-term outcomes and adherence.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more